Thomas R. Friberg,
Jenny Y. Yu
INTRODUCTION
Folds of the choroid and retina are typically a sign of an ocular disease or disorder. Choroidal folds develop secondary to biomechanical stresses, for instance, from an extraocular mass in the orbit pressing upon the globe, from thickening of the choroid from hypotony, choroidal effusion, or inflammation, or from stresses secondary to a growing choroidal tumor. Retinal folds may be seen over tight choroidal folds but are more typically a result of proliferation along the superficial retinal layers, such as seen in macular pucker, proliferative retinopathy, or in scarring from choroidal neovascularization (CNV). Both choroidal and retinal folds can be seen upon biomicroscopy but fluorescein angiography outlines choroidal folds most dramatically. Retinal folds, on the other hand, are well demonstrated by optical coherence tomography (OCT) or on high-power biomicroscopy. The clinical presence of choroidal or retinal folds needs to be explained, as the underlying disease which created them may need to be addressed. Both types of folds can be symptomatic with retinal folds creating metamorphopsia. This chapter details the biomechanical principles which create chorioretinal folds so they can be better understood.
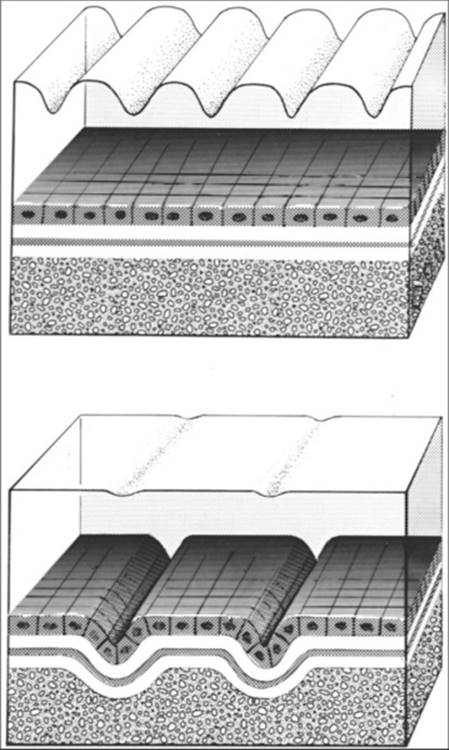
Many disorders are associated with the formation of folds in the choroid and retina. For descriptive purposes, folds primarily involving the choroid, with the overlying retina only secondarily affected, are classified as choroidal folds, whereas folds occurring exclusively within the layers of the sensory retina are termed retinal folds (Fig. 156.1). Choroidal folds are often a sign of orbital or ocular disease, but they may develop after surgery on the eye or orbit or may occur idiopathically.[1-6] Retinal folds found without the presence of choroidal folds develop most commonly in macular pucker, but they can also be present in association with uveitis, in response to certain medications,[7] and as a result of proliferative vitreoretinopathy.
|
|
|
|
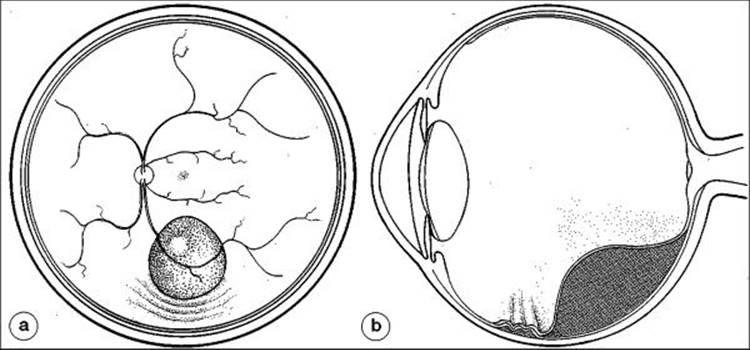
FIGURE 156.1 (Top) Retinal folds involve the superficial layers of the retina and are usually secondary to tangential forces present on the retinal surface. The underlying RPE (cuboidal cells) and choroid are not characteristically folded. (Bottom) Choroidal folds are characterized by undulations of the choroid, Bruch's membrane, and overlying retinal pigment epithelial layers. The sensory retina is folded in the deeper layers, but these pleats do not extend completely to the superficial layers. Hence, retinal vessels are typically not included in the folding process. |
CHOROIDAL FOLDS DESCRIPTION, PATHOGENESIS, AND SYMPTOMS
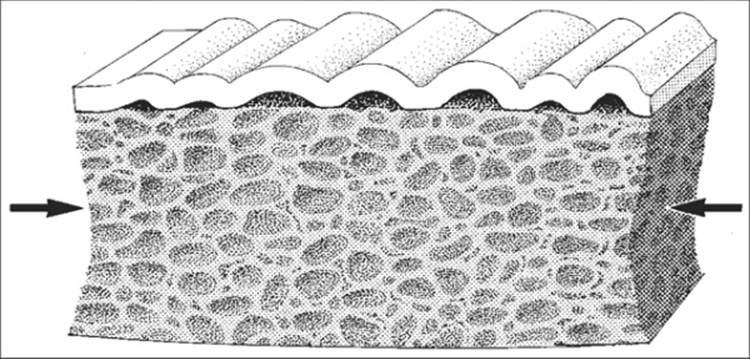
Choroidal folds are undulations of the choroid, Bruch's membrane, and pigment epithelium, with the overlying retina wrinkled to a lesser extent.[1] They develop secondary to mechanical stresses produced within these tissues. Because the choroid consists of a plexus of randomly oriented blood vessels, an interstitium of connective tissue, and multiple fluid-filled spaces, it has intrinsic elasticity and sponginess. In addition, Bruch's membrane and the overlying retinal pigment epithelium (RPE) are firmly bonded to the inner surface of choroid at the choriocapillaris. This architecture is roughly analogous to that of a sponge onto which a thin elastic sheet has been fused. When such a sponge is compressed, folds form along its surface (Fig. 156.2). Analogously, if compressive forces of sufficient magnitude are induced in the choroid, it will be forced into pleats or folds, as will Bruch's membrane, the pigment epithelium, and the sensory retina. Hence, choroidal folds are a manifestation of biomechanical stresses present within the choroid, rather than being a sign of a particular disease.[2]
|
|
|
|
FIGURE 156.2 As an analogy, the formation of choroidal folds may be compared with folds developing along the surface of a compressed sponge onto which an elastic membrane has been glued. The sponge represents the choroid, whereas the membrane represents Bruch's membrane and the RPE. |
Symptoms of choroidal folds depend on the degree of folding of the overlying retina, particularly at the fovea, and the amount of induced refractive error associated with the development of the choroidal folds. Retinal folds running through the fovea in association with choroidal folds may cause metamorphopsia and a reduction of visual acuity that cannot be eliminated by corrective lenses. Since choroidal folds are commonly found when the choroid is thickened or the globe has been flattened posteriorly, axial hyperopia is typical. If the globe is deformed more anteriorly from an intraorbital tumor, induced astigmatic errors along with the hyperopia are common.[8] Incidental equatorial folds created by encircling procedures to repair retinal detachments do not cause distortion or refractive errors themselves, but the scleral buckle in this situation produces relative myopia.
On funduscopic examination, choroidal folds appear as alternating dark and light streaks. Often, their appearance is subtle, especially if the fundus is lightly pigmented and the folds have not undergone any chronic changes. Choroidal folds are best viewed clinically by indirect ophthalmoscopy, as the field of view is usually large enough to allow observation of the entire fold pattern.
Histopathologic sections through choroidal folds demonstrate the reason for their striated appearance. Typically, Bruch's membrane and the RPE are tightly folded within the troughs of the folds (as viewed from the vitreous), whereas at the crests, the change in curvature is more gradual.[4] Hence, the melanocytes within the choroid and the RPE are compressed into a smaller-than-normal region in the troughs, whereas over the crest of the folds, these cells are stretched apart. This change in pigment density across the folds creates the alternating dark and light striae seen clinically.
FLUORESCEIN ANGIOGRAPHY AND CHOROIDAL FOLDS
Sodium fluorescein leaks quickly out of the fenestrations of the choroidal vessels and stains the choroid. However, because the RPE effectively filters out most of this potential background choroidal fluorescence, the choroid appears gray rather than white on angiography. In the troughs of the choroidal folds in which the RPE cells are compressed, the RPE becomes a more efficient filter. Conversely, when the choroid and RPE are stretched, the concentration of melanin granules per unit area is reduced. The net effect is that choroidal folds appear dramatically as alternating dark and light striae on fluorescein angiography (Fig. 156.3).[9]
|
|
|
|
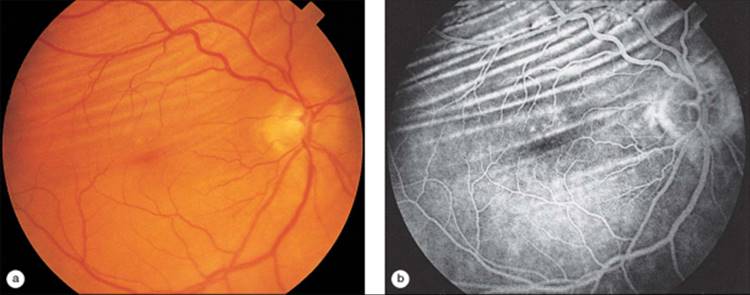
FIGURE 156.3 (a) Fundus appearance of choroidal folds caused by an extraconal tumor located within the superior temporal quadrant of the orbit. (b) On fluorescein angiography, the folds are much more dramatic, appearing as alternating light and dark streaks. Note that the retinal vessels are not distorted by the underlying choroidal folds. |
OCT AND CHOROIDAL FOLDS
OCT is a relatively new imaging tool for the posterior segment of the eye.[10] Similar to ultrasound B-mode imaging, a cross-sectional image is generated by measuring the backscattered or backreflected light from the tissue within the eye. Based on the optical properties of the underlying tissue, the layers of the retina and choroid are distinguished. The choroid appears darker in comparison to the highly reflective RPE above. The cross-section image provided by OCT can easily detect the undulating appearance of the RPE (Fig. 156.4). The elastic properties of the choroid are different from those of the sensory retina. Hence the retina can, to some degree, internally adjust (creep) along the underlying choroidal folds. This is evident on the OCT when the inner surface of the retina is only mildly undulating as opposed to the folds at the level of the choriocapillaris, Bruchs membrane, and RPE. Used in conjunction with fluorescein angiography, OCT can differentiate retinal folds from choroidal folds in various retinal pathology involving the macula and periphery.[11]
|
|
|
|
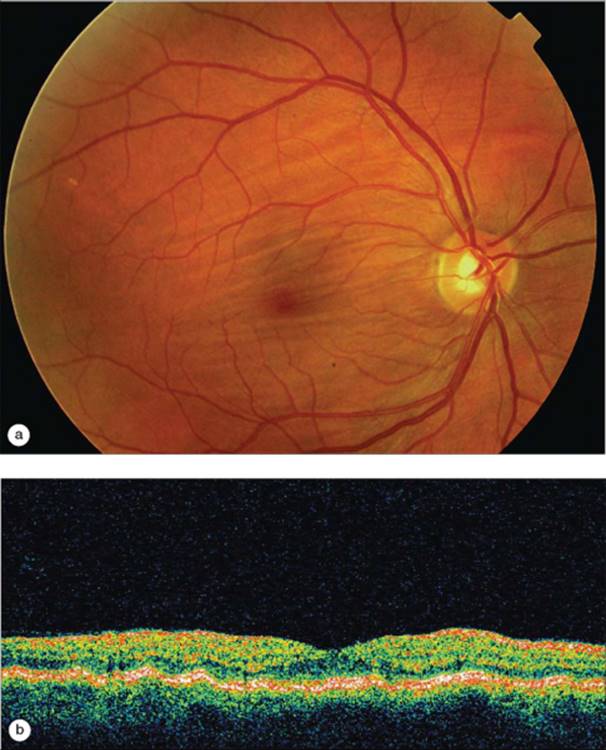
FIGURE 156.4 (a) Fundus photo of the right eye in a woman with hyperopia and idiopathic choroidal folds. (b) Cross-sectional image with false color through the posterior pole of the same eye. The troughs and crests of the highly reflective RPE layer indicate choroid folds in the macula. |
CHOROIDAL FOLDS AND SPECIFIC DISORDERS
CHOROIDAL TUMORS AND CHOROIDAL DETACHMENTS
When a choroidal tumor such as a melanoma, metastatic carcinoma, or choroidal hemangioma grows, it compresses the adjacent choroid and may force it into folds. In this instance, folds develop parallel to the boundaries of the tumor (Fig. 156.5). Similarly, choroidal folds may develop at the edge of large choroidal detachments. The folds in these cases are not extensive because only local compressive stresses are produced. Folds typically do not form over the tumor surface, at which point the choroid is stretched rather than compressed. Occasionally, however, folds develop over regions of localized choroidal hemorrhage.[12]
|
|
|
|
FIGURE 156.5 (a) An expanding choroidal tumor compresses the choroid along its boundaries, forming folds parallel to the tumor's perimeter. (b) Folds seldom form over the tumor surface because the choroid is stretched uniformly over the mass, as seen in this vertical cross-section. |
ORBITAL TUMORS
Intraconal Orbital Tumors
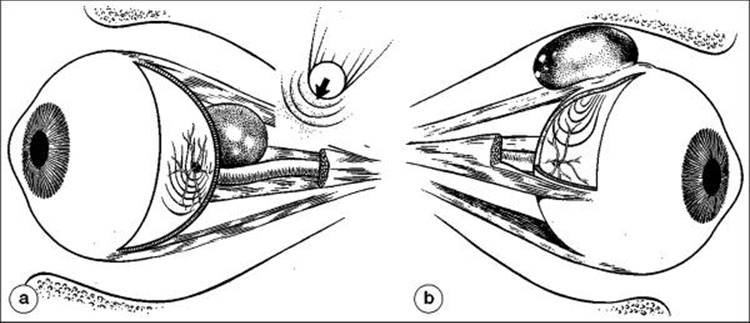
Tumors located within the muscle cone, such as cavernous hemangiomas, metastatic neoplasms, and optic nerve meningiomas, can press on the globe posteriorly, producing exophthalmos, flattening of the globe, and shifting of the refractive error toward hyperopia.[8] In addition, such a tumor often displaces the optic nerve to one side, inducing stresses within the globe at the disk (Fig. 156.5a). The choroid on one side of the optic nerve is compressed, whereas, on the opposite side, the choroid is stretched, often resulting in a parabolic fold pattern with the nerve head located among the folds (Fig. 156.6).[8]
|
|
|
|
FIGURE 156.6 (a) Intraconal orbital tumors typically displace the optic nerve, compressing the choroid in the direction of the nerve head displacement, and placing the choroid under tension on the opposite side. The result is a choroidal fold pattern, the convex side of which is directed away from the nerve head (arrow). (b) Extraconal tumors buckle the wall of the globe equatorially, producing a curvilinear fold pattern with its convex side directed toward the optic nerve. |
Extraconal Orbital Tumors
An extraconal tumor may press directly on the extraocular muscles and Tenon's capsule, as well as on the sclera. The forces generated tend to buckle the wall of the globe (see Fig. 156.6b), creating choroidal folds. Because of anterior segment distortion, astigmatic refractive errors are commonly induced. With respect to the fold pattern, the convex side usually points toward the posterior pole and optic nerve, but the nerve head is usually located outside the region of folds (Figs 156.7 and 156.8).[8] Typical extraconal tumors associated with choroidal folds include mucoceles, dermoids, tumors of the lacrimal gland, and orbital meningiomas.
|
|
|
|
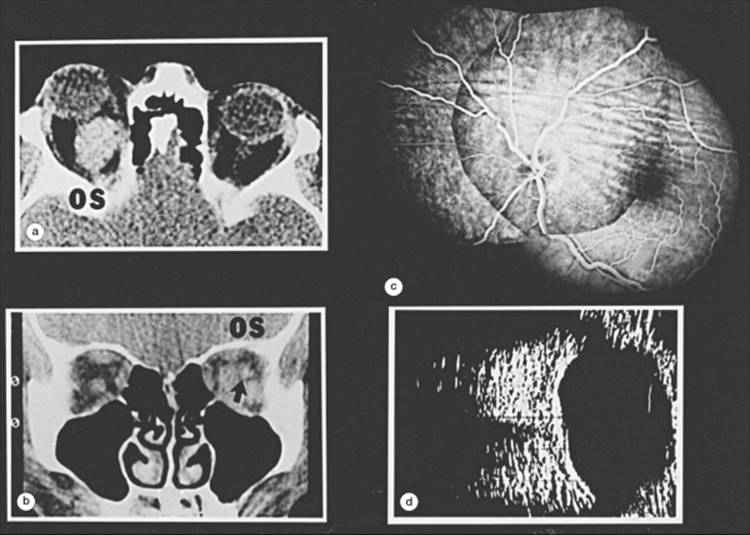
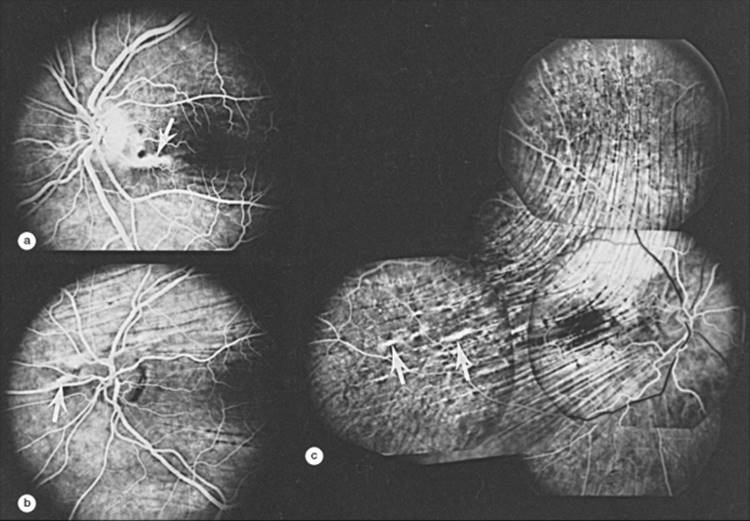
FIGURE 156.7 (a and b) An intraconal tumor (in this case, an orbital hemangioma) has displaced the left globe and optic nerve superiorly (arrow), as seen in computed tomograms. (c) The associated choroidal folds are primarily located superior to the optic nerve, whereas some folds radiate from the disk and extend into the macula. (d) A B-scan ultrasonogram demonstrates characteristic flattening of the posterior sclera. |
|
|
|
|
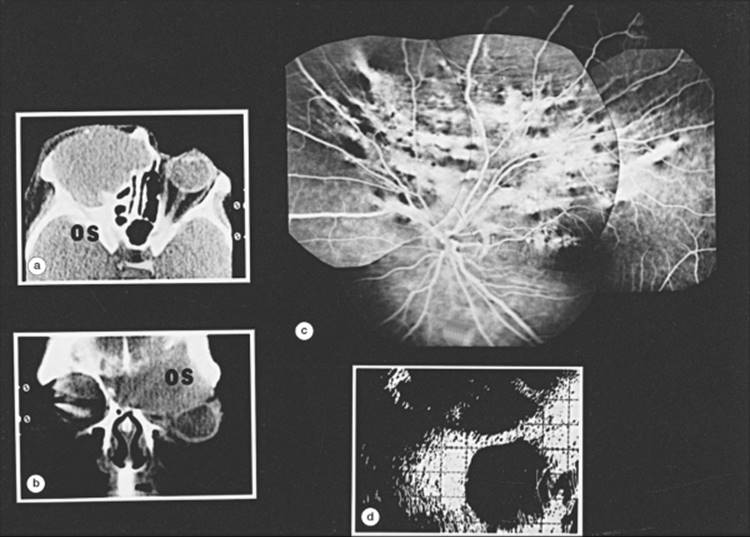
FIGURE 156.8 (a and b) Choroidal folds caused by an extraconal tumor (in this case, a meningioma) that has displaced the left globe inferiorly and temporally as seen on computed tomography. (c) A curvilinear fold pattern typically associated with an extraconal tumor is seen on the fluorescein angiogram, with the convex side of the pattern directed toward the optic nerve head. (d) A B-scan ultrasonogram shows equatorial flattening of the sclera by the meningioma. |
Orbital Tumors and the Pattern of Folds
Although historically the choroidal fold pattern was said to have no relevance in localizing a tumor within the orbit,[1] in fact the pattern of folds often reflects the location of the orbital pathologic condition. The tumor is often located along the axis of symmetry drawn through the pattern of choroidal folds.[8] The location as indicated by the folds is only approximate, however, and must be corroborated by more sophisticated evaluations, such as computed tomography or B-scan ultrasonography.
DISORDERS OF THE OPTIC NERVE HEAD
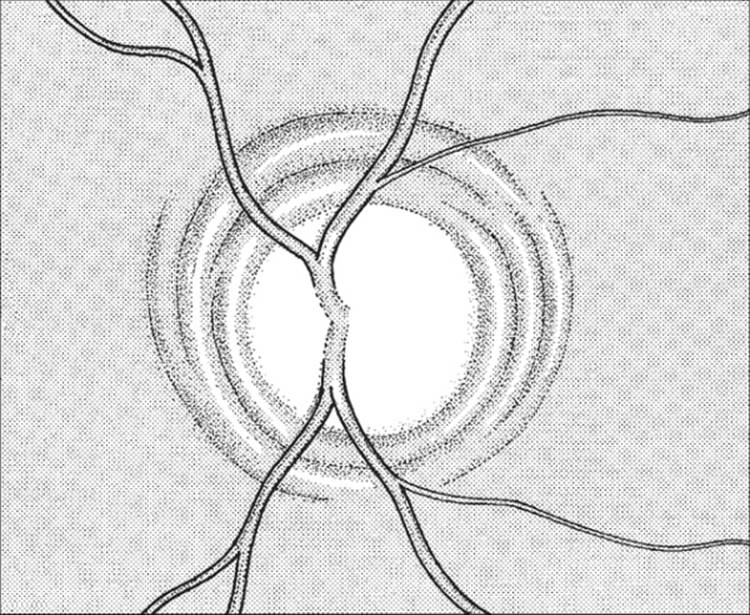
As the optic nerve head swells, it expands centrifugally, compressing the peripapillary choroid and often creating choroidal folds concentric to the disk margins (Fig. 156.9). Thus, concentric folds are a sign of papilledema,[13] disk edema, optic nerve head drusen, or a tumor within the nerve head. In these cases, the abnormality of the optic nerve is usually quite obvious, whereas the folds themselves are subtle.
|
|
|
|
FIGURE 156.9 Swelling of the optic nerve from papilledema or tumor compresses the adjacent choroid, producing choroidal folds concentric to the disk. |
SCLERAL BUCKLING PROCEDURES
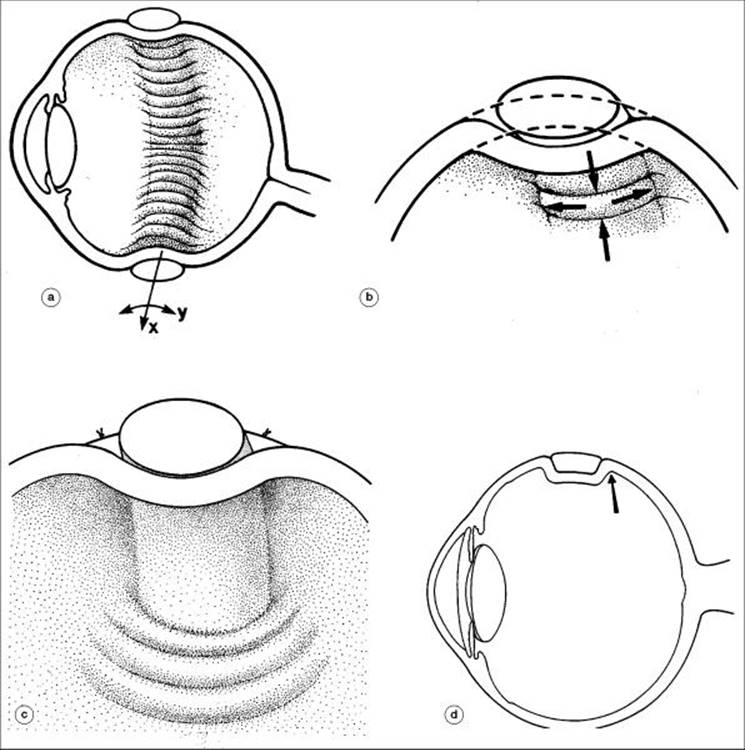
Encircling scleral buckling procedures are commonly associated with choroidal striae (Fig. 156.10a,b). In this case, the folds are confined to the vicinity of the buckle and are oriented perpendicular to the plane of the encircling element. The encirclement reduces the surface area available to the choroid, compressing the tissue together within the plane of the buckling element. In addition, radial buckling elements can also produce folds by compression (Fig. 156.10c,d). Folds associated with retinal surgery are typically prominent during the immediate postoperative period and fade over time. Furthermore, choroidal folds caused by buckling are smoothed out if the intraocular pressure rises.
|
|
|
|
FIGURE 156.10 (a) Choroidal folds secondary to an encircling scleral buckle. (b) The choroid is compressed in the x direction along the plane of the buckle and stretched in the y direction, producing folds oriented perpendicular to the induced compressive stresses. (c) A radially placed scleral buckle element produces choroidal folds by compressing the adjacent choroid. (d) The abrupt change in scleral contour (arrow), as seen on cross-section, creates these compressive forces. |
CHORIORETINAL SCARS AND CNV
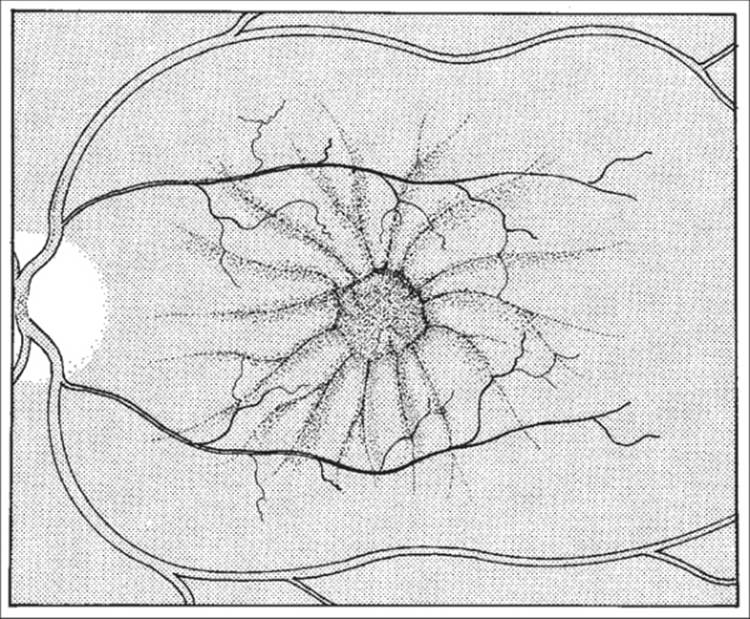
Dense, fibrotic chorioretinal scars from trauma or intense choroidal inflammation contract as the scar tissue matures. Forces from this contraction pull on the surrounding choroid and may produce folds directed radially toward the center of the scar (Fig. 156.11). Scarring associated with CNV can also produce radially oriented folds.[14]
|
|
|
|
FIGURE 156.11 A dense chorioretinal scar draws the surrounding choroid inward toward its center as the scar tissue matures and contracts. Radially oriented folds are produced. |
FOLDS ASSOCIATED WITH CHOROIDAL THICKENING
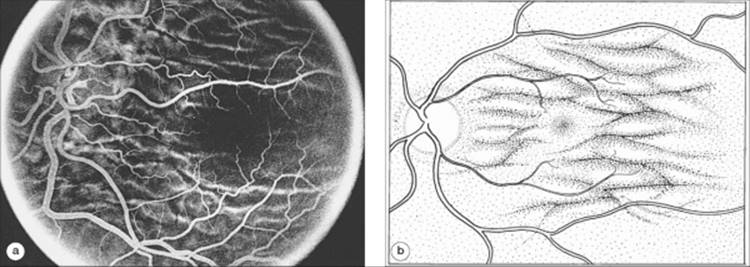
The choroid may thicken as a result of hypotony, inflammation, the uveal effusion syndrome, or venostasis such as that found after a central retinal vein occlusion. As its thickness increases, the surface area available to the choriocapillaris, Bruch's membrane, and the RPE is reduced because the choroid must expand inward toward the center of the eye, being confined by the sclera. Ultimately, the choroid may be forced into redundant folds (Fig. 156.12). Additionally, because the internal diameter of the globe has been decreased, the refractive error shifts toward hyperopia. It is important to remember that this hyperopia is secondary to the development of choroidal thickening and fold formation, rather than being the cause of the folds.
|
|
|
|
FIGURE 156.12 (a) Fluorescein angiogram of choroidal folds associated with hypotony and secondary choroidal thickening. (b) In these cases, the choroidal fold pattern is typically random, as the folds develop secondary to rather uniform swelling of the choroid. |
HYPOTONY
Hypotony or low intraocular pressure results in radial expansion of the choroid toward the vitreous cavity. Hypotony may result from an obvious cause such as uveitis, trauma, or filtration surgery, particularly when 5-fluorouracil or mitomycin C are used.[15,16] Choroidal folds developing shortly after anterior segment surgery suggest a wound leak or the presence of a cyclodialysis cleft.
INFLAMMATION
Inflammatory diseases of the orbit and sclera such as Graves' exophthalmopathy, orbital pseudotumors, and orbital myositis can flatten the sclera and cause scleral and choroidal thickening. Choroidal compression and choroidal fold formation may be the result. In diseases such as inflammatory bowel disease, the choroid itself may show signs of inflammation and may develop folds from uveitis.[17]Sometimes, serous retinal detachments develop in association with the folds, presenting a confusing picture. Successful treatment of the inflammatory component will lead to resolution of the folds in most cases.
UVEAL EFFUSION
Eyes with idiopathic choroidal folds and concomitant serous detachments may appear similar to eyes with the uveal effusion syndrome. Typically, this syndrome is characterized by poor vision, a thickened or detached choroid and ciliary body, and an extensive serous retinal detachment that dominates the clinical appearance.[18] In some cases, however, the choroid may be thickened uniformly without a significant serous detachment, and vision may be maintained. In these cases, choroidal folds may be the first sign of an abnormality. Decompression of the vortex veins and excision of scleral flaps has, in some severe cases, led to resolution of the choroidal detachments and folds with improvement of visual acuity.[18,19]
IDIOPATHIC FOLDS
Choroidal folds may develop in one or both eyes of a patient with no apparent ocular or orbital disorder. These patients are usually male and often present with acquired hyperopia of 3 D or less. Computed tomographic findings in these eyes may show thickening of the sclera, flattening of the posterior pole, enlargement of the optic nerve image, and the presence of a space seen between the optic nerve and its meninges.[20] Occasionally, serous retinal detachments develop (Fig. 156.13). Patients usually retain good vision, and in some individuals the folds disappear spontaneously.[17] The cause of these alterations is unclear. Possibly, drainage through the choroidal venous plexus and into the vortex veins is compromised from structural alterations within the scleral wall. In other cases, posterior scleritis or other local inflammation may have initially produced the folds, which then persist long after the inflammation resolves. Alternatively, idiopathic choroidal folds and acquired hyperopia have been described in intracranial hypertension.
|
|
|
|
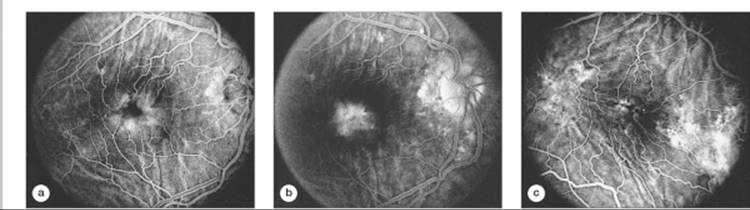
FIGURE 156.13 (a) Fluorescein angiogram of the right eye in a woman with mild hyperopia and acquired chorioretinal folds. (b) There is leakage of dye from the choriocapillaris, which pools within the fovea in the late-phase films. A serous retinal detachment is present overlying the area of leakage. (c) Left eye of the same patient. Fluorescein angiography shows randomly oriented folds and retinal pigment epithelial window defects in the peripapillary region, at the fovea, and temporal to the macula. |
IMPLICATIONS OF CHOROIDAL FOLDS
Choroidal folds are a sign of an ocular disorder or disease. Hence, the major consideration when presented with a patient with choroidal folds is to determine the cause of the folds. Of particular importance is an investigation to rule out the possibility of an orbital or choroidal tumor or intracranial hypertension.[21] B-scan ultrasonography and computed tomography are usually indicated, particularly in patients with unexplained unilateral folds.
If choroidal folds remain for months, the RPE in the troughs may undergo hypertrophy and hyperplasia from being mechanically compacted. Even if the folds resolve, this linear pigmentation may persist. RPE atrophy and apparent fractures of Bruch's membrane may also be seen along the folds, especially in older patients (Fig. 156.14). Such changes also occur along angioid streaks, which are sometimes confused with choroidal folds.[8] As with angioid streaks, CNV can develop along choroidal folds (Fig. 156.15).[22] If CNV develops, treatment should be initiated using strategies commonly used for neovascular age-related macular degeneration. Macular folds of the choroid should therefore be eliminated, if possible, to help avoid permanent visual loss.
|
|
|
|
FIGURE 156.14 (a-c) Retinal pigment epithelial clumping and atrophy (arrows) can occur along choroidal folds, making the folds appear similar to atrophic angioid streaks, both on clinical examination and particularly on fluorescein angiography. |
|
|
|
|
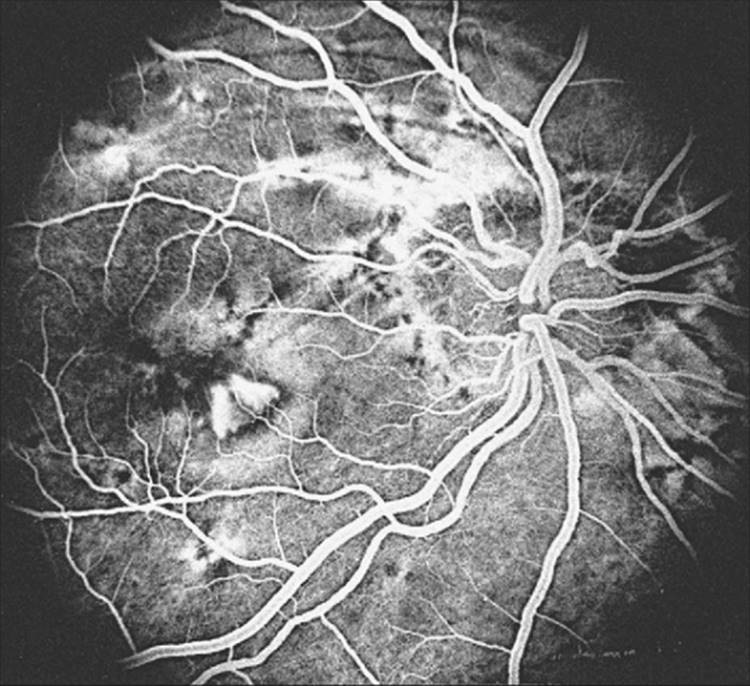
FIGURE 156.15 CNV may develop along choroidal folds, as demonstrated by this trapezoidal choroidal neovascular net found along a fold running through the macula. In this case, the choroidal folds developed secondary to an orbital tumor. |
|
Key Features |
||||||
|
RETINAL FOLDS
Retinal folds are commonly associated with epiretinal membrane formation. Such membranes exert stress on the underlying retina and promote wrinkle formation, leading to macular pucker and symptoms of metamorphopsia. These cellophane-like membranes can best be seen on careful biomicroscopy of the fundus. Alternatively, in certain cases of rhegmatogenous retinal detachment, proliferative membranes grow along the retinal surface, creating star folds and retinal striae. In both instances, surgical removal of the membranes may be necessary.
Shallow superficial retinal folds may develop when choroidal folds are lacking whenever there is relative choroidal thickening, particularly in association with uveal inflammation. Reduction of the surface area available to the retina from the radial displacement of the choroidal surface is a likely cause. Retinal folds in conjunction with transient myopia may also be associated with the administration of sulfonamides. In this case, swelling of the ciliary body and vitreous traction may play a role.[6] Elimination of the uveal inflammation or discontinuation of the sulfonamides should promote resolution of the retinal folds in these cases.[6]
|
Key Features |
|||||||||
|
REFERENCES
1. Newell FW: Choroidal folds. Am J Ophthalmol 1973; 75:930-942.
2. Friberg TR: The etiology of choroidal folds. Graefes Arch Clin Exp Ophthalmol 1989; 227:459-464.
3. Cangemi FE, Trempe CL, Walsh JB: Choroidal folds. Am J Ophthalmol 1978; 86:380-387.
4. Wolter JR: Parallel horizontal choroidal folds secondary to an orbital tumor. Am J Ophthalmol 1974; 77:669-673.
5. Bullock JD, Egbert PR: The origin of choroidal folds: a clinical, histopathological and experimental study. Doc Ophthalmol 1974; 37:261-293.
6. Hertle RW, Leahey AB, Bloom S, et al: Chorioretinal folds and a macular hole secondary to craniofacial surgery. Ophthal Plast Reconstr Surg 1990; 6:278-282.
7. Ryan EH, Jampol LM: Drug-induced acute transient myopia with retinal folds. Retina 1986; 6:220-223.
8. Friberg TR, Grove AS: Choroidal folds and refractive errors associated with orbital tumors. An analysis. Arch Ophthalmol 1983; 101:598-603.
9. Griebel SR, Kosmorsky GS: Choroidal folds associated with increased intracranial pressure. Am J Ophthalmol 2001; 131:158-159.
10. Norton EWD: A characteristic fluorescein angiographic pattern in choroidal folds. Proc R Soc Med 1969; 62:119-128.
11. Hee MR, Izatt JA, Swanson EA, et al: Optical coherence tomography of the human retina. Arch Ophthalmol 1995; 113:325-332.
12. Kokame GT, de Leon MD, Tanji T: Serous retinal detachment and cystoid macular edema in hypotony maculopathy. Am J Ophthalmol 2001; 131:384-386.
13. Morgan CM, Gragoudas ES: Limited choroidal hemorrhage mistaken for a choroidal melanoma. Ophthalmology 1987; 94:41-46.
14. Gass JDM: Radial chorioretinal folds: a sign of choroidal neovascularization. Arch Ophthalmol 1982; 99:1016-1018.
15. Altan T, Temel A, Baubeck T, Kazokoglu H: Hypotonic maculopathy after trabeculectomy with post-operative use of 5-fluorouracil. Ophthalmologica 1994; 208:318-320.
16. Stamper RL, McMenemy MG, Lieberman MF: Hypotonous maculopathy with subconjunctival 5-fluorouracil. Am J Ophthalmol 1992; 114:544-545.
17. Ernst BB, Lowder CY, Meisler DM, Gutman FA: Posterior segment manifestations of inflammatory bowel disease. Ophthalmology 1991; 98:1272-1280.
18. Schepens CL, Brockhurst RJ: Uveal effusion: clinical picture. Arch Ophthalmol 1963; 70:189-201.
19. Ward RC, Gragoudas ES, Pon DM, Albert DM: Abnormal scleral findings in uveal effusion syndrome. Am J Ophthalmol 1988; 106:139-146.
20. Dailey RA, Mills RP, Stimac GK, et al: The natural history and CT appearance of acquired hyperopia with choroidal folds. Ophthalmology 1986; 93:1336-1342.
21. Jacobson DM: Intracranial hypertension and the syndrome of acquired hyperopia with choroidal folds. J Neuroophthalmol 1995; 15:178-185.
22. Friberg TR, Grove AS: Subretinal neovascularization and choroidal folds. Ann Ophthalmol 1980; 12:245-250.