Harry B. Skinner, MD, PhD
Orthopedic surgery encompasses the entire process of caring for the surgical patient, from diagnostic evaluation to the preoperative evaluation and through the postoperative and rehabilitative period. Although the surgical procedure itself is the key step toward helping the patient, the preliminary and follow-up care can determine whether the surgery is successful.
DIAGNOSTIC WORKUP
![]() History and Physical Exam
History and Physical Exam
Although it may seem obvious, the history and physical exam are still important in the evaluation of the patient. Every office visit is a history and physical exam, whether a new or a return visit. The completeness of the history and physical has assumed new importance in view of the complexities required for compliance with federal regulations. Regulations require that a chief complaint be specified, and this must be clearly defined because it determines the direction for the rest of the history and physical. The history must address the key features of the problem, both to elucidate the medical problem and to cover the subsidiary requirements for billing purposes. The social history and past medical history are similarly important because they change billing codes without necessarily affecting outcome or success of care. The physical again must cover the essentials necessary for diagnosis, and frequently the confirmation of the diagnosis is based on physical exam, but such considerations as skin condition and blood supply must be documented, despite the fact that this process is also part of the surgical evaluation. The next step is imaging and laboratory exams. The most important point here is to use the most cost-effective examination possible while keeping patient safety, satisfaction, and convenience in mind.
![]() Imaging Studies
Imaging Studies
A. Roentgenography
Roentgenography is still the most cost-effective and most important initial diagnostic test in the orthopedist’s armamentarium. Almost every patient should have a radiograph prior to going to a more sophisticated imaging study. Certain situations are obvious; for example, a 68-year-old man with knee pain should have standing, flexed-knee posteroanterior (PA), lateral, and merchant plain film views taken. If those views show normal joint spaces, consideration of intraarticular pathology, such as a degenerative meniscus tear, can be worked up with magnetic resonance imaging (MRI). The normal views usually ordered are as follows:
1. Neck pain—
No history of trauma, more than 4 weeks’ duration. Younger than 35 years: anteroposterior (AP) lateral, odontoid.
Older than 35 years: obliques.
History of trauma: flexion/extension laterals (obtain on first visit).
2. Thoracic spine pain and tenderness—
Younger than 40 years, no reason to suspect malignancy: AP and lateral (if history of trauma, or possibility of osteoporosis on first visit, otherwise at 4 weeks).
Consider cervical (C)-spine as a source of referred pain to thoracic (T)-spine if no tenderness in T-spine.
3. Lumbar (L)-sacral (S)-spine—
Younger than 40 years, no reason to suspect malignancy after 4 weeks’ duration of the pain. With significant trauma, at first visit, or possible malignancy (ie, weight loss, malaise, fatigue): AP, lateral.
Add obliques for chronic low back pain (ie, spondylolisthesis).
4. Hips—
AP pelvis, lateral of affected hip.
Consider lumbar-sacral (L-S) series if pain is in the buttock rather than in the groin.
5. Knees—
Older than 40 years or history of meniscectomy: Rosenberg, lateral, and sunrise films. Merchant views are similar to sunrise. The Rosenberg view is a 10-degree down shot of the PA of the knees while standing at 45 degrees of flexion.
For other knees: AP, lateral, and sunrise.
In the child, up to age 16, consider a pelvis film with the complaint of knee pain and negative physical exam referable to the knee.
6. Femur, tibia, humerus, forearm—AP and lateral are indicated for trauma, palpable lesions, or suspected tumors.
7. Ankle—AP lateral and mortise.
8. Foot—AP, lateral, and oblique for routine evaluation.
9. Shoulder—AP, axillary, scapular Y, and outlet views.
10. Elbow—AP and lateral (true lateral).
11. Hand/wrist—
Hand: PA and lateral.
Wrist: PA, lateral, and oblique
For suspected instability: clenched fist PA in radial and ulnar deviation.
Follow-up radiographs are obtained when a change in the radiographic findings is expected. Remember that bone changes occur slowly, so radiographic changes take a comparable length of time. Radiographs are obtained in view of the clinical picture. For example, closed treatment of a distal radius fracture would not be expected to show changes because of healing for a minimum of 2 weeks. However, displacement of the fracture could occur sooner. Hence, radiographs to show displacement might be obtained at 1 week and 2 weeks. If no displacement is observed, the fracture position could be considered stable, and the next films might be obtained at 6 weeks—the earliest time healing might be observed. Similarly, closed treatment of an adult tibia fracture might be followed with radiographs at 2-week intervals, checking for displacement and healing, whereas a tibia fracture treated with an intramedullary rod might be followed at monthly intervals to check for healing.
B. Magnetic Resonance Imaging
This imaging modality is very useful, but like electron beam computed tomography (CT), MRI is sometimes too revealing. This method should be reserved for clarifying a particular problem. Frequently in orthopedics, a bony lesion can be localized with a radiograph or bone scan, which then provides a focus for the MRI. MRI is useful for some bony lesions, such as osteonecrosis, tumors, fatigue fractures, and osteomyelitis. It is also helpful in some soft-tissue problems, such as knee meniscus tears and shoulder rotator cuff tears. Distortion of the magnetic field by metallic implants may limit the usefulness of MRI studies of conditions such as total knee or hip replacement, or fracture fixation devices. MRI should not be used when the diagnosis can be made with a less expensive test. For example, the use of the MRI in knee studies in patients older than 45 years should always be preceded by plain films of the knee, as noted earlier. An MRI of an arthritic knee adds little additional information because the meniscus and anterior cruciate ligament are likely to be damaged from the arthritic process already. However, the MRI can be very helpful in determining soft-tissue extension of tumors or infection.
The advent of new portable MRI units that perform limited studies with more resolution adds a new dimension to their use. These can provide data on the progression of disorders such as rheumatoid arthritis or osteomyelitis in a timely and cost-effective way. The possibility of osteomyelitis in the bones adjacent to ulcers on the foot is easily determined with this test because it shows the changes, typically edema, in the bone with osteomyelitis. A bone scan usually does not have the resolution to distinguish the inflammatory response in the soft tissue from the bony involvement. Osteomyelitis should be treated much differently from a soft-tissue ulcer, which does not affect the bone.
C. Computed Tomography
The CT scan is an extremely important imaging modality for examining bony lesions such as fractures. Frequently, plain films provide some information about the fracture of interest, but the CT scan provides the three-dimensional information that can only otherwise be determined from the integration of the plain films in the surgeon’s mind. The CT scan adds significantly to the management of such fractures as tibial plateaus, scapular fractures, ankle fractures, and cervical and lumbar spine fractures, as well as many others. Furthermore, nonunions of fractures, with or without fixation, can be identified and followed with CT scans. Again, if little information can be gained that cannot be already discerned from the plain films, the CT scan only adds expense and patient inconvenience. The spiral CT makes imaging with this modality less expensive and much more rapid. The CT scan is also now the method of choice for determining whether a pulmonary embolus (PE) has occurred. Again, a CT for this indication is easier on the patient, more accurate, and less invasive than angiography.
D. Technetium-99m Bone Scan
The bone scan finds many uses in orthopedic surgery. Keep in mind that the bone scan labels the osteoblast activity with the radioactive tracer, technetium-99; thus, bone formation activity is recorded, and little or no bone resorption activity is noted. Any disorder that results in increased bone formation, therefore, results in a “hot” bone scan. This means that a disorder such as multiple myeloma may not show up on a bone scan because only osteoclastic activity is involved in the majority of lesions. This test is helpful in discerning loose total hip and total knee prostheses, however, even though the findings are nonspecific. It is very helpful in examining probable benign bone lesions because a cold bone scan largely rules out an aggressive process such as a malignancy. The bone scan is also helpful in diagnosing any disorder of unknown origin when there is pain localized to a particular region. A cold bone scan implies that the problem is a soft-tissue one, whereas a hot bone scan points to a region that may benefit from MRI.
![]() Laboratory Exams
Laboratory Exams
The two most important laboratory exams are for C-reactive protein and the erythrocyte sedimentation rate. These two tests indicate whether an inflammatory process, malignancy, or rheumatologic disorder is a diagnostic consideration. If these tests are negative, systemic causes of a complaint can frequently be ruled out. In that situation, a more localized disorder should be identified. The next most important test is the complete blood count, which provides the general indication of the patient’s health, revealing information about anemia, infectious processes, and so on. The next most useful laboratory test for the orthopedic surgeon is the synovial fluid analysis. This test typically should include a culture and sensitivity. If there is any concern about infection, a cell count, differential, protein, and glucose measurement should be performed. Crystals should be looked for because they indicate chondrocalcinosis or gout. Elevated protein and reduced glucose levels suggest infection. The final factor that should be considered with any major surgery is the patient’s nutritional status, which is evaluated with several tests, including lymphocyte count and levels of prealbumin, albumin, zinc, and serum iron transferrin. In addition, the Mini Nutritional Assessment is a nursing tool to screen elderly individuals at risk of malnutrition.
![]() Educating and Informing Patients and Their Families
Educating and Informing Patients and Their Families
Surgical procedures in orthopedics have varying degrees of difficulty and importance, ranging from a relatively simple claw toe correction to the performance of a multilevel complex spinal fusion. After the decision to employ surgery as a therapeutic modality is made, it is important to help the patient completely understand what to expect before, during, and after surgery. This process, which the legal profession calls informed consent, has the more important purpose of ensuring the patient’s cooperation and satisfaction.
To comply with the requirements of the legal profession and accrediting organizations, such as the Joint Commission on Accreditation of Healthcare Organizations (JCAHO), the surgeon must provide an explanation of the risks, prognosis, alternatives, and complications that might be encountered. The risks should be reviewed in some detail for the general risks encountered in typical orthopedic surgical procedures. The risks and the complications that occur in surgery are intimately associated and thus must be dealt with together. The alternatives are sometimes straightforward. For example, a patient with an open fracture has a high risk of infection if not adequately treated with irrigation, debridement, and antibiotics. Thus, in such a situation, any reasonable and prudent person would consent to the procedure. The choice between alternatives can become significantly more subtle, however. For example, it is possible that a choice must be made between two different procedures or between a particular procedure and no procedure. In this situation, the surgeon must consider the psychosocial and physical attributes of the patient so as to assist him or her in making this decision. For example, consider men, both 75 years of age, with severe degenerative disease in the right knee noted on radiograph. One individual is now at the point where he cannot play golf, a situation that is reducing his physical exercise and a number of his social outlets. The other individual leads a relatively sedentary lifestyle, seldom walks more than a block, and obtains cardiorespiratory exercise by swimming, an activity in which his knee does not bother him. The surgeon should recommend knee replacement to one individual but not the other. At the same time, both men must be offered the alternatives, which include continued nonsteroidal anti-inflammatory medicine, bracing, sleeping medication, and analgesics.
Patients with an active lifestyle are becoming much more concerned about what will happen to them in the postoperative period, including how soon they can safely travel, when they can work, and when they will be fully able to take care of themselves. They are also concerned about what social services are available to help them if they cannot care for themselves fully. The surgeon must be prepared to address these questions and also advise patients with lower extremity or spinal problems about when they will be able to walk. In the same manner, after procedures on the hand or upper extremity, patients must be advised about when they will be able to use the hand. Advising the patient of these situations before surgery can prevent unexpected surprises in the postoperative period.
The patient should also be informed about the range of expectations for ambulation or use of the upper extremity because individuals vary in their response to surgery. For example, patients should be advised that after surgery on the hip or knee, they will need a walker for a few days, move to crutches, and typically be done with the crutches in the range of 2–4 weeks. They will use a cane before 6 weeks and be done with the cane before 3 months. Patients’ response to surgery is somewhat unpredictable, so conservative estimates on the length of medication use, pain, restricted driving, and so on are prudent. Patients should be cautioned about travel after surgery, particularly with lower extremity injuries, because of the risk of deep venous thrombosis (DVT). In such cases, discourage (for the first 6–12 weeks) plane trips longer than an hour and extended car trips made without stopping perhaps every 45 minutes. Anti-inflammatory medication (to reduce platelet adhesion) or anticoagulants should be recommended if such travel is unavoidable.
A. Explaining the Procedures
An essential part of the patient’s presurgical preparation and postsurgical cooperation is knowing what to expect at every step in the process. Nuances become important in the process of explaining the surgical procedures and their implications. For example, scheduling a bunion procedure 2 weeks prior to a patient’s participation in her daughter’s wedding could upset the patient if she fails to realize that she will be unable to wear the shoes she purchased for the event. Similarly, lifestyle considerations can affect the decision-making process in cases of medial gonarthrosis, in which the choice between a unicompartmental knee replacement and a high tibial osteotomy could be influenced by whether the patient plays tennis and holds a physically strenuous job or, alternatively, whether the patient is sedentary and works behind a desk most of the day.
B. Reviewing the Risks and Possible Complications
Reviewing the perioperative risks is important for all patients and optimally should be done well in advance and then repeated closer to the time of surgery. Some patients require more detailed explanations, particularly if their relatives have undergone surgery in the past and had a problem with anesthesia or a complication such as a PE or infection. Based on the patient’s responses to explanations, the health care team members need to alter their approach to reach a balance between inadequately informing the patient and inducing unnecessary alarm that could make the patient refuse to undergo a procedure judged to be both beneficial and necessary.
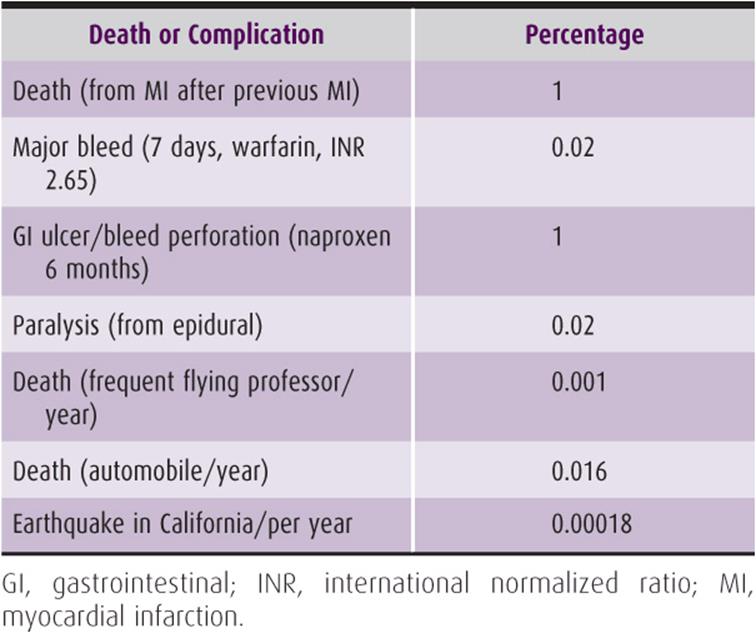
Risk is a poorly understood concept in our culture. Some situations are considered to be higher in risk than they actually are. Some risks are understood better than others. It can help the patient to understand if these risks are put in perspective. The risks can be surprisingly high or low but still disturbing to the patient. For example, many people have moved away from California to avoid an earthquake or refuse to fly commercial aircraft because of the risk, not realizing that the risk of death is 10–100 times higher while driving a car (Table 1–1). This lack of understanding of the risk can contribute to significant differences in the perception of liability associated with these activities. For example, the death benefit from a commercial airline accident might reach several million dollars per passenger, whereas death in an automobile accident might have no death benefit at all. Thus, the perception of risk is very important and must be clarified in the patient’s mind. Similarly, patients can understand and accept having a myocardial infarction after a major surgery because they can clearly see the strain on the heart from the surgery. However, they are not nearly as understanding of a lower extremity paralysis that can result from the epidural anesthetic for that surgery. The explanation of risks must be individualized for each patient. The patient with a previous myocardial infarction is clearly different from the healthy 20-year-old (see Table 2–1). Across-the-board rates of problems do not translate into direct risks for the individual patient.
Table 1–1. Rates of death and complications associated with common activities.
Although all procedures carry some risks, the incidence and type of risks and complications vary with the surgical procedure as well as with the patient’s age and general health. Potential problems are listed and discussed here in alphabetical order.
1. Amputation—The potential problem of amputation is seldom of acute concern except in cases of significant trauma. The topic of amputation can frequently be discussed with the risk of infection because ischemia and infection can increase the risk of amputation.
2. Anesthesia—One of the major risks in orthopedic surgery is associated with anesthesia, not because complications of anesthesia are frequent but because they can be devastating. Death occurs at a rate of approximately 1 in 200,000 patients undergoing elective anesthesia. Other complications include, but are not limited to, the following: nerve damage and paraplegia from nerve blocks, headaches from dural leaks following use of spinal anesthetics, aspiration of stomach contents, and cardiac problems, including ischemia and arrhythmias. The surgeon should discuss these problems with the patient only in general terms, allowing the anesthesiologist to provide the most detailed explanations.
3. Arthritis—Virtually any procedure that enters a joint, other than to replace it, has the potential to cause damage to that joint. In some instances, as in an intraarticular fracture, the surgery will likely lessen the risk of arthritis. Even in these instances, the patient should be told that the risk of damage is still real because the joint surface healing will not result in a normal cartilage surface.
4. Blood loss—Patients should be given a reasonably accurate estimate of blood loss as well as the opportunity to donate autologous blood prior to surgery. Designated donor blood is probably not safer but gives the patient who receives it a sense of security. The use of erythropoietin can elevate preoperative hemoglobin (Hgb) levels in selected cases and thereby reduce postoperative homologous blood transfusion needs. Other alternatives include the use of intraoperative blood salvage for reinfusion (OrthoPAT, Sure-Trans, Constavac). The use of erythropoietin is generally accepted by Jehovah’s Witness patients, whereas the autologous reinfusion acceptance is variable. To help minimize blood loss during surgery, the patient’s use of nonsteroidal anti-inflammatory drugs (NSAIDs) should be discontinued approximately 2 weeks before surgery. Discontinuation of NSAIDs can significantly compromise comfort and incite rheumatoid flares in many patients who rely on these drugs. To minimize the risk, newer cyclooxygenase-2 (COX-2) inhibitor NSAIDs may be used as a substitute during this period; no platelet disorder or bleeding time derangement occurs with these drugs because they do not affect platelet function or inhibit thromboxane A2.
5. Blood vessel damage—Arterial and venous damage take on greater significance as the size of the vessel increases and the arterial supply becomes more calcified with age and vascular disease. Patients generally understand this, but it must be emphasized where appropriate. Hip and knee replacement puts unusual strains on the femoral and popliteal vessels, from positioning, and may damage calcified arteries.
6. Deep venous thrombosis/pulmonary embolism—Virtually all lower extremity and spine procedures in orthopedics involve some risk of DVT, which should be explained to the patient. As many as 40–60% of patients who undergo a relatively high-risk procedure such as total hip arthroplasty develop DVT if not receiving thromboprophylaxis. The risk of PE is much less, however, and is in the range of 0.3% for fatal emboli. This rate of fatal PE is approximately a 10-fold increase over the rate of fatal PE in the U.S. population in men older than 65 years. The risks associated with other procedures may be lower. In any case, the patient should be reassured that prevention procedures commensurate with risk will be undertaken.
7. Fracture—Many procedures in orthopedic surgery carry the risk of a bone fracture. Some procedures, such as uncemented hip replacement, present a higher risk for this complication, but virtually any orthopedic procedure could result in fracture of a bone. The patient must be informed of the risk in relation to the probability of the occurrence of such a problem.
8. Infection—The risk of infection in orthopedic surgery ranges from near zero in procedures such as arthroscopy to several percent in open fracture surgery. The problem of infection should be emphasized in proportion to risk. For example, if a diabetic patient is to undergo knee replacement, he or she should not only be assured that all steps will be taken to prevent infection (eg, administration of prophylactic antibiotics, use of ultrafiltration of air, or ultraviolet lights in the operating room) but should also be told of the various techniques that would be considered if infection occurred. These options include debridement, prosthesis removal, gastrocnemius flap, reinsertion, arthrodesis, and amputation. The common use of external fixation devices for fracture care is accompanied by the frequent problems associated with pin care. The patient and family should be informed about the problems caused by percutaneous devices to prevent the presumption that something has gone wrong. Skin problems are frequently associated with infection but may arise from other causes, such as adjacent scars compromising the blood supply to a surgical flap. Older patients and individuals who are smokers, have diabetes and/or obesity, or have wounds on the distal lower extremity are at increased risk. In such cases, the patient may be warned that delayed healing or necrosis of the skin edges may occur.
9. Loss of reduction—Although fracture care continues to improve, displacement of hardware or fracture fragments may necessitate a second procedure. The explanation of this risk should be individualized, based on the type of fracture. Loss of reduction may contribute to delayed union or nonunion of fractures. These problems may occur despite optimal care by the orthopedic surgeon. Poor vascular supply or smoking can be a factor leading to nonunion. The rate of nonunion is site dependent but is only a few percent.
10. Nerve damage—Certain procedures are associated with nerve damage, although the damage is usually minor. For example, medial parapatellar incisions on the knee cause some numbness from cutting the infrapatellar branch of the saphenous nerve. The patient should be informed in advance if some degree of minor nerve damage is anticipated in association with the particular surgical procedure being pursued and should also be informed of the risks of unexpected nerve damage that accompany all surgical procedures.
C. Prognosis
The patient’s prognosis is intimately related to the procedure. However, certain guidelines may be given. The expected time off work or time away from activities is important to the patient and depends on the patient’s occupation, age, and available sick leave. The bank president with more control over her agenda will be able to return to work activities sooner than the day laborer. Driving is an important activity for many people, and limitations placed by a procedure can determine how much postoperative assistance a patient will need.
The patient should be given reasonable expectations about range of motion, strength, possible disability, and when these should return to normal, if at all. Furthermore, walking or writing ability, ability to use a computer keyboard, and the time to expect to be able to do such activities may be appropriate for some patients. Again, these have to be individualized for each patient and determined for each home situation.
D. Keeping the Patient and Family Informed
Immediately before elective surgery, the surgeon can help comfort the patient and family by meeting them in the preoperative area and appearing relaxed, well rested, and positive about the outcome of the surgery. Giving the family a good estimate of the surgery time is important, but they should also be reassured that delays do not necessarily indicate the occurrence of complications that are detrimental to the patient. If the family members wish to be notified about delays, they should be encouraged to leave instructions about where they can be contacted. When surgery is completed and the patient is no longer at risk of untoward accidents such as aspiration during extubation, a member of the surgical team should apprise the family of the outcome. At this time, it is appropriate to emphasize particular concerns to the family, such as the need to continue vigilance for infection in a diabetic patient who has undergone foot surgery.
Geerts WH, Bergqvist D, Pineo GF, et al: Prevention of venous thromboembolism. Antithrombotic and thrombolytic therapy, ACCP Evidence-Based Clinical Practice Guidelines (8th Edition). Chest2008;133(Suppl):381S. [PMID: 18574271]
Johnson BF, Manzo RA, Bergelin RO, Strandness DE Jr: Relationship between changes in the deep venous system and the development of the postthrombotic syndrome after an acute episode of lower limb deep vein thrombosis. A one- to six-year follow-up. J Vasc Surg 1995;21:307. [PMID: 7853603]
Lilienfeld DE: Decreasing mortality from pulmonary embolism in the United States, 1979–1996. Int J Epidemiol 2000;29:465. [PMID: 10869318]
Lilienfeld DE, Godbold JH: Geographic distribution of pulmonary embolism mortality rates in the United States, 1980 to 1984. Am Heart J 1992;124:1068. [PMID: 1529881]
McKee MD, DiPasquale DJ, Wild LM, et al: The effect of smoking on clinical outcome and complication rates following Ilizarov reconstruction. J Orthop Trauma 2003;17:663. [PMID: 14600564]
Mini Nutritional Assessment. Available at: http://www.mnaelderly.com/forms/MNA_english.pdf.
Nosanchuk JS: Quantitative microbiologic study of blood salvaged by intraoperative membrane filtration. Arch Pathol Lab Med 2001;125:1204. [PMID: 11520273]
Schneider D, Lilienfeld, DE: The epidemiology of pulmonary embolism: racial contrasts in incidence and in-hospital case fatality. J Natl Med Assoc 2006;98:1967. [PMID: 17225843]
Sweetland S, Green J, Liu B, et al: Duration of the magnitude of the postoperative risk of venous thromboembolism in middle aged women: prospective cohort study. BMJ 2009;339:b4583. [PMID: 19959589]
Warner C: The use of the orthopaedic perioperative autotransfusion (OrthoPAT) system in total joint replacement surgery. Orthop Nurs 2001;20:29. [PMID: 12025800]
SURGICAL MANAGEMENT
![]() Preoperative Care
Preoperative Care
A. The Team Approach
Inclusion of nurses, residents, anesthesiologists, and other members of the surgical team in the planning process can improve the efficiency and therefore affect the outcome of a surgical procedure. Good estimates of the length of the operative procedure and of the patient’s anticipated blood loss and muscle relaxation requirements minimize the risks from anesthesia and surgery. Reviewing the site of the operation and assessing the need for any special supplies and equipment, such as prostheses, lasers, or fracture tables, also contribute to efficiency and optimal results. Special care must be exercised by all members of the operative team to prevent “wrong side” surgery. It is now a JCAHO standard to have the surgical team “mark” the surgical site.
B. Preparing and Positioning the Patient
Once the patient is in the operating room, every effort should be made to make him or her comfortable. A calm, efficient, and professional demeanor by everyone involved is necessary both before and after anesthesia is induced. If the anesthesiologist indicates that placement of the anti-thromboembolic hose, intermittent pneumatic compression stockings, or tourniquets will improve efficiency, these can be put in place prior to induction. Placement of arterial lines, central lines, and Foley catheters should be done after the patient is anesthetized, if possible. Location of the operating table must be adjusted to ensure good lighting, optimize the efficiency of the surgeon and staff, and allow for maintenance of surgical sterile technique.
Positioning of the patient is the responsibility of both the surgeon and the anesthesiologist to facilitate the operation and to ensure the patient’s safety. A perfectly executed operation can be marred by a nerve palsy that results from the failure to pad a remote area appropriately. If the patient is placed in the lateral decubitus position, the peroneal nerve at the knee and the brachial plexus of the downside shoulder girdle must be protected. During shoulder surgery, the surgeon must take care to avoid stretching the patient’s brachial plexus or cervical nerve roots while attempting to maximize the operative field. Similarly, the patient’s shoulder should not be abducted past 90 degrees, and joints with contractures should not be forced into unusual positions. These precautions are particularly necessary in treating rheumatoid patients or older osteoporotic patients. Injury to the extremities and loss of lines can be avoided by careful planning and synchronization when positioning patients into the lateral decubitus position or prone position.
![]() C. Use of Antibiotics
C. Use of Antibiotics
Except in cases in which concern about infection requires unambiguous cultures to be obtained, prophylactic antibiotics have been mandated to be started within 1 hour prior to skin incision by JCAHO. A first- or second-generation cephalosporin antibiotic is considered appropriate for orthopedic procedures. JCAHO has also mandated that prophylactic antibiotics be stopped within 24 hours of orthopedic surgery.
D. Use of a Tourniquet
A tourniquet can be extremely helpful in some procedures and is practically mandatory for others. The tourniquet stops the flow of blood to and from an extremity. To achieve this, the pneumatic tourniquet is inflated to a pressure that must be significantly higher than the arterial pressure because the pressure is dissipated in the soft tissue underneath the tourniquet.
1. Tourniquet size and placement—The tourniquet should be wide enough for the extremity while still permitting adequate exposure of the extremity. Particularly in cases involving surgery on muscles that cross the elbow or knee, the tourniquet should be placed as proximal as possible to ensure the muscles have adequate stretch to permit full joint motion. When a tourniquet is used on a large extremity with a great deal of adipose tissue, care must be taken to ensure that the tourniquet does not slip distally, which could result in wrinkles in the tourniquet and localized pressure on the skin. Slippage can be prevented by applying 5-cm (2-in) adhesive tape to the skin in a longitudinal direction below the cast padding placed under the tourniquet.
2. Tourniquet time and pressure—The effects of tourniquets on tissues are a combination of time and pressure on individual structures. Neural and muscle tissue are most sensitive, with deleterious effects arising from direct pressure to structures and from distal ischemia.
Several considerations are involved in the selection of the level of tourniquet pressure. First, the level must be low enough to avoid pressure damage to sensitive neural structures but high enough so the pressure around the arterial supply to the extremity is greater than systolic pressure (Figure 1–1). Second, if the patient’s blood pressure is labile, a margin of safety is usually necessary. The 2009 Association of Perioperative Registered Nurses (AORN) recommendation is to use a graduated increment in pressure above the measured occlusion pressure. Thus, the incremental increases are 40, 60, and 80 mm Hg for occlusion pressures of <130, 131–190, and >190 mm Hg, respectively. The measured occlusion pressure is defined as the pressure at which arterial flow to an extremity is stopped. If the tourniquet is on an extremity with a great deal of adipose tissue, higher pressures may be necessary to achieve adequate pressure at the artery to stop blood flow. Tourniquets should be calibrated and can be tested with an independent pressure measurement device or alternatively calibrated by palpation of the pulse and gradual elevation of pressure until the pulse disappears.
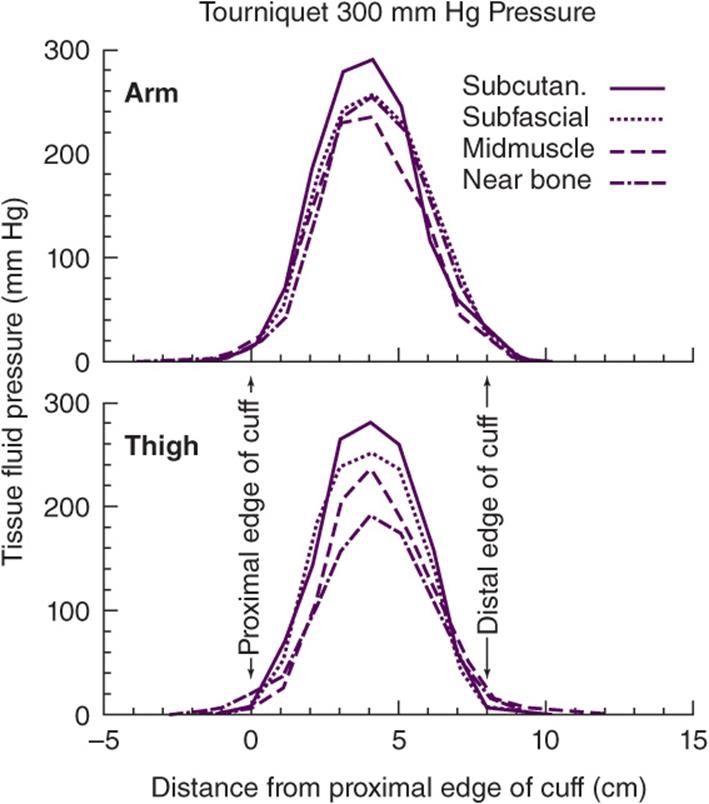
![]() Figure 1–1. Distribution of tissue fluid pressure at four depths beneath pneumatic tourniquet with cuff pressure of 300 mm Hg applied on arms (top) and thighs (bottom). Values represent means for six limbs on each graph. (Reproduced, with permission, from Hargens AR, McClure AG, Skyhar MJ, et al: Local compression patterns beneath pneumatic tourniquets applied to arms and thighs of human cadavers. J Orthop Res 1987;5:247.)
Figure 1–1. Distribution of tissue fluid pressure at four depths beneath pneumatic tourniquet with cuff pressure of 300 mm Hg applied on arms (top) and thighs (bottom). Values represent means for six limbs on each graph. (Reproduced, with permission, from Hargens AR, McClure AG, Skyhar MJ, et al: Local compression patterns beneath pneumatic tourniquets applied to arms and thighs of human cadavers. J Orthop Res 1987;5:247.)
Complications will arise if tourniquets are used at high pressure for too long. The effects can sometimes be mitigated by using wider cuffs and curved cuffs, which allow for higher and more uniform pressure below the tourniquet. A rule of thumb is that tourniquet pressures should not be elevated for longer than 2 hours, and less time is preferable. In a canine study of the muscle tissue distal to the tourniquet, investigators found that 90-minute tourniquet times with 5 minutes between reinflation minimized the ischemic damage. This finding points to the need for efficiency in performing surgical procedures under tourniquet. After tourniquet release, reflex hyperemia and edema are frequently encountered, making closure more difficult. Exsanguination with an Esmarch bandage prior to tourniquet inflation facilitates emptying of large veins of the thigh and arm, although it is not recommended to use an Esmarch in trauma cases. Careful exsanguination may help prevent DVT, especially when reinflation of the tourniquet is planned.
Barwell J, Anderson G, Hassan A, Rawlings I: The effects of early tourniquet release during total knee arthroplasty: A prospective randomized double-blind study. J Bone Joint Surg Br 1997;79:265. [PMID: 9119854]
Classen DC, Evans RS, Pestotnik SL, et al: The timing of prophylactic administration of antibiotics and the risk of surgical wound infection. N Engl J Med 1992;326:281. [PMID: 1728731]
Fernandez AH, Monge V, Garcinuno MA: Surgical antibiotic prophylaxis: effect in postoperative infections. Eur J Epidemiol 2001;17:369. [PMID: 11767963]
Hargens AR, McClure AG, Skyhar MJ, et al: Local compression patterns beneath pneumatic tourniquets applied to arms and thighs of human cadavers. J Orthop Res 1987;5:247. [PMID: 3572594]
Idusuyi OB, Morrey BF: Peroneal nerve palsy after total knee arthroplasty. Assessment of predisposing and prognostic factors. J Bone Joint Surg Am 1996;78:177. [PMID: 8609107]
Noordin S, McEwen JA, Kragh JF Jr, et al: Current concepts review: surgical tourniquets in orthopaedics. J Bone Joint Surg Am 2009;91A:2958. [PMID: 19952261]
Ostman B, Michaelsson K, Rahme H, Hillered L: Tourniquet-induced ischemia and reperfusion in human skeletal muscle. Clin Orthop Relat Res 2004;418:260. [PMID: 15043128]
Pedowitz RA, Gershuni DH, Botte MJ, et al: The use of lower tourniquet inflation pressures in extremity surgery facilitated by curved and wide tourniquets and an integrated cuff inflation system. Clin Orthop Relat Res1993;287:237. [PMID: 8448950]
Sapega AA, Heppenstall RB, Chance B, et al: Optimizing tourniquet application and release times in extremity surgery. J Bone Joint Surg Am 1985;67: 303. [PMID: 3968122]
Wakai A, Winter DC, Street JT, Redmond PH: Pneumatic tourniquets in extremity surgery. J Am Acad Orthop Surg 2001;9:345. [PMID: 11575914]
![]() Operative Care
Operative Care
The surgical team should make every effort to work efficiently during the period between the administration of anesthesia and the conclusion of the final steps of preoperative preparation, which may take from 10 to 30 minutes or longer. It is in the best interests of the patient to minimize the time between onset of anesthesia and the beginning of surgery.
A. Incision Sites and Approaches
Although the surgical wound “heals side-to-side, not end-to-end,” the incorrect placement or the excessive length of a surgical incision for a given procedure only serves to increase surgical trauma to the patient, slow the healing process, and lengthen the rehabilitation period. If there is any doubt about the surgical incision site, roentgenographic examination should be considered. Use of an image intensifier should be considered in obese patients or in patients with previous surgery and retained hardware.
The incision should be made perpendicular to the skin, generally longitudinally, and with a sharp knife. In tumor biopsies, longitudinal incisions are always made. The approach by the surgeon through the subcutaneous fatty layer is variable and depends on the location on the body. In most areas, sharp dissection with a knife through the subcutaneous tissue to the fascial layer is indicated. In the upper extremity and in areas where cutaneous nerves can be troublesome if injured, blunt dissection is used because cutaneous nerves travel in the fatty tissue. Many surgeons prefer blunt dissection with scissors used to spread tissue perpendicular to the wound. Hemostasis is obtained layer by layer. Subcutaneous fat usually is not dissected from the skin, because this might devascularize it.
Surgeons must be extremely careful with the skin, making sure to avoid crushing it when forceps are used. The skin should never be clamped, nor should it be excessively stretched. A larger incision is much better for the skin than extreme tension. Care of the soft tissues includes keeping them moist, avoiding excessive retraction, and being especially careful of neurovascular bundles. Nerves suffer damage from both traction and compression. Nerve palsies and paresthesias can spoil an otherwise well-performed operation in the eyes of both the surgeon and the patient. Care of the cartilage includes keeping it moist because drying has a deleterious effect.
Surgical approaches that go through internerve planes, such as between the deltoid and the pectoralis major, should be used to avoid denervation of muscles. The splitting of muscles in the surgical approach should also be avoided because splitting is generally more traumatic and more likely to denervate the muscle. This rule does not always apply in tumor surgery because it is important to keep tumor cells in a single compartment.
B. Orthopedic Instruments and Drains
It is mandatory that tools be sharp at all times because the sharpness enables the surgeon to avoid the excessive pressure that creates problems by plunging into the depths of the wound. When an osteotome or elevator is needed, the concurrent use of a hammer is preferred because achieving exact control is possible by the strength and number of hammer taps, whereas control is difficult to achieve by pushing on an osteotome. With drill points and power saws, the sharpness of the instruments should be maintained to reduce necrosis secondary to heating and to facilitate the operation. Unless using a drill guide, the surgeon should start drilling bone in a perpendicular direction even though the final direction may be at some angle to the direction of the bone. This prevents slipping off the desired bone entry point. Holes in long bones are stress concentration sites. Care should be taken to minimize the likelihood and degree of stress concentration by rounding holes and using drill holes to terminate saw cuts (Figure 1–2). When holes were made in bone, especially in the lower extremity, the patient should be advised against torsional loading.
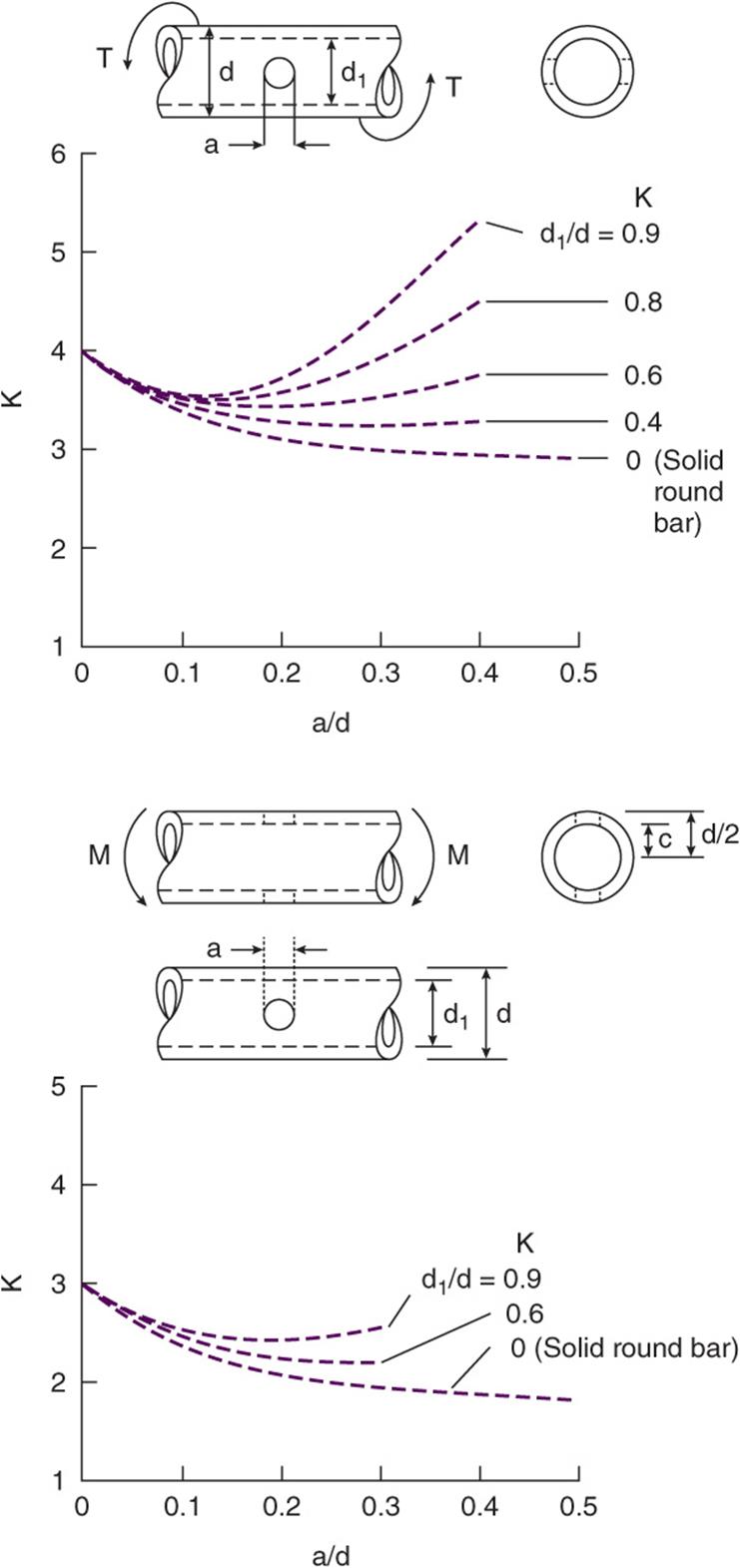
![]() Figure 1–2. Stress concentration factors for torsion (top) or bending (bottom) of a round bar or tube with a transverse hole, where a = the size of the hole; d = the outside diameter of the tube; d1 = the inside diameter of the tube; K = the stress concentration factor, defined as the factor by which stress is increased by the hole; M = the bending moment; and T = the torsional load. (Modified and reproduced, with permission, from Peterson RE: Stress Concentration Factors: Charts and Relations Useful in Making Strength Calculations for Machine Parts and Structural Elements. New York, NY: Wiley; 1974.)
Figure 1–2. Stress concentration factors for torsion (top) or bending (bottom) of a round bar or tube with a transverse hole, where a = the size of the hole; d = the outside diameter of the tube; d1 = the inside diameter of the tube; K = the stress concentration factor, defined as the factor by which stress is increased by the hole; M = the bending moment; and T = the torsional load. (Modified and reproduced, with permission, from Peterson RE: Stress Concentration Factors: Charts and Relations Useful in Making Strength Calculations for Machine Parts and Structural Elements. New York, NY: Wiley; 1974.)
Obtaining hemostasis in bone can be troublesome, and the use of microcrystalline collagen is preferred to bone wax because of the foreign body response. Postoperative bleeding is common from bony surfaces. Despite the traditional use of drains by surgeons, evidence is accumulating that at least for some operations, such as total hip or total knee replacement, wound drainage may not be necessary and may lead to increased blood loss. If drains are used, they should be secured to prevent accidental removal and should be large enough to prevent clogging by clot formation. Drains are generally removed within 48 hours of surgery unless they are used to eliminate dead space.
C. Closure and Dressing
Wound closure should be done quickly and efficiently to minimize total operative and anesthesia time. It should also be accomplished carefully to avoid damage to the skin. When a previous scar is entered, it is sometimes worthwhile to remove scar tissue from the edge of the skin, as well as from the subcutaneous tissue, to provide a more vascular area for healing. Meticulous subcutaneous wound closure is necessary to avoid tension on the skin in many areas on the extremities. Four-throw square knots are important for knot security, especially when plans call for use of continuous passive motion machines or early motion, which may apply repetitive stress to the wound before it heals. Barbed sutures, while eliminating knots, may not be as strong in maintaining tissue apposition. Tissue adhesives are an advent in wound closure. One study found sutures were significantly better than adhesives for minimizing dehiscence of incisions, although the adhesives generally resulted in a more cosmetic wound.
Dressings should be padded with cotton or gauze to discourage the formation of hematomas. Closed wound suction drainage does not change outcome and is associated with a higher infection rate and higher transfusion rate in total knee arthroplasty. Tape should be avoided when possible because it sometimes causes allergic reactions, and also the combination of wound swelling and shear from the tape can lead to blistering and other problems.
Batra EK, Franz DA, Towler MA, et al: Influence of surgeon’s tying technique on knot security. J Appl Biomater 1993;4:241. [PMID: 10146307]
Brown MD, Brookfield KF: A randomized study of closed wound suction drainage for extensive lumbar spine surgery. Spine 2004;29:1066. [PMID: 15131430]
Coulthard P, Esposito M, Worthington HV, et al: Tissue adhesives for closure of surgical incisions. Cochrane Database Syst Rev 2010;2:CD004287. [PMID: 20464728]
Hazarika S, Bhattacharya R, Bhavikatti M, Dawson M: A comparison of post-op haemoglobin levels and allogeneic blood transfusion rates following total knee arthroplasty without drainage or with reinfusion drains. Acta Orthop Belg 2010;76:74. [PMID: 20306968]
Minnema B, Vearncombe M, Augustin A, et al: Risk factors for surgical site infections following primary total knee arthroplasty. Infect Control Hosp Epidemiol 2004;25:477. [PMID: 15242195]
Ong CC, Jacobsen AS, Joseph VT: Comparing wound closure using tissue glue versus subcuticular suture for pediatric surgical incisions: a prospective randomized trial. Pediatr Surg Int 2002;18:553. [PMID: 12415411]
Torcchia AM, Aho HN, Sobol G: A re-exploration of the use of barbed sutures in flexor tendon repairs. Orthopedics 2009;32:10. [PMID: 19824603]
POSTOPERATIVE CARE
![]() Inpatient Care
Inpatient Care
Postoperative care begins in the postanesthesia room and is the same for both inpatients and outpatients. It is imperative that the orthopedic surgeon takes an active and early role in the treatment of the postoperative patient, including pain management, blood management, and DVT prophylaxis. As soon as practicable, neurologic and vascular evaluation of the operated area should be made. Sensory and motor exam of the pertinent upper or lower extremity nerves should be documented as soon as practical. Early vascular surgery consultation is indicated if pulses are absent or diminished. The wound site should be checked for excessive drainage, and, when appropriate, compartment syndrome should be considered. The general medical condition of the patient, although primarily the concern of the anesthesiologist, should be evaluated to be sure the anesthesiologist is aware of special concerns regarding the individual patient.
During the subsequent postoperative period, orthopedic aspects of care are relatively routine for most procedures. The main responsibility of the orthopedic surgeon is the evaluation of the vascular and neural status of the extremities affected by the surgery, as well as pain control and vigilance for disorders such as DVT or PE. The frequency of postsurgical examinations depends on the clinical setting. Hourly examinations may be necessary in the face of a potential compartment syndrome, although daily examinations are usually adequate. Epidural morphine analgesia may significantly mute or alter the pain picture in a compartment syndrome, making accurate clinical evaluation difficult, if not impossible, in the immediate postoperative period.
A. Pain Management
Pain management is a major issue in the United States. There has been a concern that patients are undermedicated and not achieving adequate pain control. The public has embraced this concept, resulting in litigation and disciplinary action by state medical boards for undermedication. Physicians traditionally were seen as being reluctant to prescribe narcotic medication as a result of concerns that they would be disciplined by state medical boards. This concept has led to a major initiative by the JCAHO to address pain control as a patient “right.” JCAHO mandates that pain control be a factor in the total evaluation of the patient and pain evaluation be performed as the fifth vital sign. The scale used is the numeric scale from 0 to 10, similar to the visual analogue scale, with 0 being no pain and 10 being unbearable pain. Patients typically have no real standards upon which to assign their pain scores, resulting in frequent use of a “10” score, or higher. This scale can be explained to the patient in more understandable terms as follows: 1–3 is “nuisance” pain, 4–6 is “distracting” pain, 7–9 is “disabling” pain, and 10 is “worst possible pain.” This more functional scale is easier to use by the patient. Acceptable pain levels are defined as 4 and below.
Pain is a very subjective sensation that is an emotional response to the process of nociception: the sum of four separate components beginning with tissue damage, which results in the first component, transduction to a nerve impulse. The next component is transmission to the spinal cord, where the third component occurs: modulation. This modulated signal is then perceived in the cerebral cortex (perception). Pain perception depends on culture, ethnicity, and gender. It is nonlinear, in that a stimulus two times higher does not necessarily result in twice the pain. Pain perception is also based on patient expectations. Studies show that preoperative patient education can reduce patients’ pain after major (eg, total knee arthroplasty [TKA]) orthopedic surgery.
Traditional postoperative pain management included the administration of intravenous (IV) or intramuscular narcotic analgesics until oral narcotics were able to control the pain. Patient-controlled analgesia (PCA) is now a mainstay. In this system, morphine is usually used as the analgesic and typically administered IV at a rate of 1 mg/h with a patient-controlled dose of 1 mg, which can be administered as often as every 10 minutes. Doses can be increased or decreased to tailor the dose to the patient. Dosing at this level can result in depressed respiration in some patients. However, more cautious dosing can result in insufficient pain relief that can stress the heart, leading to myocardial ischemia in some patients. Other problems can result from traditional pain management with narcotics. Patient rehabilitation can be delayed; nausea, vomiting, constipation, hallucinations, and disorientation can result in lengthened hospital stay and patient dissatisfaction.
Alternative postoperative analgesic methods have been utilized. These include epidural and intrathecal administration of local anesthetics and analgesics on a continuous and one-shot basis. These methods have the potential of providing significant pain relief but must be balanced against the alternatives available and the drawbacks that each presents. The one-shot method of adding morphine to the spinal or epidural anesthetic provides pain relief for a limited time, usually on the order of 12–24 hours, although a longer acting form of morphine (DepoDur) has come on the market for single-injection epidural use, providing pain relief for up to 48 hours. It has the additional problem of limiting additional narcotic analgesia by other routes because overdosing may be possible. Long-term use of continuous epidural or intrathecal analgesia poses the problem of inhibiting rehabilitation. Nurses and physical therapists tend not to mobilize patients with catheters into the spinal canal, and in some hospitals, these patients are mandated to go to the intensive care unit. Nerve blocks and injections into joint cavities are limited by the length of action of the local anesthetic agent. Nerve blocks must address all nerves to an area to control postoperative pain. Hence, studies show best results with a longer-term effect achieved by the use of pumps that provide a continuous anesthetic flow into the joint or body cavity, with some designs allowing an intermittent bolus for more pain relief. These pumps typically use a long-acting agent such as bupivacaine (0.25% or 0.5%) and infuse at the rate of 2 or more mL/h. Ropivacaine is reported to have vasoconstrictive properties and less cardiotoxicity than bupivacaine, although at a higher cost. Studies suggest damage to chondrocytes from exposure to local anesthetics such as lidocaine, bupivacaine, and ropivacaine, with possibly even a single injection. Thus, treatment of postoperative pain with infusions or infusion pumps should be reserved for total joint replacements or incision sites unconnected to a joint.
In the past, nonnarcotic pharmacologic treatment of acute postoperative pain was largely restricted to ketorolac, which can be administered by the IV or intramuscular (IM) route in the patient who is restricted in oral intake. Although ketorolac is an effective analgesic, demonstrated through reduction in the need for morphine, it also increases the perioperative blood loss due to its COX-1 activity on platelets. After oral intake is permitted, other NSAIDs can be used for analgesics. Neither ketorolac nor other NSAIDs play a routine role in the acute pain management for most orthopedic surgical patients because of the effect these drugs have on the platelets and subsequent blood loss. The availability of COX-2–selective NSAIDs has opened up the possibility of using these drugs as major analgesics for postoperative pain control, without fear of bleeding problems. These drugs act to reduce the need for narcotics with improved pain relief and decreased narcotic side effects. On the horizon are new COX-2 drugs that can be administered parenterally, and these drugs may be of major assistance in the management of early postoperative pain. Such a drug is parecoxib, which is the prodrug for valdecoxib (available in Europe, but not available in the United States). The use of highly specific COX-2 inhibitors as analgesics came into question with the withdrawal of rofecoxib and valdecoxib from the market because of concern over increased cardiovascular events with long-term use. At this time, other less specific NSAIDs may be considered as alternatives (celecoxib, diclofenac, meloxicam, etodolac) because their effect on platelet function is minimal.
Other analgesics and techniques do not get sufficient recognition for their role in pain control. Acetaminophen is thought to be a central prostaglandin synthase inhibitor and thereby achieves significant relief of pain. It can be tolerated in doses up to 4 g/day, and because it does not act in the same pathway as narcotics, its effect is additive to that of morphine or other narcotics and can reduce the requirement for narcotics. Another analgesic that should be used more often for analgesia is tramadol. This analgesic has very low abuse potential but provides significant analgesia, acting through inhibition of norepinephrine reuptake as well as a weak μ-agonist (similar to morphine) action. Again this mechanism of action is additive to that of traditional opioids and acetaminophen in its analgesic effect. Glucocorticoids are naturally increased in periods of stress such as surgery and are provided exogenously for those patients with suppressed adrenal function. One study showed an increase in cortisol production of 17-fold after TKA, but no such increase after knee arthroscopy. Divided doses of approximately 200 mg of hydrocortisone (8 days normal production) are typically prescribed for such patients. High doses (20 mg) of dexamethasone (equivalent to 400 mg of hydrocortisone) reduce the early postoperative pain in tonsillectomy patients. Although such doses may reduce postoperative nausea, swelling, and pain, as well as create a feeling of well-being, an increased susceptibility to infection may result from longer term dosing. Short courses of relatively high doses of glucocorticoids may be beneficial in reducing postoperative pain. Other methods of pain control may be indirect, such as controlling swelling and pain through hemostasis and cold therapy. Hemostasis may be achieved through the use of bone wax on cancellous bone or through the use of fibrin glue. Vasoconstriction from cold therapy can reduce swelling and also have a direct effect on nociceptive transduction.
A comprehensive approach to pain management can lead to beneficial effects. Multimodal analgesic regimens are suggested using several analgesics that address different points in the nociception process. Combinations of medications can include narcotics, acetaminophen, tramadol, COX-2 inhibitors, and local anesthetics administered through the use of pain pumps. Peripheral nerve blocks and subarachnoid morphine blocks can assist in control of pain in the early postoperative period. Injections of local anesthetics and steroids into the pericapsular tissues can also be helpful. Consideration should be given to administering medications in the preanesthesia room to preempt the pain of surgery. This can also assist in diminishing peripheral sensitization that occurs with tissue damage. In addition to pharmacologic interventions, patient education can reduce preoperative anxiety, reducing pain and increasing satisfaction.
Bianconi M, Ferraro L, Traina GC, et al: Pharmacokinetics and efficacy of ropivacaine continuous wound instillation after joint replacement surgery. Br J Anaesth 2003;91:830. [PMID: 14633754]
Chu CR, Coyle CH, Chu CT, et al: In vivo effects of a single intraarticular injection of 0.5% bupivacaine on articular cartilage. J Bone Joint Surg 2010;92A:599. [PMID: 20194318]
Cook P, Stevens J, Gaudron C: Comparing the effects of femoral nerve block versus femoral and sciatic nerve block on pain and opiate consumption after total knee arthroplasty. J Arthroplasty 2003;18:583. [PMID: 12934209]
Grishko V, Xu M, Wilson G, Pearsall AW 4th: Apoptosis and mitochondrial dysfunction in human chondrocytes following exposure to lidocaine, bupivacaine, and ropivacaine. J Bone Joint Surg2010;92A:609. [PMID: 20194319]
Hartrick CT, Hartrick KA: Extended release epidural morphine (DepoDur): review and safety analysis. Expert Rev Neurother 2008;8:1641. [PMID: 18986234]
Kuritzky L, Weaver A: Advances in rheumatology: coxibs and beyond. J Pain Symptom Manage 2003;25(Suppl2):s6. [PMID: 12604153]
Leopold SS, Casnellie MT, Warme WJ, et al: Endogenous cortisol production in response to knee arthroscopy and total knee arthroplasty. J Bone Joint Surg Am 2003;85:2163. [PMID: 14630847]
Mallory TH, Lombardi AV Jr, Fada RA, et al: Pain management for joint arthroplasty: preemptive analgesia. J Arthroplasty 2002;17:129. [PMID: 12068423]
Parvizi J, Porat M, Gandhi K, et al: Postoperative pain management techniques in hip and knee arthroplasty. Instr Course Lect 2009;58:769. [PMID: 19385585]
Rasmussen S, Kramhøft MU, Sperling KP, Pedersen JH: Increased flexion and reduced hospital stay with continuous intraarticular morphine and ropivacaine after primary total knee replacement: open intervention study of efficacy and safety in 154 patients. Acta Orthop Scand 2004;75:606. [PMID: 15513495]
Sinatra RS, Torres J, Bustos AM: Pain management after major orthopedic surgery: current strategies and new concepts. J Am Acad Ortho Surg 2002;10:117. [PMID: 11929206]
Sjoling M, Nordahl G, Olofsson N, Asplund K: The impact of preoperative information on state anxiety, postoperative pain and satisfaction with pain management. Patient Educ Couns 2003;51:169. [PMID: 14572947]
B. Deep Venous Thrombosis/Pulmonary Embolus
DVT, a potentially life-threatening disorder, frequently accompanies orthopedic surgery. It is much more of a problem for total joint replacements, spine surgery, and lower extremities immobilized after surgery, but can occur without surgery in patients having arthroscopy or cast treatment for fractures or even Achilles tendon ruptures. This is one of the expected risks after surgery and cast treatment. It is such an important issue that since 2006, JCAHO has mandated that hospitalized patients be screened and treated to prevent DVT. Venous thromboembolic phenomenon can result in three problems: postphlebitic (or postthrombotic) syndrome, nonfatal PE, and fatal PE. It is necessary to put the risks of PE into appropriate perspective because, contrary to prevailing assumptions in the public and among orthopedic surgeons, PE can occur without surgery (Table 1–2). The risk of having a PE depends on a number of risk factors, including age, weight, the presence of varicose veins, immobility, smoking, previous DVT, joint replacement, the season of the year, estrogen therapy, and the location. There is an uncertain relationship between DVT and the probability of having a PE. Obviously one cannot have a PE without having a clot, but which clots are likely to break off and become emboli and which ones will cause problems are still unresolved issues. It is thought that thigh clots are more important than calf clots because of their size and the potential damage they can do. It is generally conceded, however, that DVT is a marker for PE, and that is the surrogate variable used to determine the effectiveness of treatment of PE. A nonfatal PE can cause cor pulmonale, but this is thought to be an unlikely circumstance, and it is speculated that nonfatal PE would result in a residual effect in the range of 0.1–0.01% of cases. DVT itself is thought to be a significant problem that results in incompetence of the valves in the deep veins of the calf and thigh. This results in persistent edema, which can progress to brawny edema and ulceration over time. However, many things are thought to cause these changes in addition to DVT. There is an uneven geographic distribution of fatal PE without surgery in the United States, with the West Coast census region having the lowest fatal PE rate. The rate of fatal PE increases with age, although age may simply be a marker for health and activity level. The rate of fatal PE in the general population older than 65 years is in the range of 0.03%, whereas approximate total joint PE rates are typically approximately 0.3%. Thus, there is a 10-fold increase in risk of having a fatal PE with a total hip or knee replacement.
Table 1–2. Rates of complications associated with total hip replacement at the Mayo Clinic.

Three classes of drugs can be used for chemoprophylaxis of DVT in the United States: warfarin (the vitamin K inhibitor), the low-molecular-weight heparins (dalteparin, enoxaparin, and similar drug fondaparinux), and the platelet aggregation inhibitors (aspirin, naproxen, other NSAIDs). Each approach has its advantages and disadvantages. Sodium warfarin has a slow onset of action, sometimes taking several days to reach therapeutic levels, but its oral route of administration is convenient. However, monitoring of the prothrombin time is necessary to ensure appropriate therapeutic levels. The low-molecular-weight heparins do not affect the prothrombin time or the partial thromboplastin time but do affect factor IIa and Xa levels. These do not have to be monitored because the medications are given in standard doses. These medications are provided parenter-ally. Both warfarin and the low-molecular-weight heparins are associated with bleeding problems. Aspirin, naproxen, and other NSAIDs have proponents who recommend them because of their relative safety, but they are probably not effective in prevention of DVT. Mechanical means of preventing DVT include compression hose and intermittent pneumatic compression. These have recently been demonstrated to be as efficacious as chemoprophylaxis.
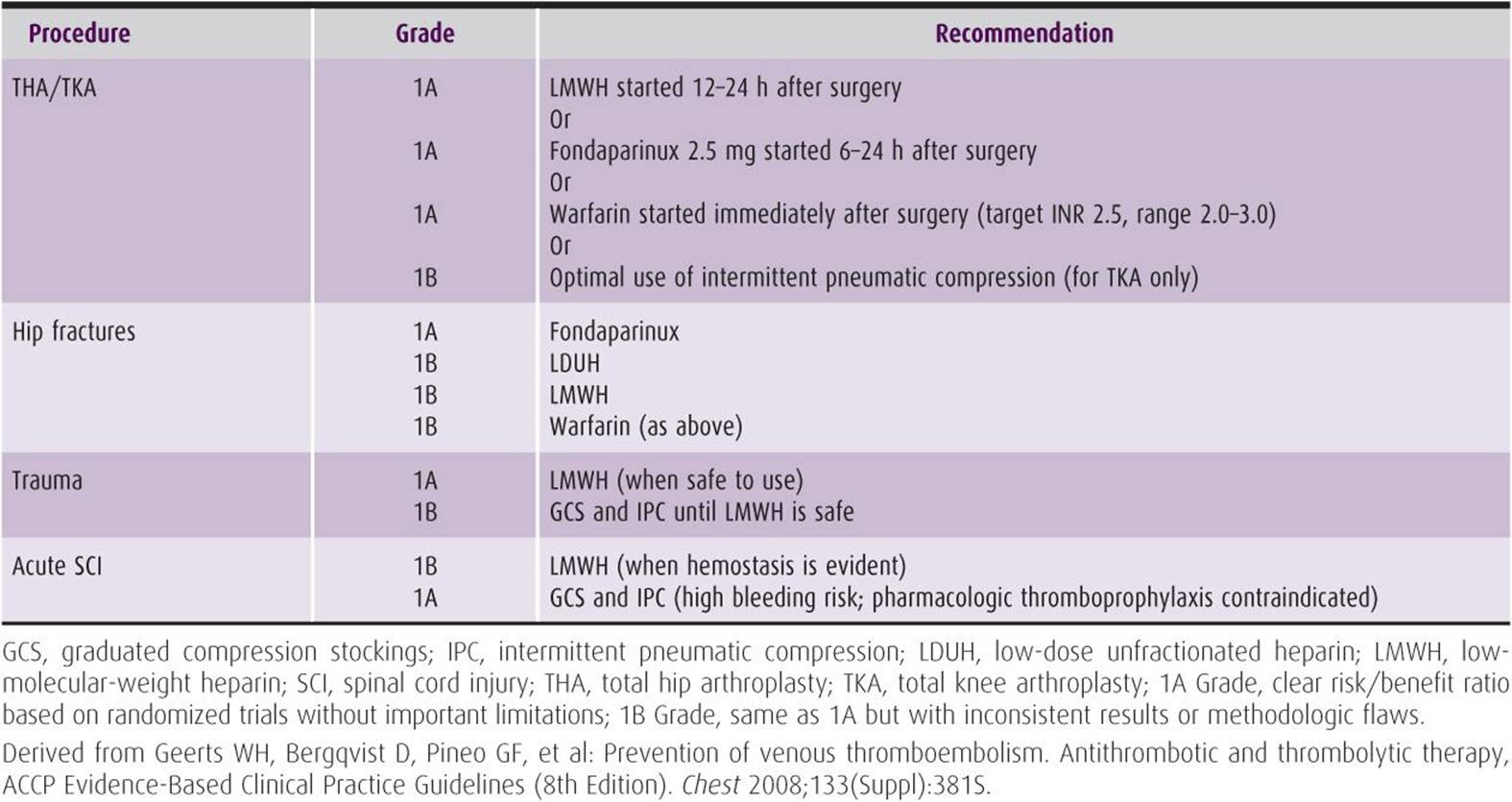
The American College of Chest Physicians regularly performs and publishes meta-analyses of the data available on DVT with updated recommendations. Generally, for orthopedic indications after high-risk surgery, warfarin with an international normalized ratio (INR) of 2–3, a low-molecular-weight heparin starting 12–24 hours after surgery, and elastic stockings and intermittent pneumatic compression are useful as supplemental protection against DVT. The recommended period is a minimum of 7 days. Occasionally, use of heparin or vena cava filters is recommended in high-risk situations. Table 1–3 lists the current recommendations.
Table 1–3. Recommendations for management of DVT prophylaxis for high-risk orthopedic patients.
The community standard in orthopedic surgery probably differs somewhat from that recommended by the American College of Chest Physicians. Newer orthopedic literature seems to suggest that warfarin is the drug of choice but with lower INR values. However, the choice of prophylactic agent is made by the doctor and the patient and is influenced by their interpretation of the risk of thromboembolism and bleeding problems.
Both warfarin and heparin, either low-molecular-weight (LMWH) or regular, have problems that can cause catastrophic side effects in rare cases. Warfarin can cause skin necrosis and venous limb gangrene syndromes unrelated to the operative site. Heparin can induce thrombocytopenia. This is apparently an immunoglobulin G (IgG) antibody formation that occurs 5–10 days after starting heparin (including LMWH) and can result in a hypercoagulable state that can result in serious problems of coagulation in unintended areas. Some new agents are becoming available, some of which are on the market at the time of this writing but are not indicated for DVT prophylaxis. These drugs are related to the antithrombin drug produced by leeches. Two of these are desirudin and bivalirudin, and they are indicated for anticoagulation in the presence of heparin-induced thrombocytopenia.
In addition, dabigatran is an antithrombin drug that may soon be available for DVT prophylaxis as an oral prescription (presently available in Europe). Another drug, rivaroxaban, an oral factor Xa inhibitor, is approved for use in Canada and Europe and has been recommended for approval in the United States by a Food and Drug Administration advisory panel. A pentasaccharide (fondaparinux) is approved for DVT prophylaxis and acts in a manner similar to heparin.
1. Diagnosis—DVT is diagnosed with ultrasound in the postsurgical patient with calf swelling or with Homan’s sign in the appropriate clinical setting. Several risk factors can be elicited from the history to increase the suspicion of DVT. These include immobilization, lower extremity or pelvic surgery (in the previous 4 weeks), previous history of DVT, and history of cancer. Ultrasound is a reliable, noninvasive screen for DVT of the lower extremity veins and has replaced the venogram as the gold standard for diagnosing DVT. Testing for PE has also evolved. In nonsurgical patients, D-dimer can be helpful in the diagnosis of PE, and the risk of PE continues for weeks after surgery, so there may be a role for it in the late postoperative period. Previously, ventilation/perfusion scans were the standard method, followed by pulmonary angiography, if the probability was intermediate. Now spiral CT is quite reliable but is still only reported to be 70% sensitive and 91% specific. In outpatients with a normal ultrasound and a normal lung scan, spiral CT has only a 7% false-positive rate and 5% false-negative rate. Furthermore, evidence from a preliminary study suggests that fibrin monomer discriminates between total hip arthroplasty patients with PE and those without PE. The D-dimer was also higher in PE patients but not significantly until 7 days postoperatively.
Colwell CW: The ACCP guidelines for thromboprophylaxis in total hip and knee arthroplasty. Orthopedics 2009;32 (12 Suppl):67. [PMID: 20201479]
Colwell CW, Froimson MI, Mont MA, et al: Thrombosis prevention after total hip arthroplasty: a prospective, randomized trial comparing a mobile compression device with low-molecular-weight heparin. J Bone Joint Surg Am2010;92A:527. [PMID: 20194309]
Freedman KB, Brookenthal KR, Fitzgerald RH Jr, et al: A meta-analysis of thromboembolic prophylaxis following elective total hip arthroplasty. J Bone Joint Surg Am 2000;82:929. [PMID: 10901307]
Geerts WH, Pineo GF, Heit JA, et al: Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004;126:338S. [PMID: 15383478]
Hong MS, Amanullah AM: Heparin-induced thrombocytopenia and thrombosis. Rev Cardiovasc Med 2010;11:13. [PMID: 20495512]
Johnson BF, Manzo RA, Bergelin RO, Strandness DE Jr: Relationship between changes in the deep venous system and the development of post thrombotic syndrome after an acute episode of lower limb deep vein thrombosis: a one- to six-year follow-up. J Vasc Surg 1995;21:307. [PMID: 7853603]
Lilienfeld DE: Decreasing mortality from pulmonary embolism in the United States, 1979–1996. Int J Epidemiol 2000;29:465. [PMID: 10869318]
Lilienfeld DE, Godbold JH: Geographic distribution of pulmonary embolism with mortality rates in the United States, 1980–1984. Am Heart J 1992;124:1068. [PMID: 1529881]
Mont MJ, Eurich DT, Russell DB, et al: Post-thrombotic syndrome after total hip arthroplasty is uncommon. Acta Orthop 2008;79:794. [PMID: 19085497]
Nazarian RM, Van Cott EM, Zembowicz A, Duncan LM: Warfarin-induced skin necrosis. J Am Acad Dermatol 2009;61:325. [PMID: 19615543]
Perrier A, Howarth N, Didier D, et al: Performance of helical computed tomography in unselected outpatients with suspected pulmonary embolism. Ann Intern Med 2001;135:88. [PMID: 11453707]
Rafee A, Herlikar D, Gilbert R, et al: D-dimer in the diagnosis of deep vein thrombosis following total hip and knee replacement: a prospective study. Ann R Coll Surg Engl 2008;90:123. [PMID: 18325211]
Schneider D, Lilienfeld DE: The epidemiology of pulmonary embolism: racial contrasts in incidence and in-hospital case fatality. J Natl Med Assoc 2006;98:1967. [PMID: 17225843]
Stevenson M, Scope A, Holmes M, et al: Rivaroxaban for the prevention of venous thromboembolism: a single technology appraisal. Health Technol Assess 2009;13(Suppl 3):43. [PMID: 19846028]
Turpie AG, Gallus AS, Hoek JA: A synthetic pentasaccharide for the prevention of deep-vein thrombosis after total hip replacement. N Engl J Med 2001;344:619. [PMID: 11228275]
![]() Outpatient Care
Outpatient Care
Economic realities today mandate earlier discharge from the hospital after some procedures and after outpatient surgery in procedures previously done on an inpatient basis. This trend suggests that patients must take more responsibility for their care, and surgeons must provide outpatient access for patients previously treated as inpatients. The indications for discharge have broadened just as the reasons for admission have narrowed. The reasons for keeping a postoperative patient in the acute-care setting are few. The main indications for hospitalization are pain control requiring parenteral narcotics, presence of hemodynamic instability, a need for traction, or a need for frequent physician observation (drains, infection, etc.). Even extended administration of IV antibiotic therapy is not an adequate reason for an acute-care stay. Thus timing of follow-up visits is important to ensure that the patient is not only unnecessarily inconvenienced but also does not suffer delayed recognition of a complication. In most cases, the first visit should be for suture removal (10–14 days). Again, economic realities mandate a 90-day follow-up as part of the global surgical fee. Follow-up for a total hip replacement patient might be at 2 weeks, 6 weeks, and 12 weeks after surgery. Longer or shorter intervals may be necessary, depending on how the patient is progressing and how much external support the patient is receiving (physical therapy, home nurse visits, home caregivers, and home environment). Joint-replacement patients should be followed up at least yearly on a permanent basis after the first 5 or so years. The American Academy of Orthopedic Surgeons recommends prophylactic antibiotics for joint-replacement patients for procedures such as dental cleaning in which bacteremia may occur for life, especially when immune compromise is likely (eg, diabetes or renal transplant).
Long-term follow-up for patients with plates, screws, pins, rods, or other fracture devices is not typically necessary after healing of the fracture and rehabilitation of the affected muscles and joints. Antibiotic prophylaxis is not necessary for these patients. In cases of painful hardware, removal may be indicated after healing. Removal of hardware in older (more than 75 years) patients is generally not indicated. In younger (less than 50 years), active patients, hardware removal may be justified to reduce the stress concentration or stress shielding effects of the metal devices to prevent fracture prophylactically. An adequate period (12 weeks or more, depending on activity) of stress protection, especially in torsion, is indicated to reduce the risk of fracture through defects incurred by the bone during removal of hardware. For a detailed discussion of rehabilitation, see Chapter 12, “Rehabilitation”.
Pacheco RJ, Buckley S, Oxborrow NJ, et al: Gluteal compartment syndrome after total knee arthroplasty with epidural postoperative analgesia. J Bone Joint Surg Br 2001;83:739. [PMID: 11476317]
Richards H, Langston A, Kulkarni R, Downes EM: Does patient controlled analgesia delay the diagnosis of compartment syndrome following intramedullary nailing of the tibia? Injury 2004;35:296. [PMID: 15124799]
Yang J, Cooper MG: Compartment syndrome and patient-controlled analgesia in children- analgesic complication or early warning system. Anaesth Intensive Care 2010;38:359. [PMID: 20369773]
![]() Blood Loss and Replacement
Blood Loss and Replacement
Because blood replacement is now a complicated issue, it is fortunate that not all orthopedic procedures require blood replacement. In California, the surgeon is obligated to give the patient a brochure from the state that describes the blood management options available to the surgeon and the patient when blood transfusion is likely after surgery. Patient involvement in the decision on how to manage blood loss is certainly a good idea.
The data on when to transfuse are conflicting, however, and generally the decision is based on the physician’s clinical assessment to determine the need for transfusion. This uncertainty is reflected in the variability in the postoperative transfusion “trigger,” as shown by the percentages of patients receiving blood varying from 16 to 87% for total hip arthroplasty and 12 to 87% for TKA in one study; it should be noted that these rates also reflect differences in blood loss for these procedures at various hospitals. Blood volume is approximately 7–8% of body weight, or approximately 5 L in a 70-kg individual. Normal individuals can be resuscitated from acute blood losses of up to 25% with crystalloid/colloid. Greater blood losses can be tolerated if the euvolemic state is maintained, but transfusion should be considered. The status of the clotting system must be monitored in the acute blood loss phase to prevent accelerated blood loss. Blood loss in the postoperative subacute phase can be managed with volume replacement and evaluation of symptomatology to determine the need for transfusion of red cell mass. Patients at risk of stroke or myocardial infarction or those with decreased cardiac output may need transfusion at higher hemoglobin levels. Younger (less than 50 years), healthier patients may tolerate lower hemoglobin levels unless they have postural hypotension, tachycardia, dizziness, or fainting.
A. Criteria for Blood Transfusion
The decision to transfuse in the immediate postoperative period is predicated on numerous factors, including age, medical condition and cardiac status, estimated blood loss, projected blood loss, availability of blood (autologous, designated donor, or bank), and the patient’s perception of risk. Consideration of all factors argues against transfusion in the younger (less than 50 years) or healthier patient until the patient has a hematocrit level of 20–22% or has symptoms that include tachycardia, early and postural hypotension, and dizziness or fainting. Older (more than 60 years) patients at risk of stroke or myocardial infarction would be candidates for transfusion at higher hematocrit levels or with a lower threshold of symptoms.
B. Strategies for Minimizing the Risks Associated With Blood Transfusion
Blood loss is an inevitable part of surgery. With the realization that the banked blood supply is at low risk, but still at risk, of containing infectious agents, strategies to minimize the risk of transmission have been developed.
An obvious method of accomplishing this goal is to reduce blood loss. Anesthetic techniques to reduce mean arterial blood pressure can reduce blood loss by reducing the time of surgery as well as the actual blood loss. The patient has to be counseled to avoid antiplatelet drugs in the period prior to surgery. These medications include baby aspirin and clopidogrel but also all of the ubiquitous NSAIDs that are in over-the-counter analgesics, cough and cold remedies, and arthritis medications. In the operative period, topical agents such as bone wax, Gelfoam and similar collagen products, thrombin, tranexamic acid and aminocaproic acid (antifibrinolytics), and fibrin glue should be considered. Tranexamic acid can be administered IV or locally to help control bleeding. Surgical technique should be efficient and meticulous to reduce time and therefore blood loss. The patient should be positioned to minimize venous pressure and blood loss, such as closing a total knee in flexion or positioning a postoperative total knee in flexion to reduce blood loss.
Presurgical banking of autologous blood by the patient (with or without hematopoietic growth factors), immediate preoperative autodonation by hemodilution, and salvage of the patient’s intraoperative and postoperatively lost blood with infusion of either washed or unwashed red cells can reduce the patient’s exposure to the risks of designated donor blood or homologous banked blood. The problems with autologous blood begin with the cost, but there are other issues. Older (more than 70 years) patients sometimes do not tolerate the anemia from donation. Perhaps the greatest risks are bacterial contamination and clerical error, in which a patient gets a potentially fatal ABO-incompatible unit instead of his or her own. Autologous blood that is not used is discarded and not put into the general blood bank pool.
Preoperative hemodilution has the cost associated with the operating room time to draw off the blood and that of the anesthesiologist in supervising the process. Preoperative hematocrit can be boosted through parenteral erythropoietin, which can minimize the effect of surgical blood loss. Erythropoietin is estimated to cost $900 per unit of blood saved, which is more than the cost of autologous blood at $300–400/unit. Furthermore, there may be risks with abnormally high hematocrits. Thus, it is only considered when there is little other choice, such as for surgery on Jehovah’s Witnesses who refuse transfusions.
Despite initial resistance and continued questions about cost-effectiveness by blood bank officials, autologous blood donation has achieved considerable acceptability from patients, physicians, and blood bank administrators. There are disadvantages of autologous donation that counterbalance the obvious advantages of eliminating transfusion-related disease and incompatibility. These are possible bacterial contamination of the blood, perioperative anemia with increased risk of transfusion, administrative error resulting in blood incompatibility from receiving the wrong blood, cost, and wastage of autologous blood that is not used. Blood can be stored for 35 days or can be frozen as a red cell mass for up to 1 year, but loss in viability of the red cells occurs with both storage methods. Use of autologous blood can eliminate the need for banked blood for many but not all orthopedic patients. Some patients, for example, have marginal laboratory test results (eg, Hgb level of 10 g/dL and hematocrit level of 30%) that preclude their predonation of blood. The ability of patients to predonate blood and the amount of blood donated can sometimes be increased through the use of recombinant human erythropoietin therapy. Injections can be given twice weekly and may result in a higher red cell mass collected and a higher hematocrit level at the time of hospital admission. Although expensive, this therapy can be of benefit to patients, especially those who have blood types that are difficult to match or have religious beliefs that conflict with the practice of receiving blood from others.
Red blood cells can be salvaged by suction in the operating room or collected via surgical drains in the recovery room. Adequate loss of blood must be present to make these procedures cost effective. Blood salvage is probably effective (absolute reduction in risk of receiving an allogeneic red cell transfusion, 21%, with a saving of 0.68 units of allogeneic blood per patient) in minimizing perioperative allogeneic transfusion, but should be reserved for cases with high expected blood loss (ie, greater than 2 units), patients with low starting hemoglobins, and/or Jehovah’s Witness patients who will accept intraoperative salvage. The salvaged blood is generally washed to remove cell debris, fat, and bone fragments. Newer filtration techniques permit the transfusion of blood collected from drains without the washing process.
Bezwada HP, Nazarian DG, Henry DH, Booth RE Jr: Preoperative use of recombinant human erythropoietin before total joint arthroplasty. J Bone Joint Surg Am 2003;85:1795. [PMID: 12954840]
Carless PA, Henry DA, Moxey AJ, et al: Cell salvage for minimizing perioperative allogeneic blood transfusion. Cochrane Database Syst Rev 2010;4:CD001888. [PMID: 20393932]
Gombotz H, Rehak PH, Shander A, Hofmann A: Blood use in elective surgery: the Austrian benchmark study. Transfusion 2007;47:1468. [PMID: 17655591]
Goodnough LT: Autologous blood donation. Crit Care 2004;8 (Suppl 2):S49. [PMID: 15196325]
Keating EM, Ritter MA: Transfusion options in total joint arthroplasty. J Arthroplasty 2002;17:125. [PMID: 12068422]
Strumper D, Weber EW, Gielen-Wijffels S, et al: Clinical efficacy of postoperative autologous transfusion of filtered shed blood in hip and knee arthroplasty. Transfusion 2004;44:1567. [PMID: 15504161]
Zohar E, Ellis M, Ifrach N, et al: The postoperative blood-sparing efficacy of oral versus intravenous tranexamic acid after total knee replacement. Anesth Analg 2004;99:1679. [PMID: 15562053]
ETHICS IN ORTHOPEDIC SURGERY
Ethics in medicine started with Hippocrates and was codified by Thomas Percival in 1803, with the publication of his Code of Medical Ethics. This was extended by the American Medical Association in 1847 and has undergone several revisions over time. Ethics basically define the standards of conduct of honorable or moral behavior by the physician. Many areas of medical ethics, such as abortion or artificial insemination, have little to do with orthopedics. Although many areas of ethics are more restrictive than the law, litigation and legislation have in some cases become the standard by which orthopedists have to abide, with tighter constraints than ethics alone would place. Although ethics as a field is too broad a subject for a text such as this, certain areas that impinge on orthopedics are addressed here.
![]() Clinical Trials
Clinical Trials
A particularly difficult ethical area is the clinical research study. Although many of these are now more than adequately controlled by institutional review boards (IRBs), the federal government’s Office for Human Research Protections, and sponsors of research, the single practitioner in a small orthopedic group is still at risk of performing human, or even animal, research without appropriate ethical controls. The three main areas for concern are the use of ionizing radiation for exams that are not clinically indicated, the use of patient or third-party-payer funds for exams that are not clinically indicated, and the use of patient data in a manner that does not maintain confidentiality. Certainly, ionizing radiation can be used, even for control subjects, if adequate IRB review and patient/subject consent are obtained. This must be done in a formal manner. However, the use of third-party-payer funds for research or revealing patient confidentiality is never ethical. Performing unindicated studies (laboratory, radiographs) at patient expense is certainly unethical. Also, patient confidentiality is fundamental to the doctor–patient relationship. The Health Insurance Portability and Accountability Act (HIPAA) changed the way physicians have to look at confidentiality. Verbal, written, and electronic privacy must be maintained in the office and hospital setting. Patient data have to be closely controlled with care taken regarding personal data assistants, scraps of paper with patient identifiers and data, and roentgenographic images. Photos or slides of football injuries in the public domain may be acceptable for presentation, although in some situations, this may not be true. Certainly, photos or slides of radiographs with patient identifiers for professional presentations or publications cannot be used without written patient permission. The electronic medical record will produce many potential areas that might violate HIPAA regulations, especially with local area networks that permit laptop access in an entire office or building.
The typical orthopedic clinical research study is a retrospective review of a surgeon’s cases. This model of research is considered to be of modest value by researchers doing multicenter, randomized, controlled, double-blind studies, but until the funding is found to do this type of study on something as common as knee replacement, retrospective reviews will have to serve as the database for decision making. This is especially true for low-volume procedures. These types of studies raise several issues. The main issues are paying for the study (not through patient or third-party funds), maintaining patient confidentiality, and conflict of interest. The first two issues can be resolved by IRB oversight, and private practitioners are advised to obtain that help from their hospital. Conflict of interest has at least two aspects. Physicians may be consultants or designers of the prosthesis or drug and have a financial interest in the success of the product, and they have ego invested in their surgery, that is, they do not want to look like “bad” surgeons and hence may be hesitant to report poor results. Furthermore, they may be professors and need to demonstrate clinical research publications as part of promotion requirements or simply want to “advertise” their abilities through publication. The latter aspects are implied conflicts of interest but are probably as important as a financial conflict. The potential financial conflict should be disclosed to the patient and to other parties such as the hospital and to the journal of publication. Surgeons have an ethical obligation to share medical advances, and presenting surgeons’ results with a procedure certainly meets that standard.
![]() Gifts From Industry
Gifts From Industry
The concept that gifts from industry may affect the choice of medication, prosthesis, and so on, is of concern. Generally, the guidelines recommended by the American Medical Association allow gifts, other remuneration, subsidies for meetings, and so on, if the primary purpose is education or of benefit to the patient. Gifts should be of minimal value and related to the physician’s work. The pharmaceutical and orthopedic manufacturers are now self-regulated by industry organizations regarding the type of meetings that they can sponsor. Meetings directly sponsored by the company are only allowed to discuss “label” applications of the drug or device, whereas continuing medical education credit courses, which can only be done through an educational institution, can discuss “off-label” uses of products. Payment for travel costs, lodging, and honoraria to attend such meetings is considered inappropriate unless the physician is performing a service, such as faculty duties or consulting. Although it seems unlikely that a physician would change his or her prescribing practice based on a free meal, the appearance of impropriety is important and should be kept in mind.
Cartwright JC, Hickman SE, Bevan L, Shupert CL: Navigating federalwide assurance requirements when conducting research in community-based care settings. J Am Geriatr Soc 2004;52:1567. [PMID: 15341563]
Council on Ethical and Judicial Affairs: Code of Medical Ethics: Current Opinions with Annotations (2000–2001 edition). Chicago: American Medical Association; 2000.
Epps CH: Ethical guidelines for orthopedists and industry. Clin Orthop 2003;412:14. [PMID: 12838046]
Healy WL Peterson RN: Department of Justice investigation of orthopedic industry. J Bone Joint Surg 2009;91A:1791. [PMID: 19571103]
Laskin RS, Davis JP: The use of a personal digital assistant in orthopaedic surgical practice. Clin Orthop 2004;421:91. [PMID: 15123932]
Oyama L, Tannas HS, Moulton S: Desktop and mobile software development for surgical practice. J Pediatr Surg 2002;37:477. [PMID: 11877671]
Pancoast PE, Patrick TB, Mitchell JA: Physician PDA and the HIPAA privacy rule. J Am Med Inform Assoc 2003;10:611. [PMID: 14631929]