Daniel M. Fein
Jeffrey R. Avner
HIGH-YIELD FACTS
• The risk of serious bacterial illness (SBI) is greatest during the neonatal period, defined as birth to 28 days of life. Some authorities recommend that a child born prematurely should have the degree of immaturity subtracted from the child’s chronological age for this consideration.
• It is generally accepted that a fever is a temperature of ≥38°C or 100.4°F taken with a rectal thermometer.
• A neonate who had a documented fever by any method but is afebrile on admission to the ED should be treated as a febrile neonate whether or not antipyretics have been given.
• The most frequent bacterial pathogens in the neonatal period are group B Streptococcus (GBS), Escherichia coli, and Listeria monocytogenes.
• Hypothermia is a rectal temperature less than 36°C or 96.8°F and, in the neonatal period, may actually be a more common presentation than elevated temperature. All neonates with hypothermia should be treated as septic.
• Causes other than SBI, especially herpes simplex virus (HSV) infection, should be considered and, if suspected, treated expectantly.
• Noninfectious problems, such as congenital heart disease (CHD) and inborn errors of metabolism, may present in a similar way and must always be on the list of potential causes of the septic-appearing infant.
• If the child is exhibiting signs of shock, such as tachycardia, mottling, apnea, or prolonged capillary refill time, aggressive fluid resuscitation must be immediate.
• Antibiotics should be started after cultures have been obtained.
• If the child is unstable, the lumbar puncture may need to be postponed.
Fever is one of the most common presenting complaints of children evaluated in the emergency department (ED). Of particular concern to both parents and practitioners is the febrile neonate (0–28 days), since fever is often the only clinical sign of SBI in this age group. Neonates are at a particularly high risk of SBI due to a relatively immature immune system; including decreased T-helper cell activity, opsonization, antibody titers, macrophage, neutrophil, monocyte, and complement activity compared to older infants.1–3 (Some authorities recommend that a child born prematurely should have the degree of immaturity subtracted from the child’s chronological age for this consideration.) The resultant inability to adequately contain bacterial infections results in higher morbidity for neonates with SBI. In addition, due to developmental immaturity, clinical indicators of wellness are not universally present in the neonate. For example, acquisition of the social smile, one of the most commonly used signs to judge the clinical appearance of infants, generally does not develop until 4 to 8 weeks of age.
Fever is generally defined as a rectal temperature ≥38.0°C (100.4°F). Temperatures obtained by the axillary, otic, temporal artery, or noncontact mid-forehead infrared routes tend to underestimate the rectal temperature and are often unreliable. Neonates with a documented rectal fever obtained by a reliable caretaker at home or in the office setting, who are afebrile on presentation to the ED, have the same risk of SBI as those with documented fever who present initially to the ED. Therefore, they should be managed as febrile whether or not antipyretics have been given. Mild temperature elevation can occur secondary to environmental factors such as bundling; however, in this scenario, the neonate should be unbundled and have repeated temperature measurements to determine whether or not there is fever. Subjective (tactile) fever determination by the parent is unreliable and does not place the neonate at higher risk for SBI. Hypothermia (a≤36.0°C [96.8°F]) can also be a presenting symptom of SBI and the evaluation should be the same as for a febrile neonate.
SBI is typically defined as the presence of a pathogenic bacterial organism in the cerebrospinal fluid (CSF), blood, urine, or stool. Many investigators consider the presence of a lobar infiltrate on chest x-ray to be indicative of bacterial pneumonia and therefore considered a SBI. The rate of SBI in the febrile neonate is >20%.4 Focal bacterial infections such as cellulitis, septic arthritis, omphalitis, and otitis media are typically managed as a SBI if the neonate is febrile.
The epidemiology of SBI has changed over the past several decades due to routine childhood immunization against two of the most previously common pathogens implicated in bacterial meningitis and bacteremia—Haemophilus influenzae type B (HiB) and Streptococcus pneumoniae. The incidence of HiB meningitis has decreased drastically since introduction of the vaccine; although S. pneumoniaeremains one of the most common causes of bacterial meningitis, an overall decrease in the incidence of invasive pneumococcal disease reflects vaccine efficacy. Currently, Escherichia coli and GBS are the most common causes of bacteremia and bacterial meningitis in neonates. E. coliis the pathogen responsible for the majority of neonatal UTIs. Listeria monocytogenes is also a recognized pathogen in younger or premature neonates. Other bacterial pathogens in febrile neonates include Staphylococcus aureus, Salmonella sp., and other gram negative organisms.
While emphasis is typically placed on identification of SBI in febrile neonates, viral infections occur more frequently than bacterial infections. While most viral infections are benign, some may result in serious illness. Neonatal herpes simplex virus (HSV) infection is rare (estimated 1500 cases/year in the United States); however, it carries risk of significant morbidity (primarily neurologic deficits) and mortality that can be reduced with appropriate antiviral therapy. Three different clinical presentations of neonatal HSV that may overlap exist: skin, eye, and mouth infection (45% of cases); central nervous system infection (30% of cases); and disseminated HSV (25% of cases).5Respiratory viruses, such as influenza and respiratory syncytial virus (RSV), are fairly common in febrile neonates, especially in the winter months.
The differential diagnosis of the septic-appearing neonate is broad. Conditions other than sepsis are listed in Table 2-1.
|
TABLE 2-1 |
Noninfectious Etiologies of the Septic-Appearing Neonate |
Congenital Heart Disease (Chapter 39)
Dysrhythmias (Chapter 42)
Inborn Errors of Metabolism (Chapter 79)
Electrolyte Disturbances (Chapter 80)
Congenital Adrenal Hyperplasia (Chapter 77)
Non-accidental Trauma (Chapter 144)
Volvulus (Chapter 45)
Hypoglycemia
Food Protein–Induced Enterocolitis Syndrome (FPIES)
Toxic Exposure
CLINICAL PRESENTATION
Ill-appearing febrile neonates require rapid assessment of the airway, breathing, and circulation along with intravenous access, fluid resuscitation, oxygen administration, and parenteral antibiotics. If the neonate appears well, the evaluation can begin with a complete history and physical exam. Practitioners should inquire about any changes to the neonate’s activity level and feeding habits as part of the global assessment and to evaluate for concurrent dehydration. Associated signs and symptoms are important as these may alter the ensuing evaluation—specifically, the presence of upper respiratory symptoms (rhinorrhea, cough, tachypnea, grunting, or wheezing), vomiting, or diarrhea. A thorough birth history should be obtained including gestational age, method of delivery, mother’s GBS status, history of maternal HSV, history of perinatal antibiotics, or any previous hospitalizations including a prolonged postpartum hospitalization or any time spent in the neonatal intensive care unit. The impact of an acute febrile illness on any known chronic illnesses, such as congenital heart disease or congenital adrenal hyperplasia should be considered. A family history of neonatal deaths is important as this may point to an inborn error of metabolism as the underlying etiology. Finally, a social history should be obtained; the practitioner must feel confident in the parent’s ability to observe the neonate at home and plan appropriate follow-up to consider discharge from the ED.
Practitioners tend to develop a sense of gestalt of the neonate by observing its overall general appearance and response to stimuli. The presence of abnormal vital signs necessitates immediate intervention. Care should be taken to assess the hydration status of the neonate; evaluation for the presence of sunken eyes, a depressed fontanelle, decreased skin turgor, or delayed capillary refill are signs of dehydration. Seizures or the presence of a tense, bulging fontanelle may be signs of meningitis. Tympanic membranes should be evaluated for erythema or bulging and the oropharynx for lesions. Apnea; tachypnea; signs of labored breathing such as retractions, flaring, or grunting; and findings on lung auscultation are important to help guide the evaluation and management of the neonate. A murmur or hepatomegaly can be a sign of congestive heart failure. Skin should be thoroughly examined for rashes—vesicles (seen in HSV), petechiae (seen in sepsis and disseminated intravascular coagulation), or an area of cellulitis. The umbilical stump should be examined to assess for the presence of cellulitis of the periumbilical area and anterior abdominal wall (omphalitis). Extremities should be assessed for any point tenderness or signs of joint infection. Pale or mottled skin, poor peripheral perfusion, and acrocyanosis are also potential signs of sepsis in the febrile neonate.
LABORATORY EVALUATION
Because of the high rate of SBI, the increased morbidity from these infections, and unreliability of the clinical evaluation, it is crucial for febrile neonates to be evaluated for bacterial infections. A “sepsis” evaluation for SBI consists of obtaining bacterial cultures of the blood, urine, and CSF as well as a stool culture (in the presence of diarrhea) and a chest x-ray (if there are respiratory findings). Other standard tests include a complete blood count, urinalysis, and clinical chemistry panel (Table 2-2).
|
TABLE 2-2 |
Potential Evaluation of the Febrile Neonate |
Complete blood count (CBC)
Blood culture
Urinalysis and culture (regardless of U/A results)—catheterized specimen
Lumbar puncture with cell count and differential, culture, protein, glucose
CSF-PCR for herpes and enterovirus
Chest radiograph (when indicated)
Complete metabolic panel (electrolytes, glucose, liver function tests)
Stool culture and leukocyte count (with diarrhea)
C-reactive protein
Procalcitonin
Urine is commonly sent for a dipstick analysis to evaluate for the presence of leukocytes or nitrites; however, a microscopic urinalysis must be obtained to evaluate the gram stain and number of WBCs as the dipstick analysis is not reliable in this age group. An enhanced urinalysis, using a hemocytometer cell count and gram stain on uncentrifuged urine, has a higher sensitivity and negative predictive value for presence of a UTI.6 It is important that the urine be obtained by urethral catheterization or suprapubic aspiration as bagged urine samples have increased risk of contamination and a false-positive result. CSF can be examined for WBCs and also be sent for enterovirus and/or HSV PCR if indicated. A stool smear for WBCs and stool culture should be obtained if there is diarrhea. Rapid antigen testing for RSV and influenza can be obtained in the presence of rhinorrhea or respiratory symptoms, especially during winter months when these viruses are at their peak prevalence. A chest x-ray should only be obtained in a febrile neonate with respiratory symptoms as it has not been shown to have diagnostic utility in the absence of respiratory symptoms.
As most mothers of HSV-positive neonates do not report a history of HSV infection, and most cases of neonatal HSV will present without any skin findings, the practitioner must often use clinical clues to determine if a febrile neonate is at risk for HSV infection. A HSV PCR is indicated if there are any vesicular skin lesions; a history of maternal HSV infection; or if the neonate is lethargic, irritable, or ill-appearing. In addition, laboratory evaluation for HSV is warranted if there is hypothermia, seizures, respiratory distress, elevated liver transaminases (a sign of disseminated HSV), or CSF pleocytosis. Some advocate testing of all neonates <21 days old for HSV, irrespective of other clinical findings.
There has been a recent focus on the use of serum biomarkers such as C-reactive protein (CRP) and procalcitonin to aid in the diagnosis of SBI in febrile neonates. Procalcitonin has been found to have a higher sensitivity and negative predictive value than CRP when evaluating febrile neonates for SBI; however, only one study limited the evaluation to infants <2 months of age.7 Although procalcitonin and other biomarkers may play a role in screening for SBI in the future, they are currently not used for risk stratification of febrile neonates.
MANAGEMENT
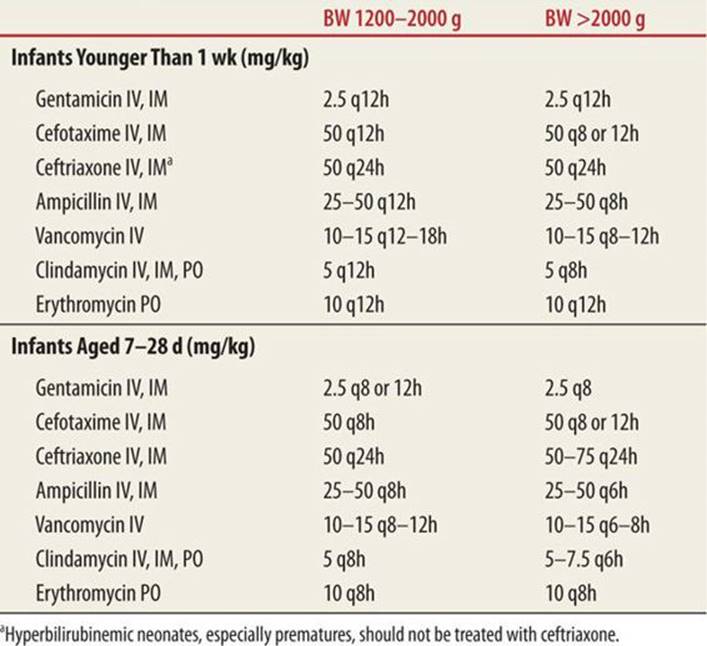
Management of the ill-appearing or febrile neonate begins with ensuring hemodynamic stability. This includes assessment and stabilization of the airway, breathing, and circulation. Endotracheal intubation may be necessary to maintain adequate oxygenation and ventilation. Appropriate fluid management to compensate for any deficits is crucial, and vasopressors may be required to maintain circulation in a critically ill patient. Since glucose is the major energy source for neonates and alternate energy sources (ketones, lactate) are limited, any metabolic stress predisposes the neonate for developing hypoglycemia. Therefore, a bedside blood glucose level should be measured and glucose supplemented if low. Inasmuch as ill-appearing neonates are at high risk for SBI, empiric antibiotic treatment should be administered as part of the initial management, deferring the lumbar puncture, if necessary, until the patient is hemodynamically stable. Although there remains considerable practice variation with respect to empiric antibiotics for the febrile or ill-appearing neonate, we recommend ampicillin and a third-generation cephalosporin, such as cefotaxime, as first-line therapy for the empiric treatment of the febrile neonate. The recommended doses for these and other antibiotics are given in Table 2-38
|
TABLE 2-3 |
Antibiotic Therapy for the Febrile or Septic-Appearing Neonate |
A variety of management strategies exist for neonates who are at high risk for HSV infection, including empiric treatment with acyclovir for all neonates <21 days of age9 or those with CSF pleocytosis.10Empiric acyclovir should be considered for ill-appearing neonates; premature neonates; neonates with vesicular skin lesions, seizures, increased liver transaminases, or maternal history of HSV in the third trimester. Early initiation of acyclovir is the goal of therapy as a delay of even 1 day after hospitalization is associated with increased mortality. Nevertheless, a recent survey suggests that despite these management recommendations and knowledge of neonatal HSV risk factors, many practitioners do not often administer empiric acyclovir.11
REFERENCES
1. Zola H. The development of antibody responses in the infant. Immunol Cell Biol. 1997;75(6):587–590.
2. Maisey HC, Doran KS, Nizet V. Recent advances in understanding the molecular basis of group B Streptococcus virulence. Expert Rev Mol Med. 2008;10:e27.
3. Doran KS, Nizet V. Molecular pathogenesis of neonatal group B streptococcal infection: no longer in its infancy. Mol Microbiol. 2004;54(1):23–31.
4. Schwartz S, Raveh D, Toker O, et al. A week-by-week analysis of the low-risk criteria for serious bacterial infection in febrile neonates. Arch Dis Child. 2009;94(4):287–292.
5. White JC, Magee SR. Neonatal herpes infection: case report and discussion. J Am Board Fam Med. 2011;24(6):758–762.
6. Herr SM, Wald ER, Pitetti RD, Choi SS. Enhanced urinalysis improves identification of febrile infants ages 60 days and younger at low risk for serious bacterial illness. Pediatrics. 2001;108(4):866–871.
7. Woelker JU, Sinha M, Christopher NC, Powell KR. Serum procalcitonin concentration in the evaluation of febrile infants 2 to 60 days of age. Pediatr Emerg Care. 2012;28(5):410–415.
8. American Academy of Pediatrics. Tables of antibacterial drug dosages. In: Pickering LK, Baker GJ, Long SS, et al., eds. Red Book: 2006 Report of the Committee on Infectious Disease. 27th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2006:751–752.
9. Long SS, Pool TE, Vodzak J, Daskalaki I, Gould JM. Herpes simplex virus infection in young infants during 2 decades of empiric acyclovir therapy. Pediatr Infect Dis J. 2011;30(7):556–561.
10. Caviness AC, Demmler GJ, Swint JM, Cantor SB. Cost-effectiveness analysis of herpes simplex virus testing and treatment strategies in febrile neonates. Arch Pediatr Adolesc Med. 2008;162(7):665–674.
11. Benidir A, Lim R, Salvadori M, Sangha G, Poonai N. Current practice patterns regarding diagnostic investigations and empiric use of acyclovir by Canadian pediatric emergency physicians in febrile neonates. Pediatr Emerg Care. 2013;29(3):273–278.