Andrea T. Cruz
HIGH-YIELD FACTS
• The most common cause of fever in the child returned from international travel is the nonspecific viral illness.
• It is imperative to consider treatable causes of fever (e.g., malaria) or fever etiologies at risk for decompensation and the need for supportive care (e.g., dengue).
• Diagnostic evaluation and differential diagnosis should be driven by the history of pre-travel immunizations and receipt of prophylactic medication, region of travel, activities undertaken while abroad, return date, physical examination findings (including severity and duration), and knowledge of the most common pathogens seen in a given area.
• A population at considerable risk for travel infections is termed visiting friends and relatives (VRFs), as these families often opt not to seek medical attention prior to travel.
• Thick and thin smears for malaria are indicated for any febrile child returning from a malaria-endemic region. Negative smears to not exclude malaria, and if strong clinical suspicion exists, smears should be repeated every 6 to 12 hours.
• Malaria treatment often is empiric, and chloroquine resistance should be assumed. Therapy for children with high-grade parasitemia may involve blood transfusion (or exchange transfusion) and treatment with a combination of parenteral agents. These may include clindamycin in addition to quinidine or quinine.
• Typhoid fever is very common in travelers (especially from the Indian subcontinent and Asia). Diarrhea is not always seen. Bacteremia may be common. Increasing antibiotic resistance in Salmonella typhiisolates makes microbiologic confirmation important.
• Dengue is extending its geographical distribution and is now seen in southern portions of the United States. It is a biphasic illness, with an initial nonspecific febrile illness with or without a viral exanthema. After a few days, hemorrhagic manifestations and symptoms corresponding to capillary leak are manifest, lasting 2 to 3 days. Treatment is supportive.
• Evaluation of the child with diarrheal disease after return from international travel warrants stool culture. Although antimicrobial therapy (often, macrolide-based) can reduce symptom duration, disease severity, and secondary spread within the household, the mainstay of therapy is fluid resuscitation.
The emergency department (ED) is a common venue of care for children who are ill after a recent international travel. At least three categories of pediatric travelers can be identified: children returning home after travel; international adoptees; and recently arrived immigrants. Barriers to access to care, severity of illness, timing of symptom onset (weekends, holidays), and community referral patterns may result in children in all the above mentioned groups presenting to the ED.
Individuals VFRs often neglect to seek travel advice prior to trips under the preconception that children have residual immunity when returning to the family’s country of origin. Waning immunity, failure to develop effective long-term immune responses to certain infections (e.g., malaria), and lack of preventive strategies result in many of these children becoming ill. In the Houston area, for example, the single greatest risk factor for childhood malaria is being a VFR traveling to Nigeria; few of these children had received adequate malarial prophylaxis.1
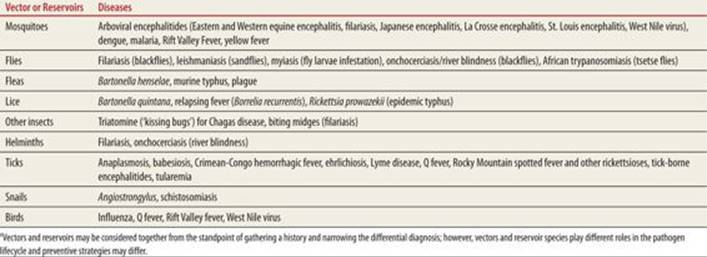
It is also important for the ED provider to recognize the regional flavor for what is considered “local” (Table 66-1)2 Endemic diseases in one part of the United States may represent a travel infection in another. Families may neglect to mention trips to a given area if they are taken frequently or do not require much travel time (e.g., hunting trips) but the definition of travel from an infectious disease’s standpoint is not contingent upon distance. It is any activity that places a person in contact with a set of microbial flora to which the person is not exposed in his/her everyday life. A list of non-mammalian vectors for different diseases is listed in Table 66-2.3
|
TABLE 66-1 |
Geographic Distribution of Selected Infectious Diseasesa |

|
TABLE 66-2 |
Non-mammalian Vectors or Reservoirs for Selected Infectious Diseasesa |
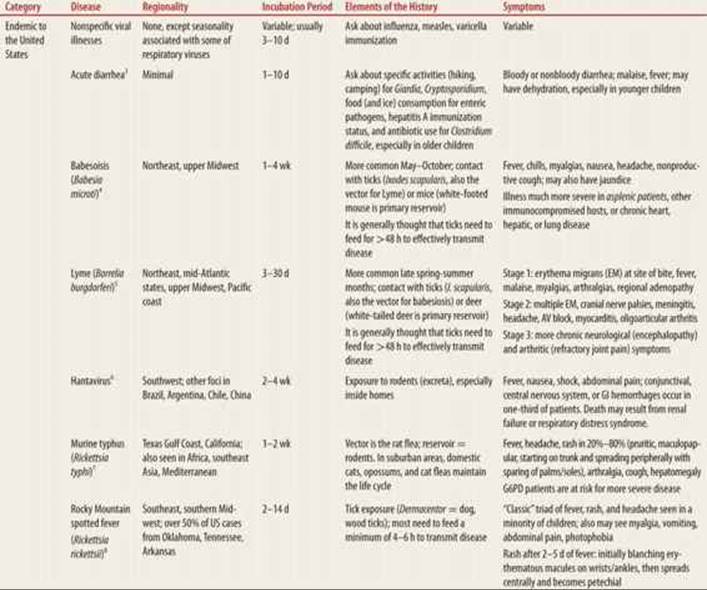
One way to conceptualize fever in the traveler is to subdivide diseases into three categories (Table 66-3).4–25 The first category represents diseases endemic to the United States, and thus the travel history represents a red herring. The most common cause of fever in returned travelers is a nonspecific viral illness or gastroenteritis.26 A sub-category is the vaccine-preventable illness,27 such as hepatitis A, influenza, or measles. The latter specifically is very readily transmitted, and given the low vaccination rates in many portions of the United States28 may rapidly spread in a susceptible population. VFRs are more likely to have a vaccine-preventable disease than other groups.29Another sub-category is disease seen in other parts of the country (e.g., babesiosis, Lyme). A final subcateory is sexually transmitted infections (STIs) acquired internationally (e.g., acute HIV infection), and should be on the differential diagnosis of the adolescent returning from abroad (see Chapter 88, Sexually Transmitted Infections).
|
TABLE 66-3 |
Travel Diseases |
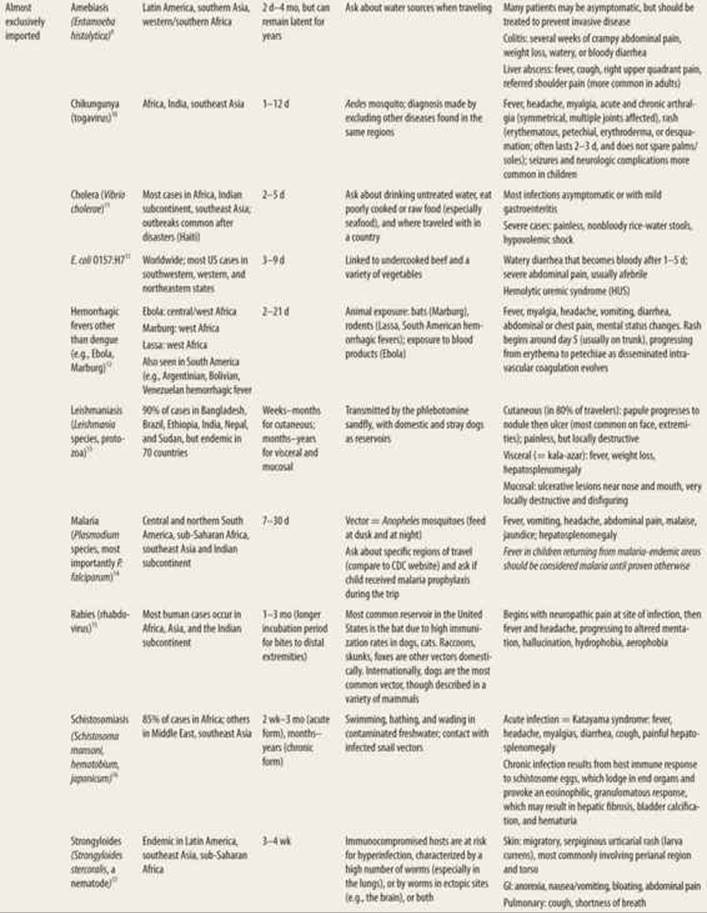
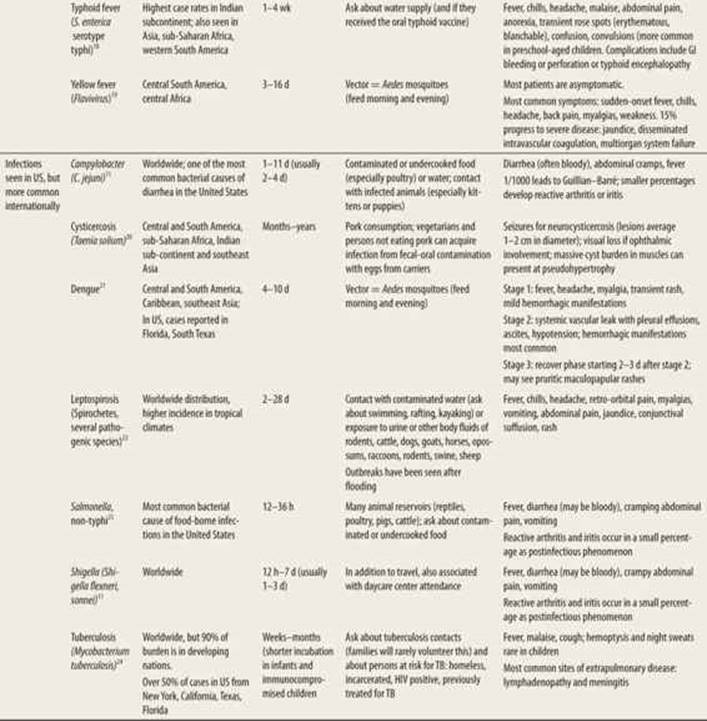
The second category reflects illnesses that are not endemic to the United States and are almost exclusively imported (e.g., malaria, yellow fever, most cases of typhoid, some causes of dysentery). The history both of travel and of activities performed and location within a given country are essential to identifying the cause of fever. The spectrum of symptoms may overlap with common domestic diseases (e.g., gastroenteritis) or the child may present with fever without localizing signs.
The third category is for illnesses seen both domestically and internationally (e.g., tuberculosis (TB), non-typhi Salmonella, and some diseases that are now emerging in the United States, such as dengue).30Depending upon the region where the child resides, these diseases may be more or less common there. Finally, there are infectious diseases whose incubation period is quite long, and children are unlikely to present to the ED with symptoms referable to a recent trip (e.g., TB in older children and adolescents).
HISTORY AND PHYSICAL EXAMINATION
Historical elements that should be queried: use of prophylactic medications; receipt of vaccines prior to travel; activities, areas and duration of travel, and timing of return.
It is insufficient to simply ask if a medication was given prior to departure; specific questions regarding adherence should be asked. For example, a child may have been prescribed chloroquine and subsequently traveled to an area where all Plasmodium species are chloroquine-resistant. Some antimalarial prophylaxis medications are administered daily, whereas others are given weekly leading to a lower likelihood that a family will remember to administer the weekly medication. Finally, most antimalarials are intended to be started before arrival and continued after departure for maximum efficacy.
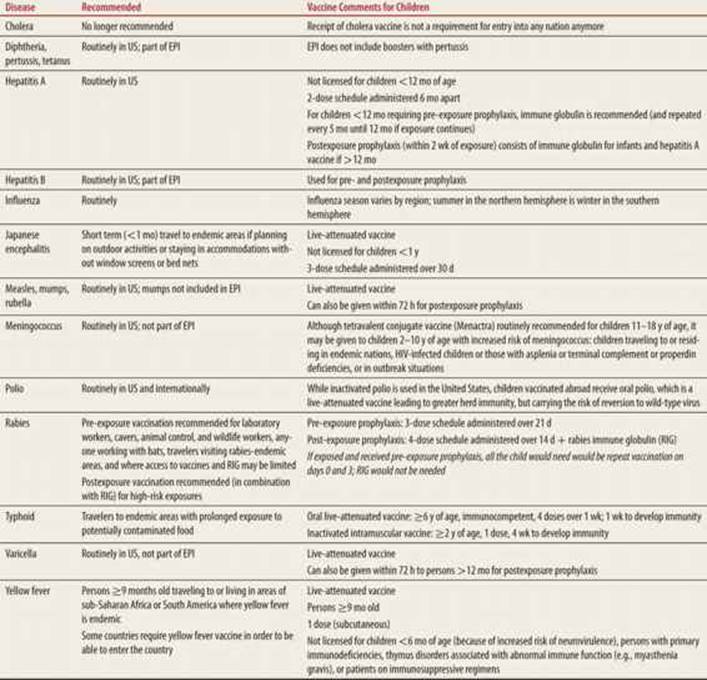
A history of immunizations obtained prior to travel is also important (Table 66-4).31 A number of vaccine-preventable diseases are not on the World Health Organization’s Expanded Programme on Immunizations32 due to cost issues. Vaccine-preventable diseases may be more common in some countries versus others owing to political or infrastructure access limitations. The child whose family opts to defer immunization may well become ill internationally, where the herd immunization effect may not be present. For typhoid immunization, it is worth asking if the child received the more effective oral live-attenuated vaccine or the intramuscular injection. Finally, from the standpoint of influenza, it is important to realize that the viral seasonality diminishes the closer one gets to the equator,33 and that travel to sub-Saharan African during summer vacation in the United States means that the child is entering winter viral respiratory season during travel.
|
TABLE 66-4 |
Vaccine-preventable Illnesses More Common Internationally |
It also is important to inquire about regions with countries visited. Rural areas may have less reliable water supplies than urban regions, and visitors staying with families may also have less access to potable water than persons staying in hotels. Persons traveling at high altitudes may be at less risk of malaria, as most Anopheles species are less common at high elevation.34 Activities undertaken on the trip may help evaluate risk for exposure to specific vectors. Many enteric pathogens are water-borne and more common in kayakers and rafters.
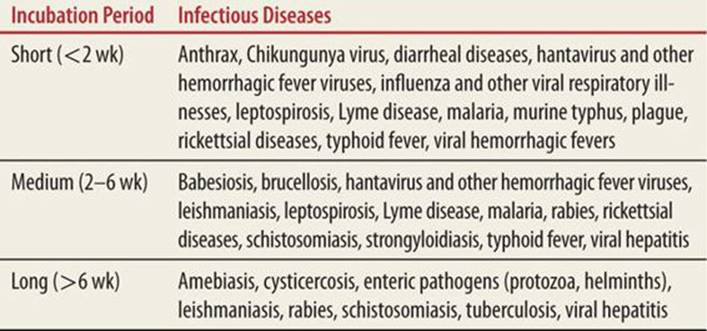
Trip duration and date of return may help quantify the risk of certain diseases based on its incubation period (Table 66-5)3 Of note, the use of prophylaxis for travelers is bimodal when compared to trip duration. Many travelers who will only be in-country for a few days may opt not to take prophylaxis. Travelers who will be in country for weeks to months may take antimalarial prophylaxis, but trips of longer duration may result in families defaulting on or never initiating preventive therapy.
|
TABLE 66-5 |
Incubation Periods for Selected Infectious Diseases |
The most common examination findings for selected diseases are listed in Table 66-3. The presence of lymphadenopathy, hepatosplenomegaly, rash, and neurological or musculoskeletal complaints may enable clinicians to narrow the differential diagnosis as can clinical manifestations of locally endemic diseases.
LABORATORY EVALUATION
There is no standard approach to laboratory evaluation in a febrile child returning from abroad. In part, the evaluation is contingent upon clinical appearance, duration of fever, and primary symptoms. Table 66-3 provides lists of diagnostic tests for identifying specific disease entities.
Of note, eosinophilia (>500 cells/mm3) in infectious diseases is seen when parasites have a phase with tissue migration; pathogens that stay within the gut lumen, for example, do not have associated eosinophilia. The presence of eosinophilia may be the first suggestion of roundworm (Ascaris, Strongyloides, Toxocara), tapeworm, filariasis, schistosomiasis, Echinococcus, or lung/liver flukes. Other parasitic diseases are described in Chapter 65.
SPECIFIC DISEASES
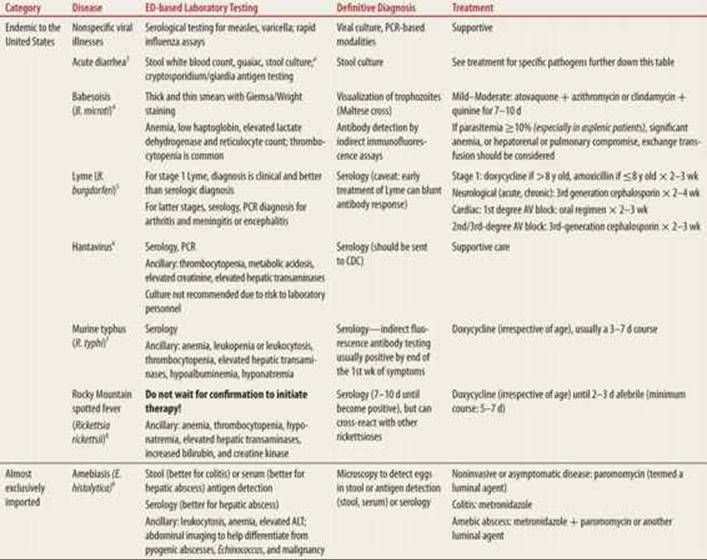
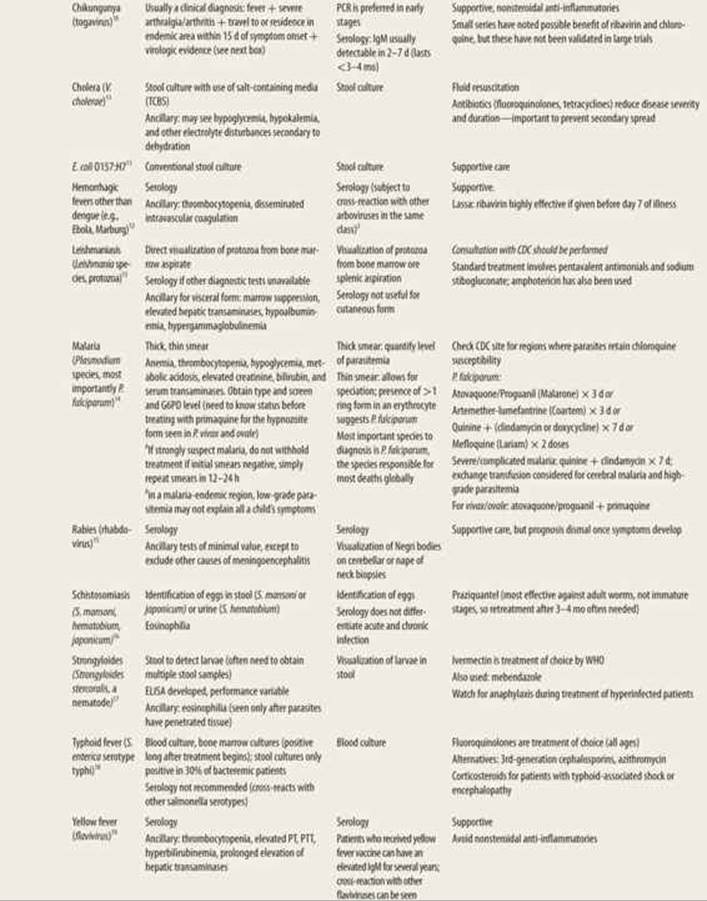
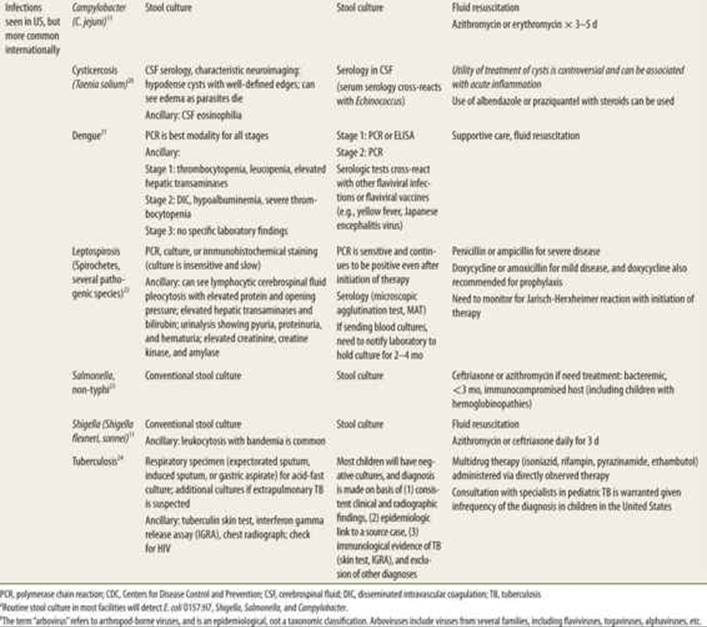
The incubation periods and most common symptoms of diseases in the returning traveler are listed in Table 66-3, whereas diagnostic and therapeutic approaches are discussed in Table 66-6. Malaria, dengue, and typhoid are specifically described below; all of which are diseases reportable to health departments.28
|
TABLE 66-6 |
Diagnostic Testing and Treatment of Travel-Associated Infections |
![]() MALARIA
MALARIA
Plasmodium falciparum should be very high on the differential diagnosis of the febrile child returning from a malarial-endemic region. The urgency of establishing this diagnosis is because the disease is treatable and the highest morbidity and mortality occur in young children.35 In malarial endemic areas, fever is considered malaria until proven otherwise. However, low-level parasitemia should not preclude evaluation for other infectious etiologies. Malarial regions often have substantial overlap with typhoid or other treatable infectious agents (Table 66-1). Malarial symptoms in a child who has not traveled internationally may represent babesiosis (Tables 66-3 and 66-6).
Evaluation for malaria is based upon thick and thin smears using Giemsa and Wright stains. Ancillary laboratory evaluation should include a complete blood count to evaluate for anemia, thrombocytopenia and other findings seen with malaria, glucose and electrolytes, and blood should be held for type and cross and glucose-6-phosphate dehydrogenase (G6PD) deficiency. Thick smears enable the laboratory to estimate the degree of parasitemia (percentage of parasite-infected erythrocytes per 100 erythrocytes counted) but cannot estimate disease severity solely. Knowledge of disease burden can provide preliminary estimate of risk of complication and potential interventions needed. Parasitemia levels above 2% are most common with P. falciparum and less frequently noted with other species. Levels of 2% to 5% are associated with increased mortality, and levels above 10% can be associated with ischemic damage and warrant consideration for exchange transfusions (at or above this level).
The thin smear enables one to differentiate among malarial species, as more than one species may be endemic in certain areas (e.g., West Africa). P. falciparum, the most common species causing death in children, is characterized by signet ring forms in the erythrocytes, and is the only malarial species with high enough levels of parasitemia that more than one ring form may be visualized in a single erythrocyte. Other smear findings with P. falciparum may be a banana-shaped gametocyte form. Negative smears should not preclude initiation of empiric malarial therapy if the clinical suspicion for malaria is high. Children may have transient parasitemia, so if the initial smears are negative, they should be repeated every 6 to 12 hours (collecting specimens up to 72 hours is not uncommon). The optimal time to collect blood for smears is midway between episodes of chills. Once treatment is initiated, smears should be repeated to monitor response to therapy. Rapid diagnostic assays have been developed to detect plasmodial proteins; these generally enable differentiation of P. falciparum from other forms, but do not enable differentiation between the other 3 species. Polymerase chain reaction (PCR) is more sensitive (and user-independent) than smear, but is not available in all settings.
Parasitemia of any degree in a febrile child returning from abroad should be treated. Treatment of mild–moderate malaria occurs in the outpatient setting in many regions, but inpatient treatment should be considered in industrialized nations because of the risk of continued hemolysis and electrolyte disturbances. Disease severity is worse in young children and in children with baseline anemia (including hemoglobinopathies). The heterozygous state for sickle cell is protective against developing malarial symptoms; the homozygous state for sickle cell is associated with increased mortality due to high-output cardiac failure and electrolyte disturbances due to hemolysis. In regions where Plasmodium vivax (northern South America, southern Central America, sub-Saharan Africa, Indian subcontinent and southeast Asia) and Plasmodium ovale (West Africa, southeast Asia, Pacific islands) are endemic, children will require primaquine to eliminate the latent (hypnozoite) form. Primaquine will cause massive hemolysis in children with G6PD deficiency, so this laboratory should be sent in any child in whom malaria is being considered, as there is considerable overlap in the distribution of Plasmodium species. Any child receiving quinidine (quinine being less readily available in the United States) should receive electrocardiogram (EKG) monitoring, as quinidine may prolong the QT interval.15 Children with a high degree of parasitemia, severe anemia, altered mentation, respiratory distress, or evidence of renal failure should be considered for admission to the pediatric intensive care unit for close monitoring and in the event they require exchange transfusion.
![]() DENGUE
DENGUE
Dengue should be considered in the differential diagnosis of any patient presenting within 2 weeks of return from tropical or subtropical areas, even if the region is not traditionally described as being dengue-endemic (since its distribution is widening). The diagnosis of dengue is of importance for epidemiological reasons (expansion of disease into the southern United States) and for monitoring for potential complications, not because of specific treatment options available. The fever, rash, and myalgias/arthralgias of dengue can be confused with other viral syndromes or rickettsial disease. There are four dengue serotypes, and sequential infection by two different serotypes is associated with more severe diseases, including hemorrhagic complications.22
After an incubation period of 3 to 7 days, three distinct clinical phases can be identified. Phase 1 is termed the febrile phase. During this stage, children have pyrexia (or hyperpyrexia), vomiting, joint pain, and may have a transient maculopapular rash. Hemorrhagic findings are uncommon, and laboratory findings may indicate mild thrombocytopenia or leukopenia, sometimes with elevation of hepatic transaminases. This phase often lasts 3 to 7 days, and most patients do not progress to the next phase.22 The differential diagnosis for a child presenting in phase 1 may include cytomegalovirus and Epstein–Barr virus. Phase 2, which is more common in children and adolescents than in older adults, is characterized by capillary leak. There may be clinical and radiographic evidence of serositis, with ascites and pleural effusions due to hypoalbuminemia and disseminated intravascular coagulation, evidenced by mucosal bleeding or development of petechiae. Children may remain normotensive initially, but narrowed pulse pressure is common before children develop uncompensated shock. Once hypotension develops, it may be refractory to fluid resuscitation. Prognostic factors for shock include worsening abdominal pain, persistent emesis, tender hepatomegaly, evidence of hemoconcentration, mucosal bleeding, and altered mentation.22 Transfusion-refractory thrombocytopenia (often, <20,000/mm3) is common and resolves spontaneously during stage 3. Phase 3 begins 2 to 3 days after the onset of phase 2. It is characterized by rapid clinical and laboratory improvement. Changing rash morphology may be seen, with a pruritic vasculitic rash that may desquamate during resolution (over 1–2 weeks).
Laboratory evaluation should include a complete blood count, electrolytes, and blood urea nitrogen (BUN) and creatinine (to evaluate for renal failure), type and screen, hepatic transaminases, prothrombin time, partial thromboplastin time, fibrinogen, D-dimer, and fibrin split products. Management of phase 2 patients is complicated by the high risk of fluid overload in these patients with vascular leak.36 Blood transfusion may be needed for patients who are severely anemic. There are no convincing data regarding the utility of platelet transfusions for dengue patients. The consumptive coagulopathy seen in dengue appears to be refractory to transfusions. There are no specific antivirals that are of use in dengue.
![]() TYPHOID
TYPHOID
Salmonella enterica serotype typhi (typhoid fever) may cause local (diarrheal) or invasive disease (bowel perforation, bacteremia, meningitis, osteomyelitis). The decision to treat persons with local disease is contingent upon their risk of invasive disease. The American Academy of Pediatrics recommends treating Salmonella gastroenteritis in infants younger than 3 months, immunocompromised hosts of any age (e.g., patients with hemoglobinopathies), chronic gastrointestinal (GI) tract disease, and persons with signs of systemic disease.37 Typhoid fever is spread from fecal-oral transmission from Salmonella carriers or persons with symptomatic disease, and is much more common internationally, with particularly high prevalence on the Indian subcontinent. In contrast, non-typhi salmonellosis is more commonly acquired from contaminated poultry or other nonhuman animals, and is quite common domestically.19
Preschool-aged children may have a nonspecific febrile illness without GI manifestations. In older children and adults, an influenza-like illness with generalized abdominal pain may follow. Tender hepatosplenomegaly may be found on examination. Relative bradycardia is neither a frequent nor a pathognomonic finding, and rose spots (blanchable erythematous subcentimeter maculopapular lesions) are transient and found in a minority of patients. Complications of typhoid include shock, meningitis, pneumonia (primary Salmonella pneumonia or secondary bacterial infection), and GI perforation or hemorrhage.
Management includes fluid resuscitation, and prompt administration of antibiotics to children with evidence of invasive disease or at risk for dissemination of localized gastroenteritis (Table 66-3). Empiric antibiotic therapy has been complicated in recent years by increasing antibiotic resistance, driven in part by the ready availability of antibiotics without prescriptions in developing nations. Multidrug-resistant strains have been described in the Middle East, Africa, and Asia. Randomized trials have shown that the use of fluoroquinolones results in decreased time to defervescence, lower relapse rates, and lower rates of stool carriage when compared with other commonly used antibiotics such as trimethoprim-sulfamethoxazole. Many experts recommend first-line use of fluoroquinolones in patients of all ages.19 Use of third-generation cephalosporins and macrolides are options for children, as fluoroquinolones are not approved for this indication in children younger than 18 years.37 Adjunctive corticosteroid use has been shown to decrease morbidity and mortality for patients with central nervous system manifestations and those with fluid-refractory shock.
DIARRHEAL DISEASES
After the nonspecific febrile illness, the second most common reason returning travelers seek medical attention is for diarrheal disease. The risk of a traveler having a bacterial etiology is much higher than a child without a travel history who presents to the ED. Bacterial stool studies should be strongly considered in the traveler or any child with dysentery (lower GI tract inflammation characterized by the presence of blood and/or mucus).
Elements of the history of present illness should include if the diarrhea is painless (e.g., cholera) or painful (e.g., Campylobacter), presence of systemic symptoms such as fever, and fecal characteristics (e.g., foamy, bloody, presence of mucus). Examination findings should evaluate for level of dehydration, presence of extra-intestinal disease or systemic toxicity, abdominal tenderness, presence of hepatosplenomegaly, and signs of renal failure, anemia, or volume overload for patients with hemolytic uremic syndrome (HUS). Stool studies to consider would include fecal white blood cells, guaiac, stool culture, and Cryptosporidium/Giardia antigen testing. Knowledge of institutional protocols regarding stool processing is important as evaluation for other parasites may require a discussion with the microbiology laboratory. At many institutions, the default for ordering ova and parasites is to perform antigen testing for Cryptosporidium and Giardia (the most common organisms encountered domestically). Ancillary laboratory evaluation may include a complete blood count, blood culture, BUN and creatinine, and a peripheral smear if HUS is suspected.
Management includes fluid resuscitation and, for children with severe dehydration, evaluation for electrolyte disturbances and/or hypoglycemia. Antibiotics are indicated for certain species (Shigella, Campylobacter, non-typhi Salmonella in certain scenarios), cholera, enterotoxigenic and enteroinvasive Escherichia coli) to decrease symptom duration, decrease fecal shedding (and thereby decrease secondary spread within the household), and decrease morbidity/mortality. It is equally important to be cognizant of situations where antibiotic therapy is detrimental (e.g., Shiga-toxin producing E. coli, where there are data indicating that the use of antibiotics increases HUS risk12). Empiric use of a macrolide will offer coverage for most bacterial etiologies, and if empiric therapy is to be utilized, azithromycin is now the first-line antibiotic, given resistance to cephalosporins and penicillins. Although this strategy is commonly utilized in travel medicine clinics to provide anticipatory guidance to families prior to travel, the risks and benefits of empiric treatment of dysentery should be evaluated on a case-by-case basis. The following diarrheal diseases must be reported to health departments: cholera, giardiasis, non-typhi salmonellosis, shiga toxin-producing E. coli, and shigellosis.28
CONCLUSIONS
Evaluation of fever in the returning traveler can be challenging. Asking not only about travel, but specifics (locations within countries, activities) of travel, as well as travel dates, can narrow the differential diagnosis. Diagnostic evaluation should be driven by specific risk factors, physical examination findings (including toxicity), and duration of illness. Treatable etiologies, such as malaria, and etiologies with higher morbidity and mortality should be considered first. A number of online resources (Figure 66-1) can be utilized to expand differential diagnoses, guide the diagnostic evaluation, and risk stratify children who have returned from different areas.
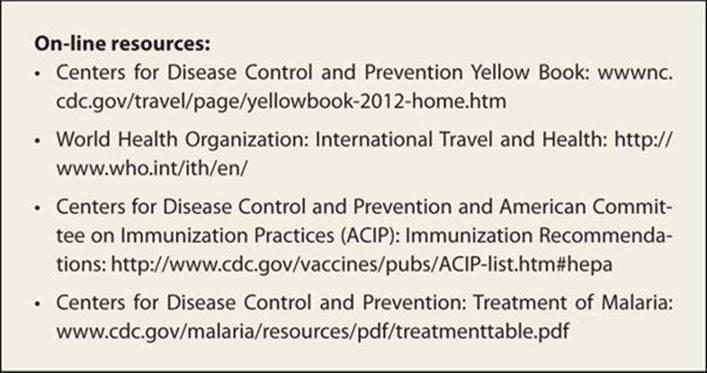
FIGURE 66-1. On-line resources for healthcare workers caring for travelers.
REFERENCES
1. Oramasionwu GE, Wootton SH, Edwards MS. Epidemiologic features impacting the presentation of malaria in children in Houston. Pediatr Infect Dis J. 2010;29:28–32.
2. Brunette GW, ed. Centers for Disease Control and Prevention. The Yellow Book: CDC Health Information for International Travel. Oxford University Press; 2012.
3. Pickering LK, ed. American Academy of Pediatrics. Red Book: 2012 Report of the Committee on Infectious Diseases. 29th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2012.
4. Thielman NM, Guerrant RL. Acute infectious diarrhea. N Engl J Med. 2004;350:38–47.
5. Vannier E, Krause PJ. Human babesiosis. N Engl J Med. 2012;366: 2397–2407.
6. Steere AC. Lyme disease. N Engl J Med. 2001;345:115–125.
7. Jonsson CB, Figueiredo LT, Vapalahti O. A global perspective on hantavirus ecology, epidemiology, and disease. Clin Microbiol Rev. 2010;23:412–441.
8. Civen R, Ngo V. Murine typhus: an unrecognized suburban vector-borne disease. Clin Infect Dis. 2008;46:913–918.
9. Dantas-Torres F. Rocky Mountain spotted fever. Lancet Infect Dis. 2007;7:724–732.
10. Haque R, Huston CD, Hughes M, et al. Amebiasis. N Engl J Med. 2003;348:1565–1573.
11. Burt FJ, Rolph MS, Rulli NE, et al. Chikungunya: a re-emerging virus. Lancet. 2012;379:662–671.
12. DuPont HL. Bacterial diarrhea. N Engl J Med. 2009;361:1560–1569.
13. Meltzer E. Arboviruses and viral hemorrhagic fevers. Infect Dis Clin N America. 2012;26:479–496.
14. Pavli A, Maltezou HC. Leishmaniasis, an emerging infection in travelers. Int J Infect Dis. 2010;14: e1032–e1039.
15. Centers for Disease Control and Prevention. Guidelines for the treatment of malaria in the United States. www.cdc.gov/malaria/resources/pdf/treatmenttable.pdf. Accessed August 5, 2012.
16. Yousaf MZ, Qasim M, Zia S, et al. Rabies molecular virology, diagnosis, prevention, and treatment. Virol J. 2012;9:50.
17. Ross AG, Bartley PB, Sleigh AC, et al. Schistosomiasis. N Engl J Med. 2002;346:1212–1220.
18. Siddiqui AA, Berk SL. Diagnosis of Strongyloides stercoralis infection. Clin Infect Dis. 2001;33:1040–1047.
19. Parry CM, Hien TT, Dougan G, et al. Typhoid fever. N Engl J Med. 2002;347:1770–1782.
20. Jentes ES, Poumerol G, Gershman MD, et al. The revised global yellow fever risk map and recommendations for vaccination, 2010: consensus of the informal WHO Working group on Geographic Risk for Yellow Fever. Lancet Infect Dis. 2011;11:622–632.
21. Garcia HH, Gonzalez AE, Evans CAW, et al. Taenia solium cysticercosis. Lancet. 2003;362:547–556.
22. Simmons CP, Farrar JJ, van Vinh Chau N, et al. Dengue. New Engl J Med. 2012;366:1423–1432.
23. Bharti AR, Nally JE, Ricaldi JN, et al. Leptospirosis: a zoonotic disease of global importance. Lancet Infect Dis. 2003;3:757–771.
24. Feasey NA, Dougan G, Kingsley RA, et al. Invasive non-typhoidal Salmonella disease: an emerging and neglected tropical disease in Africa. Lancet. 2012;379:2489–2499.
25. Cruz AT, Starke JR. Pediatric tuberculosis. Pediatr Rev. 2010;31:13–25.
26. Naudin J, Blonde R, Alberti C, et al. Aetiology and epidemiology of fever in children presenting to the emergency department of a French paediatric tertiary care centre after international travel. Arch Dis Child. 2012;97:107–111.
27. Boggild AK, Castelli F, Gautret P, et al. Vaccine-preventable diseases in returned international travelers: results from the GeoSentinel Surveillance Network. Vaccine. 2010;28:7389–7395.
28. Centers for Disease Control and Prevention. Summary of notifiable diseases, United States, 2010. MMWR Morb Mort Wkly Report. 2012;59:1–111.
29. Wilson ME, Weld LH, Boggild A, et al. Fever in returned travelers: results from the GeoSentinel Surveillance Network. Clin Infect Dis. 2007;44:1560–1568.
30. Bouri N, Sell TK, Franco C, et al. Return of epidemic dengue in the United States: implications for the public health practitioner. Publ Health Rep. 2012;127:259–266.
31. Centers for Disease Control and Prevention and the American Committee on Immunization Practices. Vaccination Recommendations. http://www.cdc.gov/vaccines/pubs/ACIP-list.htm. Accessed August 16, 2012
32. World Health Organization. Expanded Programme on Immunization (EPI). www.who.int/immunization_delivery/en. Accessed August 8, 2012.
33. Azziz-Baumgartner E, Dao C, Nasreen S, et al. Seasonality, timing, and climate drivers of influenza activity worldwide. J Infect Dis. 2012;206(6):838–846.
34. Kulkami MA, Kweka E, Nyale E, et al. Entomological evaluation of malaria vectors at different altitudes in Hai district, northeastern Tanzania. J Med Entomol. 2006;43:580–588.
35. Ndugwa RP, Ramroth H, Muller O, et al. Comparison of all-cause and malaria-specific mortality from two West African countries with different malaria transmission patterns. Malar J. 2008;18: 7–15.
36. Ranjit S, Kissoon N. Dengue hemorrhagic fever and shock syndromes. Pediatr Crit Care Med. 2011;12:90–100.
37. American Academy of Pediatrics. Salmonella. In: Pickering LK, ed 2009 report of the Committee on Infectious Diseases. 28th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2009.