Patrick J. Maloney
Katherine M. Bakes
HIGH-YIELD FACTS
• Examination of the posterior pharynx in patients with hematemesis may reveal a posterior nosebleed as the cause.
• The Apt–Downey test can differentiate swallowed maternal blood from neonatal GI bleeding.
• Vascular malformations are a rare but serious cause of both upper and lower GI bleeding.
• Melena typically indicates proximal bleeding, while hematochezia is usually seen with bleeding from the distal colon and rectum.
A GENERAL APPROACH TO GASTROINTESTINAL BLEEDING
Although the exact incidence of gastrointestinal (GI) bleeding in children is unknown, hematemesis, hematochezia, and melena are common and often anxiety-provoking medical conditions for parents, children, and emergency department (ED) providers. In healthy children, most GI bleeding is minor and self-limited, but occasionally can be life-threatening.
Although most children will be clinically stable, a child with massive GI bleeding may present critically ill and hemodynamically unstable, requiring rapid stabilization. The Pediatric Assessment Triangle facilitates a quick bedside assessment.1
Once stability of a child’s airway, breathing, and circulation has been confirmed, obtain further history and a more complete physical examination to direct secondary management. Information regarding the color (red, coffee-ground, black, or tarry), timing, and volume (drops, “spoonful,” “cupful”) of bleeding is essential, although often difficult to accurately assess.2 Associated symptoms such as abdominal pain, vomiting, fever, diarrhea, and stooling patterns may be helpful. A history of certain pre-existing medical conditions known to be associated with GI bleeding, such as coagulopathy, liver or bowel disease, or recent surgical procedures, may help direct care. Seek a thorough medication history including prescription and nonprescription medicines, such as NSAIDs, corticosteroids, and anticoagulants, among others, that are known to increase the risk for bleeding. Also consider inadvertent or accidental ingestion of medications prescribed to close contacts.
The origin of GI bleeding is often difficult to visualize on physical examination. However, beyond the initial assessment, a focused methodical examination can reveal key diagnostic findings. Examine the nose and pharynx for extra-gastrointestinal bleeding sources such as epistaxis, oropharyngeal trauma, or posttonsillectomy hemorrhage. Look for signs of liver disease, including jaundice, hepatosplenomegaly, and ascites. Bruising or petechiae may indicate an underlying coagulopathy or platelet disorder. In patients with suspected rectal bleeding, carefully examine the perineum, rectum, and anus for anal fissures, hemorrhoids, excoriated skin from diaper rashes, or signs of physical or sexual abuse.
Direct the diagnostic evaluation and treatment according to the child’s level of hemodynamic stability, history, and physical examination. Patients with small and self-limited GI bleeding who are clinically well-appearing require minimal diagnostic testing. If there is any question about the presence of blood, perform a guaiac test.3 Seemingly obvious bloody stool or vomitus may be caused by ingestions of red food dyes, medications (e.g., cefdinir and rifampin), and foods (e.g., beets) rather than bleeding. Bismuth salicylate, iron supplementation, spinach, licorice, cranberries, and other foods can turn stools very dark and be mistaken for melena. False-positive guaiac tests are rare but may be seen with ingestions of red meat or peroxidase-containing fruits and vegetables such as cauliflower, broccoli, turnips, or radishes.4
It is important that extra-gastrointestinal sources of bleeding, such as epistaxis, hemoptysis, hematuria, or menstrual blood, are not mistaken for GI bleeding. Newborns may present with either hematemesis or melena secondary to ingested maternal blood. When it is clinically necessary to differentiate maternal from infant blood, utilize the Apt–Downey test, in which adult hemoglobin turns brown in an alkaline environment. In confirmed GI bleeding a hematocrit will assess for anemia. However, since acute blood loss prior to crystalloid administration will not immediately result in a drop in hematocrit, serial hematocrit measurements are also needed. Order a platelet count and coagulation studies in patients with evidence of life-threatening GI bleeding. If there is concern for large or continued blood loss, order a type and screen (or type and cross if hemodynamic instability is imminent).
Gastric lavage may help identify an upper GI bleed as well as help assess the volume of ongoing hemorrhage. However, gastric lavage is rarely beneficial in practical management and is associated with significant discomfort and risk of aspiration.5,6 Patients with recurrent, continued, or massive GI bleeding may require specialty consultation for emergent endoscopy.
UPPER GASTROINTESTINAL BLEEDING
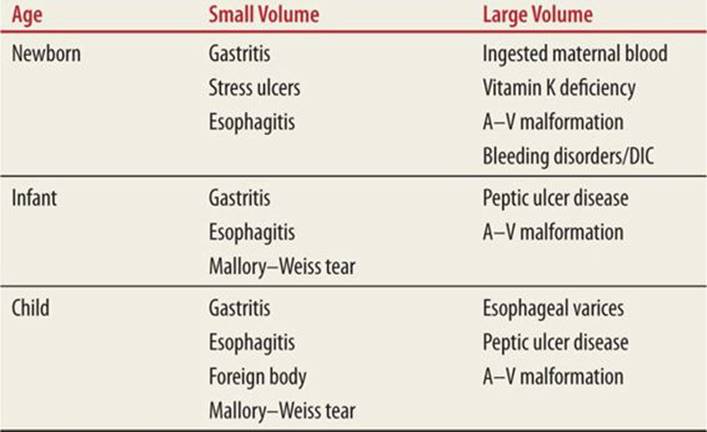
Upper GI bleeding is classically defined as occurring proximal to the ligament of Treitz, and may originate in the esophagus, stomach, or duodenum, with common pediatric causes varying by age (Table 71-1). Although hematemesis is the typical presentation of an upper bleed, 75% of children with bright red rectal bleeding will also have an upper source originating from a brisk upper bleed and rapid intestinal transit time. The distinction is important as upper GI bleeding carries a higher mortality rate compared to lower GI bleeding.7
|
TABLE 71-1 |
Causes of Upper Gastrointestinal Bleeding (BY AGE) |
![]() ESOPHAGU
ESOPHAGU
Inflammatory disorders of the esophagus can result in irritation of the mucosa and subsequent bleeding. Gastroesophageal reflux is the most common cause of esophageal inflammation and may present with regurgitation, abdominal or chest pain, cough, and food refusal.8 (See Chapter 72 for a detailed review of gastroesophageal reflux.) Esophageal infections from Candida, cytomegalovirus, and herpes occur most commonly in immunocompromised children presenting with severe chest or abdominal pain, fever, dysphagia, and odynophagia; if bleeding occurs, it is typically small in volume. Many patients with reflux esophagitis can be treated empirically with lifestyle modifications and acid suppression with either an H2 antagonist (ranitidine 5–10 mg/kg/day PO divided two or three times daily, max 300 mg/day or famotidine 1–2 mg/kg/day divided twice daily, max 80 mg/day) or a proton pump inhibitor (PPI) (esomeprazole 10–20 mg PO twice daily, lansoprazole 7.5–30 mg PO once or twice daily, omeprazole 10–20 mg PO once daily, pantoprazole 0.5–1 mg/kg PO once daily, max dose 20 mg), but children with infections of the esophagus often require further evaluation and possibly inpatient treatment depending on the severity of their symptoms.
Lacerations of esophageal mucosae (Mallory–Weiss tears) occur in patients with repeated retching, vomiting, or paroxysmal cough, typically occurring at the gastroesophageal junction or in the cardia of the stomach.9 Abdominal pain is usually minimal, and bleeding is self-limited and relatively small in volume.10,11 Most patients are successfully treated with antiemetics and acid suppression.12
Children with known liver disease and portal hypertension are at risk for esophageal varices, coagulopathy, and significant GI bleeding (Fig. 71-1). Although self-limited in up to 50% of patients, variceal bleeding is associated with a mortality rate of up to 8%.9,13 These patients may require packed red blood cell, platelet transfusions, and/or correction of coagulation defects with fresh frozen plasma (10–15 mL/kg) and vitamin K (5–10 mg, subcutaneously for non–life-threatening bleeding, intravenous for life-threatening bleeding). Endoscopy offers diagnosis as well as therapeutic sclerotherapy or banding in severe cases. Medical therapy with intravenous octreotide (loading dose: 1–2 μg/kg IV, max 50 μg; maintenance infusion: 1–2 μg/kg/h IV, max 50 μg/h) or vasopressin (starting dose: 0.002 units/kg/min IV; may titrate to max of 0.01 units/kg/min) may control variceal bleeding in children with portal hypertension, either alone or in conjunction with endoscopic management.12–14
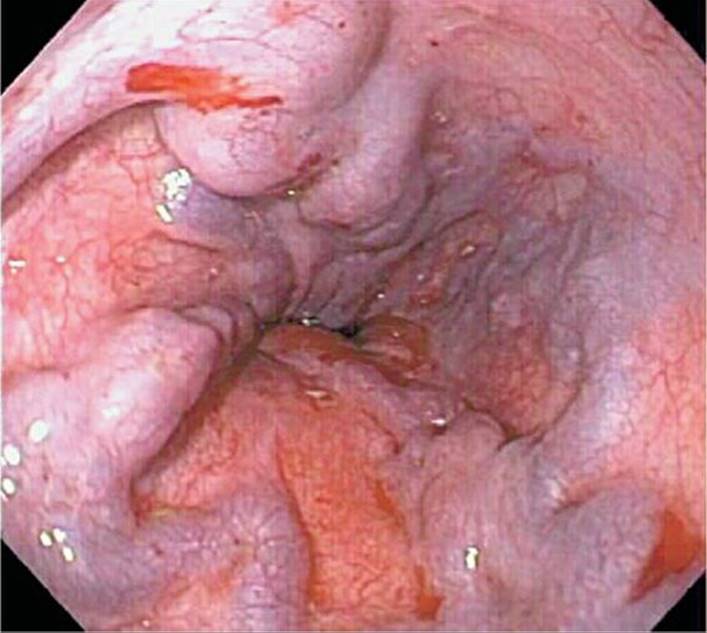
FIGURE 71-1. Multiple oozing esophageal varices seen, extending to gastroesophageal junction in a child with portal hypertension. (Used with permission from Dr. Brian Riedel, Pediatric Gastroenterology, West Virginia University School of Medicine.)
![]() STOMACH/DUODENUM
STOMACH/DUODENUM
Gastritis and peptic ulcer disease are common etiologies of upper GI bleeding (Fig. 71-2). Medications such as NSAIDs, corticosteroids, and iron increase the risk for gastric and duodenal mucosal inflammation. Infection with Helicobacter pylori is a common cause of gastric and duodenal ulcers in healthy children.15 Critically ill children are particularly at risk for development of “stress gastritis,” and prophylactic acid-suppression therapy is essential. Patients with gastritis or ulcers often present with epigastric or left upper quadrant abdominal pain relieved by eating. Hematemesis and melena are usually self-limited, although can be massive and even life threatening, particularly in the setting of ulceration and perforation.12 Although the gold standard for the diagnosis of H. pylori infection is endoscopy with biopsy, noninvasive testing for H. pylori IgG serology and fecal antigen testing are reliable and highly sensitive.16 Gastritis and peptic ulcers can be treated with acid suppression (PPI: esomeprazole 10–20 mg PO twice daily, lansoprazole 7.5–30 mg PO once or twice daily, omeprazole 10–20 mg PO once daily, pantoprazole 0.5–1 mg/kg PO once daily, max dose 20 mg) and close follow-up provided the bleeding is minimal and self-limited.17 Initiate antimicrobial therapy if infection with H. pylori is confirmed. There are three common first-line treatment regimens, although with no consensus on superiority of any one regimen: (1) Standard PPI dose plus clarithromycin 15 mg/kg/day divided twice daily, max 1 g/day, and amoxicillin 40mg/kg/day divided twice daily, max 1 g/day, for 10 to 14 days; (2) Standard PPI dose plus clarithromycin 15 mg/kg/day divided twice daily, max 1 g/day, and metronidazole 15 to 20 mg/kg/day divided twice daily, max 1 g/day, for 10 to 14 days; and (3) Bismuth Subsalicylate 252 to 524 mg PO four times daily plus metronidazole 15 to 20 mg/kg/day divided twice daily, max 1 g/day, and amoxicillin 40 mg/kg/day divided twice daily, max 1 g/day, for 10 to 14 days. Endoscopy is typically reserved for severe or persistent symptoms.
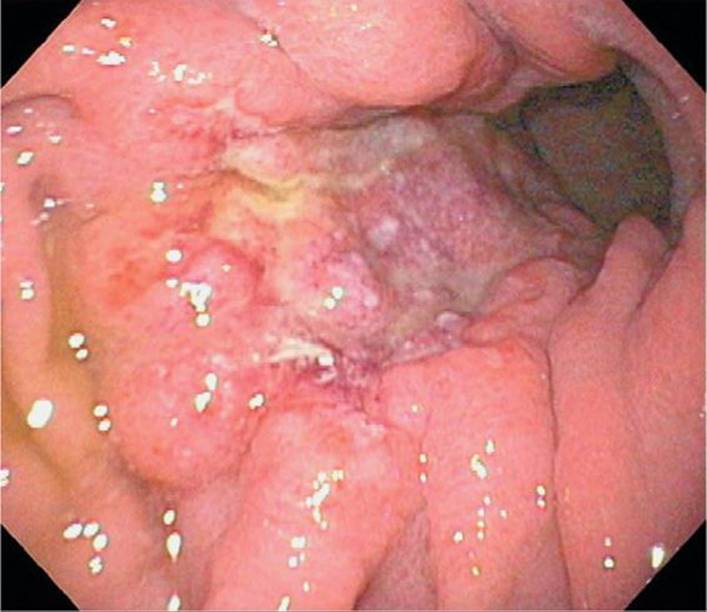
FIGURE 71-2. Deep crater peptic ulcer seen in the fundus of the stomach on endoscopy. (Used with permission from Dr. Brian Riedel, Pediatric Gastroenterology, West Virginia University School of Medicine.)
Vascular malformations are a rare but important cause of GI bleeding and may be present anywhere along the GI tract. They typically present with painless, massive, and recurrent hemorrhage in the absence of other symptoms. Endoscopy is valuable for the identification and possible therapeutic management of either proximal or distal lesions. For vascular lesions not visualized by endoscopy, computed tomography (CT) or magnetic resonance imaging may be helpful.18 For slow, yet persistent bleeding (at least 0.1 mL/min), a radioisotope-labeled red blood cell scan may be diagnostic. Although difficult to perform in children, angiography will detect brisk bleeding (1–2 mL/min), and identify vessels an enable to embolization.10 Dieulafoy malformations, upper GI submucosal vessels occur in the stomach without overlying ulceration, and can cause massive bleeding; detection is difficult by endoscopy since these lesions have a tendency to retract and thus not be visible.7
Keep a high level of suspicion for a foreign body causing GI bleeding in young children with a history of choking, unexplained coughing, dysphagia, or food refusal. Button batteries are of particular concern, as erosion and severe esophageal mucosal injury can occur in as little as 2 hours post-ingestion. Although some objects may be visible on plain radiography, many foreign bodies will be transparent on images, requiring further investigations such as CT scan or endoscopy. (See Chapter 74 for a detailed discussion of GI foreign bodies.)
LOWER GASTROINTESTINAL BLEEDING
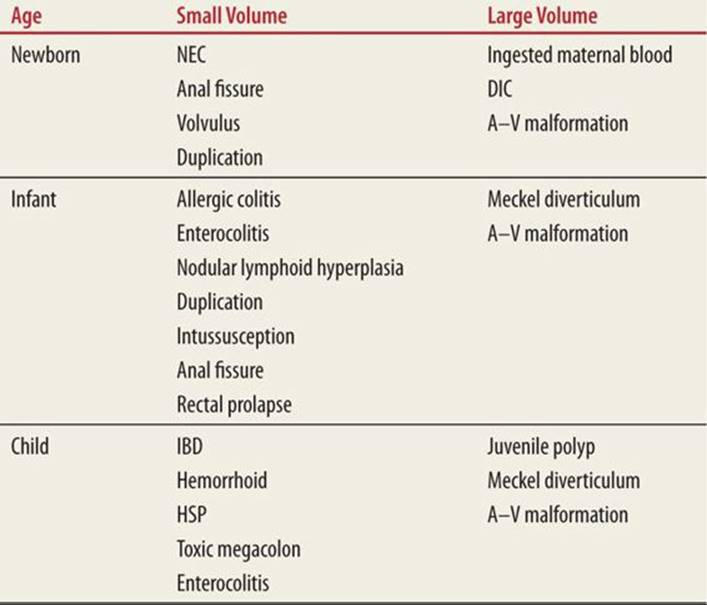
Lower GI bleeding, presenting as melena or hematochezia, can occur anywhere distal to the ligament of Treitz, including the small intestine, colon, rectum, and anus. Causes of lower GI bleeding vary by age (Table 71-2). Although bloody stools are a common complaint, encompassing 0.3% of pediatric ED visits overall, most causes are relatively benign and self-limited.4 The actual bleeding source, however, may be difficult to identify. Melena typically indicates a more proximal source and occurs when blood has been present in the GI tract for a prolonged period of time, resulting in breakdown of hemoglobin.19Small-volume hematochezia is typically from the distal colon or anus, although large-volume rectal bleeding can result from lesions any place along the GI tract if bleeding is brisk.
|
TABLE 71-2 |
Causes of Lower Gastrointestinal Bleeding (BY AGE) |
![]() INTESTIN
INTESTIN
A common cause of lower GI bleeding in children is infectious enterocolitis. Enterocolitis occurs among children of all ages and can result in abdominal pain, fever, and bloody stools. Common pathogens implicated in bloody diarrhea include Salmonella, Shigella, Campylobacter jejuni, Yersinia enterocolitica, Escherichia coli, Clostridium difficile, and Entamoeba histolytica.4 Although most enterocolitis is self-limited, rare complications such as hemolytic uremic syndrome can occur; thus, children with infectious enterocolitis and bloody diarrhea may require additional testing with close follow-up. Diagnosis can be made by stool culture or antigen testing. Most cases of infectious enterocolitis in otherwise healthy children do not require specific treatment; avoid antimotility agents. Antimicrobial therapy may worsen the clinical course in some cases and are only recommended for patients with documented Shigella, Campylobacter, C. difficile, or E. histolytica enterocolitis as well as very young or immunocompromised children and those with sepsis or septic shock.20
Necrotizing enterocolitis (NEC) is a rare but serious cause of neonatal lower GI bleeding. Although it is most common in premature newborns in the intensive care unit, neonates may present to the ED. These infants often have a history of prematurity, significant anoxic stress at birth, or cyanotic congenital heart disease, all leading to gut hypoperfusion.21,22 Infants with NEC appear ill with lethargy, abdominal distension, vomiting, and bloody stools. Abdominal radiographs may reveal distended loops of bowel, pneumatosis intestinalis, or bowel perforation. Treatment involves fluid resuscitation, bowel rest, broad-spectrum antimicrobials, and emergent surgical consultation.21
Children with Hirschsprung disease can develop toxic megacolon and may present acutely ill with abdominal distension, fever, explosive diarrhea, hematochezia, and abdominal pain. Toxic megacolon may be the initial presentation of Hirschsprung disease, but may also occur after surgical resection of the aganglionic segment, particularly in children with longer segment disease or Down syndrome.23 Intestinal dilation with air–fluid levels can be seen on plain abdominal radiography, often with an intestinal cutoff sign (abrupt cutoff of intestinal distension at the pelvic brim, Fig. 71-3).24 Treatment involves bowel decompression, hydration, and broad-spectrum antibiotics.23

FIGURE 71-3. Intestinal cutoff sign seen in a child with toxic megacolon. This child had previously undergone resection of his aganglionic colon segment. Note the massive intestinal distension. (Used with permission from Dr. Thomas J. Abramo, Pediatric Emergency Medicine, Vanderbilt University Medical Center.)
Obstructive disorders of the intestine can also cause lower GI bleeding, usually small in volume, secondary to ischemia. Intussusception, the most common cause of obstruction, typically occurs in children younger than 2 years of age. The classic presentation is intermittent colicky abdominal pain and vomiting; some children present with a generalized illness, malaise, or altered mental status. Intussusception can occur anywhere within the bowel, but most commonly at the ileocecal junction. A sausage-shaped abdominal mass may be palpated in the right lower quadrant or anywhere along the ascending or transverse colon, depending on the extent of bowel telescoping. Bleeding from an intussusception is classically described as “currant-jelly,” although this appearance is present in only approximately 10% of confirmed cases of intussusception.25 Hematochezia, from bowel ischemia, is a late and ominous finding.4 More commonly, bleeding is only detectable by guaiac testing, and lack of blood in the stool does not exclude intussusception. Abdominal radiographs may show a classic “target sign” or paucity of bowel gas in the right lower quadrant, but may also be normal.21 Ultrasound is a more sensitive and specific modality for the diagnosis of intussusception, with the added benefit of lacking ionizing radiation.26 With the growing role of ultrasound, air-contrast enema is less often used for the primary diagnosis, but remains the therapeutic modality of choice for uncomplicated intussusception. Complications such as failure to reduce the intussusception or bowel perforation with possible tension pneumoperitoneum can occur, necessitating surgical consultation availability.
Volvulus can also present with rectal bleeding from bowel ischemia, most commonly in neonates with congenital malrotation of the midgut; typical presentations include bilious vomiting, abdominal distension, and refusal to feed. Abdominal radiographs may reveal a paucity of gas in the abdomen with a “double bubble sign,” which is a foci of gas seen in the dilated stomach and duodenum. An upper GI contrast study is the diagnostic study of choice. Fluid resuscitation, antimicrobials, and emergent surgical reduction of the volvulus are critical to preserve bowel viability. Duplication of the bowel can also result in bowel ischemia and bleeding from intussusception, volvulus, or expansion of the duplication.4
Meckel diverticulum, resulting from incomplete obliteration of the omphalomesenteric duct during fetal development, is a common cause of otherwise asymptomatic bleeding in the small intestine. The “rule of 2’s” characterizes the classic Meckel diverticulum as 2 inches long, occurring within 2 ft of the ileocecal valve, and present in approximately 2% of the population.4,27 If the diverticulum contains ectopic gastric mucosa, ulceration and massive (typically, painless) bleeding can occur. For diagnosis, a radionuclide scan with technetium-99m pertechnetate, or “Meckel scan,” utilizes a radioisotope that preferentially binds to gastric mucosa.4 Treatment involves medical resuscitation if hemadymmedially instable, surgical consultation and bowel resection for definition care.27
Juvenile polyps are a common cause of GI bleeding outside the neonatal period. Bleeding is typically painless, recurrent, and small in quantity. Most polyps in children are solitary, benign, and occur within the left colon, often in the rectosigmoid region.19 Diagnosis is made by direct visualization with endoscopy, which also allows for therapeutic excision (Fig. 71-4).
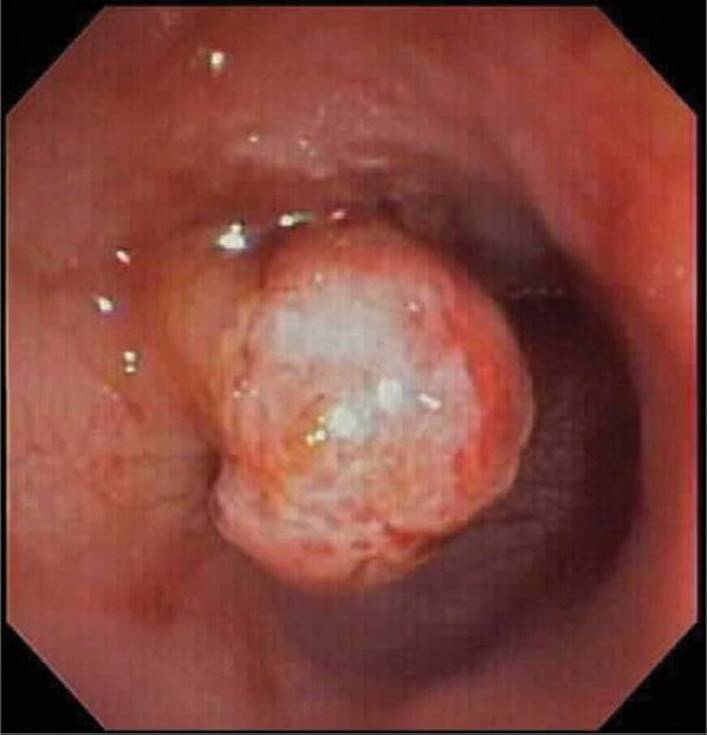
FIGURE 71-4. A 0.7-cm pedunculated polyp was identified in the sigmoid colon of a child presenting with painless rectal bleeding. (Used with permission from Dr. Brian Riedel, Pediatric Gastroenterology, West Virginia University School of Medicine.)
Intestinal inflammatory disorders can cause lower GI bleeding. Up to 15% of infants have IgE-mediated milk protein allergic colitis, responsible for up to 20% of rectal bleeding in children less than 1 year old.28 These infants are usually well-appearing but may present with poor weight gain, anemia, metabolic derangements, or failure to thrive. Most infants are treated empirically with exclusion of any known allergens.28 Soy-based foods and formulas should also be eliminated due to 60% cross-reactivity with animal proteins. Even with dietary modification, bloody stools can persist for weeks.29
Inflammatory bowel disease (IBD), ulcerative colitis and Crohn disease, most commonly occurs in adolescents, causing crampy abdominal pain, frequent bloody stools, tenesmus, and weight loss (Fig. 71-5). While ulcerative colitis involves only the colon, Crohn disease can involve any portion of the GI tract. Laboratory evaluation may reveal anemia, thrombocytosis, or an elevated ESR; colonoscopy with biopsy is required for definitive diagnosis.30Therapy involves anti-inflammatory and immunosuppressive medications, and rarely surgical resection.
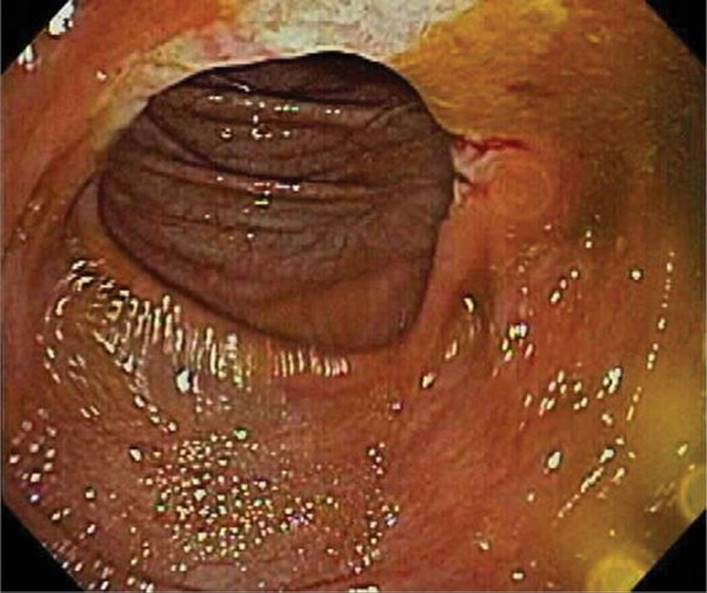
FIGURE 71-5. Edema, friability, and ulceration of colon seen on endoscopy in a child with ulcerative colitis. (Used with permission from Dr. Brian Riedel, Pediatric Gastroenterology, West Virginia University School of Medicine.)
Henoch–Schönlein Purpura (HSP), an immune-mediated vasculitis which can involve the entire GI tract, can have GI manifestations including abdominal pain, vomiting, and bloody stools. Although bleeding is usually due to mucosal hemorrhage, lesions can act as a lead point for developing intussusception with the potential for bleeding from bowel ischemia. HSP is diagnosed clinically, particularly challenging when GI manifestations precede the pathognomonic purpuric skin changes. Although there is no current consensus on treatment, corticosteroids may ameliorate GI symptoms.31
Colonic lymphonodular hyperplasia from protein allergy or infection can result in asymptomatic, small-volume bleeding. More common in infants and young children, these inflammatory patches present with flecks of blood mixed in the stool of otherwise asymptomatic children. Lymphonodular hyperplasia is diagnosed on colonoscopy and does not require any specific treatment (Fig. 71-6).32

FIGURE 71-6. Diffuse lymphonodular hyperplasia is seen in this child undergoing colonoscopy for rectal bleeding. (Used with permission from Dr. Brian Riedel, Pediatric Gastroenterology, West Virginia University School of Medicine.)
![]() RECTUM/ANU
RECTUM/ANU
Benign lesions of the rectum and anus can cause apparent lower GI bleeding. Anal fissures, the most common cause of rectal bleeding in infants, present with bright red blood external to the stool and typically caused by passing painful, hard stools. Hemorrhoids, resulting in painful defecation with bloody spotting, are uncommon in young children, but can occur after prolonged constipation in adolescents. Diagnosis is made on physical examination, with treatment directed at dietary modifications and stool softeners. Young children with constipation are predisposed to rectal prolapse, which may result in scant rectal bleeding (Fig. 71-7). The prolapsed segment often self-reduces, with the diagnosis made on history alone. If a child presents with rectal prolapse, apply firm constant pressure to reduce, otherwise, surgical consultation is necessary; prescribe stool softeners to minimize recurrence (polyethylene glycol 0.5–1 g/kg BID, max 17 g/day, for up to 8 weeks). Trauma from sexual abuse may also present as rectal bleeding.

FIGURE 71-7. Rectal prolapse was seen on examination of this child presenting with rectal pain and bleeding. (Used with permission from Dr. Thomas J. Abramo, Pediatric Emergency Medicine, Vanderbilt University Medical Center.)
REFERENCES
1. Dieckmann RA, Brownstein D, Gausche-Hill M. The pediatric assessment triangle: a novel approach for the rapid evaluation of children. Pediatr Emerg Care. 2010;26(4):312–315.
2. Tebruegge M, Misra I, Pantazidou A, et al. Estimating blood loss: comparative study of the accuracy of parents and health care professionals. Pediatrics. 2009;124(4):e729–e736.
3. Allison JE, Tekawa IS, Ransom LJ, Adrain AL. A comparison of fecal occult-blood tests for colorectal– cancer screening. N Engl J Med. 1996;334:155–159.
4. Leung AK, Wong AL. Lower gastrointestinal bleeding in children. Pediatr Emerg Care. 2002;18:319–323.
5. Pitera A, Sarko J. Just say no: gastric aspiration and lavage rarely provide benefit. Ann Emerg Med. 2010;55(4):365–366.
6. Singer S, Richman P, LaVefre R, Thode HC Jr. Comparison of patient and practitioner assessments of pain from commonly performed emergency department procedures. Acad Emerg Med. 1997;4;404–405.
7. Burke SJ, Golzarian J, Weldon D, Sun S. Nonvariceal upper gastrointestinal bleeding. Eur Radiol. 2007;17:1714–1726
8. Gupta SK, Hassall E, Chiu YL, Amer F, Heyman MB. Presenting symptoms of nonerosive and erosive esophagitis in pediatric patients. Dig Dis Sci. 2006;51:858–863.
9. Chawla S, Seth D, Mahajan P, Kamat D. Upper gastrointestinal bleeding in children. Clin Pediatr (Phila). 2007;46:16–21.
10. Boyle JT. Gastrointestinal bleeding in infants and children. Pediatr Rev. 2008;29:39–52.
11. Esrailian E, Gralnek IM. Nonvariceal upper gastrointestinal bleeding: epidemiology and diagnosis. Gastroenterol Clin North Am. 2005;35:589–605.
12. Rodgers BM. Upper gastrointestinal hemorrhage. Pediatr Rev. 1999;20:171–174.
13. Molleston JP. Variceal bleeding in children. J Pediatr Gastroenterol Nutr. 2003;37:538–545.
14. Eroglu Y, Emerick KM, Whitingon PF, Alonso EM. Octreotide therapy for control of acute gastrointestinal bleeding in children. J Pediatr Gastroenterol Nutr. 2004;38(1):41–47.
15. Blecker U, Gold BD. Gastritis and peptic ulcer disease in childhood. Eur J Pediatr. 1999;158:541–546.
16. Sabbi T, De Angelis P, Colistro F, Dall’Oglio L, di Abriola GF, Castro M. Efficacy of noninvasive tests in the diagnosis of Helicobacter pylori infection in pediatric patients. Arch Pediatr Adolesc Med.2005;159:238–241.
17. Olson AD, Fendrick AM, Deutsch D, et al. Evaluation of initial noninvasive therapy in pediatric patients presenting with suspected ulcer disease. Gastrointest Endosc. 1996;44:554–561.
18. Dubois J, Rypens F, Garel L, Yazbeck S, Therasse E, Soulez G. Pediatric gastrointestinal vascular anomalies: imaging and therapeutic issues. Pediatr Radiol. 2007;37:566–574.
19. Lawrence WW, Wright JL. Causes of rectal bleeding in children. Pediatr Rev. 2001;22:394–395.
20. Pickering LK, Baker CJ, Long SS, et al. Red Book: 2006 Report of the Committee on Infectious Diseases. 27th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2006.
21. McCollough M, Sharieff GQ. Abdominal surgical emergencies in infants and young children. Emerg Med Clin North Am. 2003;21:909–935.
22. Hostetler MA, Schulman M. Necrotizing enterocolitis presenting in the emergency department: case report and review of differential considerations for vomiting in the neonate. J Emerg Med.2001;21:165–170.
23. Dasgupta R, Langer J. Evaluation and management of persistent problems after surgery for Hirschprung disease in a child. J Pediatr Gastroenterol Nutr. 2008;46:13–19.
24. Elhalaby EA, Coran AG, Blane CE, Hirschl RB, Teitelbaum DH. Enterocolitis associated with Hirschprung’s disease: a clinical-radiological characterization based on 168 patients. J Pediatr Surg.1995;30:76–83.
25. Yamamoto LG, Morita SY, Boychuk RB, et al. Stool appearance in intussusception: assessing the value of the term “currant jelly”. Am J Emerg Med. 1997;15(3):293–298.
26. Hryhorczuk AL, Strouse PJ. Validation of US as a first-line diagnostic test for assessment of pediatric ileocolic intussusception. Pediatr Radiol. 2009;39(10):1075–1079.
27. Rodrigues F, Brandao N, Duque V, Ribeiro C, António AM. Herpes simplex virus esophagitis in immunocompetent children. J Pediatr Gastroenterol Nutr. 2004;39:560–563.
28. Aryola T, Ruuska T, Keranen J, Hyöty H, Salminen S, Isolauri E. Rectal bleeding in infancy: clinical, allergological, and microbiological examination. Pediatrics. 2006;117:e760–e768.
29. Xanthakos SA, Schwimmer JB, Melin-Aldana H, Rothenberg ME, Witte DP, Cohen MB. Prevalence and outcome of allergic colitis in healthy infants with rectal bleeding: a prospective cohort study. J Pediatr Gastroenterol Nutr.2005;41:16–22.
30. Beattie RM, Croft NM, Fell JM, Afzal NA, Heuschkel RB. Inflammatory bowel disease. Arch Dis Child. 2006;91:426–432.
31. Weiss PF, Feinstein JA, Luan X, Burnham JM, Feudtner C. Effects of corticosteroid on Henoch-Schoenlein purpura: a systematic review. Pediatrics. 2007;120:1079–1087.
32. Berezin S, Newman LJ. Lower gastrointestinal bleeding in infants owing to lymphonodular hyperplasia of the colon. Pediatr Emerg Care. 1987;3:164–165.