Jannet J. Lee-Jayaram
HIGH-YIELD FACTS
• With currently existing fast magnetic resonance imaging (MRI) techniques, it is possible to evaluate for shunt malfunction in less than 90 seconds.
• CT findings of ischemic stroke lag far behind diffusion-weighted MRI findings, which can detect edema within the first hour after the event.
• MRI is the imaging modality recommended by the American College of Radiology for identifying appendicitis in pregnant patients who have a nondiagnostic ultrasound.
• Whole-body MRI is used in metastatic cancer staging and has a higher sensitivity and specificity over scintigraphy in this application. Image acquisition times of 30 to 45 minutes are similar.
• 3.0T magnets are becoming more widely available and provide thinner-slice, higher-resolution images in a shorter amount of time than the current standard 1.5T magnet machines.
MAGNETIC RESONANCE IMAGING BASICS
Magnetic resonance (MR) imaging is a technique that uses an external magnetic field and its specific effect on various atomic nuclei to produce detailed images of different tissues in the body. The magnet in the MR machine is large and cylindrically coiled, surrounded by a cooling agent such as liquid helium to allow for magnet super conduction. Computers generate the pulse sequences, collect the data, and transform the data into interpretable images. MR contrast agents are typically gadolinium-based agents. The major advantages of MR imaging (MRI) are the excellent detail in various planes when imaging areas require soft-tissue differentiation and the lack of ionizing radiation to the body. Greater awareness of the risks of ionizing radiation, including the increased risk of cancer and cognitive harm, has also led to expanding the applications of MRI to the evaluation and management of pediatric disease.1,2While CT imaging depends solely on the density gradients of tissues, MRI is a complex function of small differences in the tissues’ excitability from the applied magnetic field. MRI provides more flexibility for radiologists with the use of various sequences to elucidate fine details in differences of the tissues depending on the area of the body to be imaged. Areas of the body poorly visualized by CT due to artifact, such as the posterior fossa of the brain, are well defined on images obtained by MRI.
MR PRECAUTIONS
There are no established biologic effects associated with exposure to current medical standard MRI; however, few precautions do exist with respect to the powerful magnet in the machine,3 such as implanted or embedded electric or ferromagnetic devices. A thorough screening of each patient should take place for such devices or objects and all removable items such as jewelry, hair clips, metallic clothing should be taken off. There is also the danger of magnetic attraction of nearby devices and equipment, which can lead to missiles that may injure the patient and staff. Most resuscitation equipment cannot be brought in close proximity to the magnet, making clinically unstable patients unsuitable for MRI. Other effects include the heating of tissues, peripheral nerve stimulation, thermal injury caused by heating of applied patches or adhesives, and claustrophobia.4 Compared with agents used for CT, MR agents have typically fewer side effects and anaphylactoid reactions.5 However, a rare and possibly fatal nephrogenic systemic fibrosis that is related to concomitant severe renal dysfunction and the administration of gadolinium-based contrast agents6 should be included in the informed consent process for those patients receiving contrast for MRI.
When ordering a MRI, consultation with a radiologist facilitates the determination of the most optimal sequences that need to be obtained. Although a few sequences are discussed in the following section, these are not described in great detail and are for the purpose of general familiarity for the nonradiologist emergency medicine provider.
BRAIN
Fast MRI techniques such as single-shot fast spin echo (SSFSE) provides T2-weighted images within 20 seconds and echo planar imaging (EPI) provides T1-weighted images within 90 seconds. These techniques can image the pediatric brain without the need for sedation; however, there is poorer gray–white differentiation with SSFSE and artifact around the skull base with the EPI sequences.7 Due to these limitations, the techniques may not yet be applied for evaluation of demyelination or migration disorders, as well as for evaluating acute hemorrhage.7,8
![]() HYDROCEPHALUS
HYDROCEPHALUS
Although CT has been the common method of assessing ventriculoperitoneal shunt function, at two CT scans per year to age 20 years, the accumulated radiation exposure has an attributable risk of developing a fatal cancer of 1 in 230.9 Elimination of CT scans in this population could have a significant impact on radiation-associated disease. Using fast MRI techniques, visualization of the size and configuration of ventricles has been demonstrated, although there may be poorer visualization of the shunt catheter and the detection of hemorrhage.10,11 Figure 16-1 demonstrates shunt malfunction in a 7-year-old boy with shunted hydrocephalus due to aqueductal stenosis using a T2-weighted SSFSE image obtained in 30 seconds. Some institutions already have in place a protocol for rapid MRI upon suspicion of shunt malfunction using these techniques.11 Image acquisition is fast enough such that they are performed without sedation.
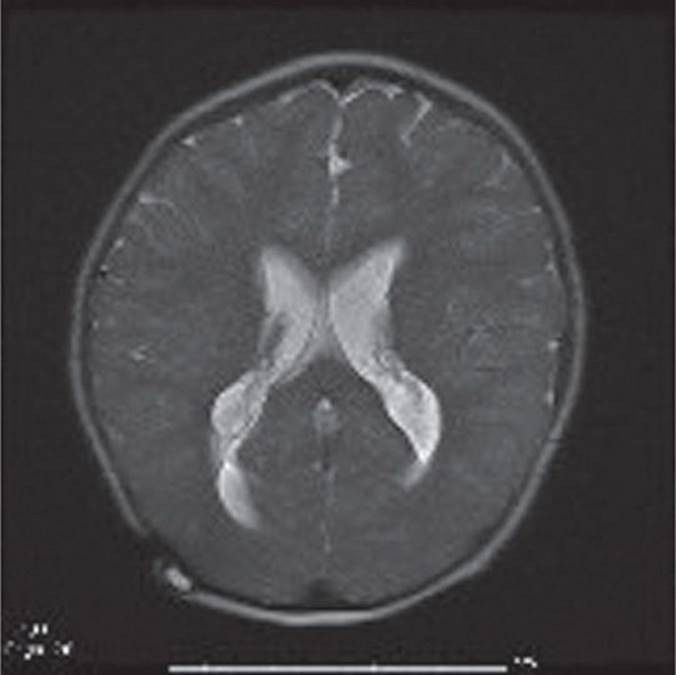
FIGURE 16-1. T2-weighted SSFSE sequence obtained in 30 seconds demonstrating ventriculomegaly from shunt malfunction in a 7-year-old boy with shunted hydrocephalus from aqueductal stenosis presenting with vomiting, headache, and lethargy. (Used with permission from Dr. Bogna Targonska.)
![]() OTHER BRAIN
OTHER BRAIN
MRI has the potential to replace CT scans for emergency department (ED) brain imaging for other causes as well. The most recent American College of Radiology (ACR) appropriateness criteria from 2012 recommend MRI as the initial study for children with chronic headache or headache with signs of increased intracranial pressure and neurologic signs, assuming MRI availability.12 CT is recommended first-line evaluation technique only for those presenting with sudden-onset severe headache concerning for vascular rupture, due to its superior ease of detecting acute hemorrhage. When compared with standard MR sequences, these fast MR techniques were noted to perform well with respect to detection of acute ischemia, infection, hydrocephalus, and tumor.8 These fast sequences did not perform as well as standard MR sequences with respect to congenital malformations, specifically those with cortical abnormalities and detecting subarachnoid hemorrhage (SAH).13 When compared with CT, these fast techniques were noted to be clearly superior, detecting 38% of abnormalities, mainly in the posterior or middle cranial fossae, that CT did not.7 The abnormalities missed by CT scan included ischemia/infarction, encephalitis, mastoiditis, thrombosis, parenchymal hemorrhage, and contusions. Standard MR sequences performed well at detecting subacute hemorrhage on gradient echo T2* and fluid attenuated inversion recovery (FLAIR) sequences, especially with elucidating associated ischemia. CT still remains the standard for imaging acute SAH. Often, the need for brain imaging in the ED, if not concerned about SAH, is to evaluate for possible mass effect or hydrocephalus to plan ongoing therapeutic management and evaluation. These fast techniques appear to adequately screen for these or at least determine the need for traditional MRI sequences.
For ataxia, ACR criteria recommends first-line evaluation with MR, except in the setting of acute trauma,14 since the posterior fossa is poorly visualized by CT. Ataxia can be a manifestation of stroke, infection, demyelination, degenerative processes, or masses, all of which are detected with great detail by MRI. With the advent of the fast techniques mentioned previously, the ataxic child presenting to the ED may be able to have a MR image which is much more sensitive at detecting lesions in the area of concern.
![]() TRAUMATIC BRAIN INJURY
TRAUMATIC BRAIN INJURY
CT is still the mainstay of evaluation of an acutely head-injured child with evidence of significant trauma or neurologic deficit due to its superior ability to detect acute hemorrhage (especially SAH), bony injury, and its immediate availability. However, there may be a role for MRI in the evaluation of the stable, subacutely injured child, including those who may present for evaluation of nonaccidental trauma. In the stable child, without evidence of significant acute injury and nonfocal neurologic examination, the patient may benefit more from having a MRI if immediate neurosurgical intervention is unlikely.15 MRI is more sensitive than CT in evaluating parenchymal injury including contusions, diffuse axonal injury, edema, and early ischemia. It is also superior at differentiating chronic subdural hemorrhage from benign collections and further defining small subdural collections close to the calvarium which may not be detected by CT.16 The extra information provided by MRI may impact the forensic evidence in the case of proven inflicted injury, as well as suggesting prognosis and need for ongoing therapeutic treatments for the injured child.17
![]() STROK
STROK
Pediatric stroke is due to both arterial ischemic insufficiency and hemorrhage, with a very small percentage due to sinus venous thrombosis. Congenital abnormalities, infections, hematologic abnormalities, vascular malformations, congenital heart disease, hypercoagulable states, and vasculopathies are some causes of arterial ischemic pediatric stroke. Sickle cell disease and congenital heart disease are the underlying etiology in the majority of cases. The presentation of arterial ischemic stroke in children may be subtle, with focal neurologic deficits, seizures, altered mental status, and headache. CT findings of ischemic stroke lag far behind diffusion-weighted MRI findings which can detect the early effects of cytotoxic edema from ischemia as early as 30 to 45 minutes after the event.18 Figure 16-2 demonstrates this contrast in a 16-year-old baseball player with sudden-onset collapse, dense right hemiparesis, and aphasia. CT is also inferior to MRI at detecting sinus venous thrombosis. The addition of diffusion-weighted imaging sequences in addition to standard sequences can be used to detect acute ischemia and are highly resistant to motion artifact and can be obtained in less than 2 minutes.18 CT has advantages for hemorrhagic stroke (including intraparenchymal and SAH), which accounts for half of pediatric stroke, and is heralded by abrupt clinical onset and subsequent neurologic deterioration. However, early MRI to follow closely after normal CT or to replace CT in stable patients (if MRI is immediately available) would add more information to the diagnosis, specifically with additional information about early ischemia. MR angiography could also be obtained at the same time if vascular malformation is suspected. ACR appropriateness criteria on cerebrovascular disease almost universally recommend MRI over CT if available, with the exception of suspected SAH.19 Although traditional sequences have not been able to reliably identify SAH, more recent experience with alternative sequences such as T2* gradient echo and FLAIR have allowed for improved recognition and characterization of intracranial blood, including SAH.20
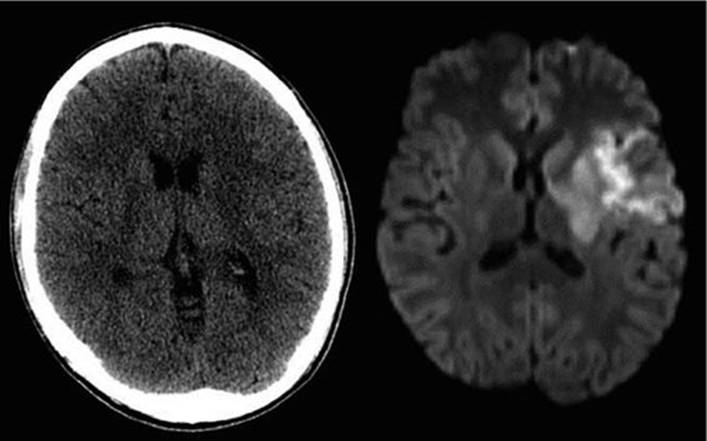
FIGURE 16-2. CT head and comparable MRI DWI sequence for a 16-year-old baseball player diagnosed with left middle cerebral artery (MCA) ischemic stroke who presented with sudden collapse, right hemiparesis, and aphasia. CT head is essentially normal, whereas MRI with DWI demonstrates restricted diffusion in the distribution of the left MCA. (Used with permission from Dr. Bogna Targonska.)
ABDOMEN AND PELVIS
MRI is currently the standard recommended by the ACR for identifying appendicitis in pregnant women in whom ultrasound results are nondiagnostic or equivocal.21 The sensitivity and specificity of MRI in identifying appendicitis is comparable to that of CT scan, even without the administration of oral contrast.22 Alternative causes for acute pelvic pain are also identified on MRI including ovarian/adnexal torsion, pelvic inflammatory disease, and colitis.23 For pelvic pain in premenopausal women, ACR recommends MRI as second-line imaging following an inconclusive or technically limited pelvic ultrasound and Doppler.24 Limitations to using MRI for evaluating acute pelvic pain are the limited availability of MRI and as well as the prolonged scanning time, which approaches 20 to 25 minutes. However, there has been successful implementation of MRI as the sole imaging study for evaluation of appendicitis in children using only four sequences, no contrast and no sedation.25 The acquisition of the four sequences took a mean time of 14 minutes, but under 10 minutes in cooperative children, without any failures to complete the examination. Appendicitis was successfully identified in children aged 5 to 17 years with a sensitivity of 98% and negative predictive value of 99%. In a smaller feasibility study using a 3T magnet, similar sequences were obtained in under 9 minutes with 100% sensitivity and negative predictive value.26 Children aged 4 to 17 years were imaged successfully without sedation and without any contrast. Both of these studies demonstrate the feasibility of MRI in evaluating children with acute lower abdominal pain, eliminating the need for CT. Offsetting the higher cost of MRI could be achieved by first starting with the more cost-effective strategy of ultrasound and then only those with equivocal results going on to MRI. Such a similar-staged protocol using ultrasound first and then CT scan if necessary has demonstrated to be highly accurate and effective in the diagnosis of pediatric appendicitis.27 The advantage of MRI over ultrasound is that image acquisition and quality are not operator dependent, as well as its ability to better identify alternate intra-abdominal/pelvic causes of pain.
SPINE
Back pain in children occurs more commonly than previously thought. Extensive workups reveal low rates of identifiable disease.28,29 Back pain may suggest diskitis, osteomyelitis, tumor, or other inflammatory conditions and in the right clinical setting warrants investigation. In addition to clinically guided laboratory investigations for the underlying cause of the back pain, imaging studies are also often obtained. If diagnostic imaging is required, plain radiography may be a good initial diagnostic tool for the evaluation of back pain. After that first step, MRI may be the next best step due to its ability to evaluate for serious pathology as described above as well as evaluation of the spinal cord.30 While CT identifies fractures well, MRI provides more information regarding the other possible causes of back pain including paraspinal, intraspinal contents, intervertebral disks, infection and congenital malformations. It is limited by the fact that younger children will likely require sedation due to prolonged image acquisition times, even when the field of view is limited to the area of concern. MRI can provide details that CT cannot about osseous structures, including edema suggestive of stress fractures. Except in trauma, if neurologic function is affected or myelopathy is present, ACR recommends MRI since it can provide crucial information regarding the spinal cord.31,32 CT remains more sensitive than MRI in detecting fractures, as cortical bone is not well defined on traditional MR sequences.33
BONY SKELETON
Imaging is required during the evaluation and management of musculoskeletal infection to confirm the clinical diagnosis, help with staging, plan surgical intervention, and monitor response to therapy.34Although MRI is superior to scintigraphy at the detection of bony infection once the location of site of infection is known or suspected, it is currently limited by the need to know the field of view.35 Once the location is identified, MRI can be used to delineate with excellent detail the early manifestations of bony involvement, in addition to any surrounding complicating factors including pyomyositis and abscesses that may affect management decisions, such as the need for an operative procedure.36 Routine radiography is not useful early in the disease process and it may not demonstrate bony changes until 7 to 10 days after onset of symptoms, with the majority not displaying lesions even within the second week.37Scintigraphy exposes children to radiation and its specificity is low, requiring further imaging to establish a diagnosis.35,37 Given the current use of whole-body MRI in metastatic cancer staging and its higher sensitivity and specificity over scintigraphy in this application, it is not difficult to anticipate the growth of whole-body MRI in other applications, including evaluation of fever of unknown origin or multifocal osteomyelitis.38 Images can be acquired within 30 to 45 minutes, which is comparable to the time it takes to acquire images for scintigraphy.
3T
Currently, the standard MR machine in clinical use uses a 1.5T (Tesla) magnet. Approved by the FDA in 2000,39 the 3.0T MR technology has advantages such as acquisition of thin-section, high-resolution images in a shorter amount of time.40 Clinical superiority of 3.0T over 1.5T has been demonstrated in contrast-enhanced studies, imaging of the pelvis, angiography, and neuroimaging.39 Shorter scanning times reduce the need for sedation.
MRI AND THE EMERGENCY DEPARTMENT
Traditionally the high cost of MRI, inconsistent availability after-hours, prolonged time of image acquisition, and susceptibility to small motion artifact have been barriers to its use in the ED. Many young children undergo deep sedation to complete these studies. Faster imaging times reduce the need for sedation and advances in sedation have improved its availability.
As providers become familiar with the widening indications for MRI, such requests from the ED should increase while the call for CT scans are likely to decrease. Although the use of all forms of diagnostic radiology and therefore exposure to ionizing radiation has increased, the use of MR has also increased fourfold over the past 15 years.41 Aware of the unique situation of childhood, which combines rapidly dividing tissue with expected long years ahead to develop malignancies, providers are making attempts to reduce childhood exposure to radiation. In recent years at specialty pediatric centers, CT utilization is static, perhaps even decreasing.42 With advancements in technology, it can be anticipated that this trend will spread beyond pediatric centers and to general hospitals where the majority of children receive their care.
REFERENCES
1. Hall P, Adami HO, Trichopoulos D, et al. Effect of low doses of ionising radiation in infancy on cognitive function in adulthood: swedish population based cohort study. BMJ. 2004;328:19.
2. Pearce MS, Salotti JA, Little MP, et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study. Lancet. 2012;380:499–505.
3. Hartwig V, Giovannetti G, Vanello N, Lombardi M, Landini L, Simi S. Biological effects and safety in magnetic resonance imaging: a review. Int J Environ Res Public Health. 2009;6:1778–1798.
4. Kanal E, Borqstede JP, Barkovich AJ, et al. American College of Radiology White Paper on MR safety. AJR Am J Roentgenol. 2002;178:1335–1347.
5. Dillman JR, Ellis JH, Cohan RH, Strouse PJ, Jan SC. Frequency and severity of acute allergic-like reactions to gadolinium-containing iv contrast media in children and adults. AJR Am J Roentgenol. 2007;189:1533–1538.
6. FDA Drug Safety Communication: new warnings for using gadolinium-based contrast agents in patients with kidney dysfunction. 2010. Cited 2012. http://www.fda.gov/Drugs/DrugSafety/ucm223966.htm. Accessed October 5, 2012.
7. Griffiths PD, Wilkinson ID, Patel MC, et al. Acute neuromedical and neurosurgical admissions, standard and ultrafast MR imaging of the brain compared with cranial CT. Acta Radiol. 2000;41:401–409.
8. Penzkofer AK, Pfluger T, Pochmann Y, Meissner O, Leinsinger G. MR imaging of the brain in pediatric patients: diagnostic value of HASTE sequences. AJR Am J Roentgenol. 2002;179:509–514.
9. Koral K, Blackburn T, Bailey AA, Koral KM, Anderson J. Strengthening the argument for rapid brain MR imaging: estimation of reduction in lifetime attributable risk of developing fatal cancer in children with shunted hydrocephalus by instituting a rapid brain MR imaging protocol in lieu of head CT. AJNR Am J Neuroradiol. 2012;33(10):1851–1854.
10. Ashley WW Jr, McKinstry RC, Leonard JR, Smyth MD, Lee BC, Park TS. Use of rapid-sequence magnetic resonance imaging for evaluation of hydrocephalus in children. J Neurosurg. 2005;103:124–130.
11. Iskandar BJ, Sansone JM, Medow J, Rowley HA. The use of quick-brain magnetic resonance imaging in the evaluation of shunt-treated hydrocephalus. J Neurosurg. 2004;101:147–151.
12. Headache—child. American College of Radiology (ACR) Appropriateness Criteria. 1999. Cited 2012. http://www.acr.org/~/media/ACR/Documents/AppCriteria/Diagnostic/HeadacheChild.pdf. Accessed October 5, 2012.
13. Singh RK, Smith JT, Wilkinson ID, Griffiths PD. Ultrafast MR imaging in pediatric neuroradiology. Acta Radiol. 2003;44:550–557.
14. Ataxia. American College of Radiology (ACR) Appropriateness Criteria. 1999. Cited 2012. http://www.acr.org/~/media/ACR/Documents/AppCriteria/Diagnostic/Ataxia.pdf. Accessed October 5, 2012.
15. Hedlund GL, Frasier LD. Neuroimaging of abusive head trauma. Forensic Sci Med Pathol. 2009;5:280–290.
16. Gentry LR, Godersky JC, Thompson B, Dunn VD. Prospective comparative study of intermediate-field MR and CT in the evaluation of closed head trauma. AJR Am J Roentgenol. 1988;150:673–682.
17. Colbert CA, Holshouser BA, Aaen GS. Value of cerebral microhemorrhages detected with susceptibility-weighted MR imaging for prediction of long-term outcome in children with nonaccidental trauma. Radiology. 2010;256(3):989–905.
18. Schaefer PW, Grant PE, Gonzalez RG. Diffusion-weighted MR imaging of the brain. Radiology. 2000;217:331–345.
19. Cerebrovascular disease. American College of Radiology (ACR) Appropriateness Criteria. 1996. Cited 2012. http://www.acr.org/~/media/ACR/Documents/AppCriteria/Diagnostic/CerebrovascularDisease.pdf. Accessed October 5, 2012.
20. Parizel PM, Van Goethem JW, Ozsarlak O, Maes M, Phillips CD. New developments in the neuroradiological diagnosis of craniocerebral trauma. Eur Radiol. 2005;15:569–581.
21. Right lower quadrant pain—suspected appendicitis. American College of Radiology (ACR) Appropriateness Criteria. 1996. Cited 2012. http://www.acr.org/~/media/ACR/Documents/AppCriteria/Diagnostic/RightLowerQuadrantPainSuspectedAppendicitis.pdf. Accessed October 5, 2012.
22. Singh AK, Desai H, Novelline RA. Emergency MRI of acute pelvic pain: MR protocol with no oral contrast. Emerg Radiol. 2009;16:133–141.
23. Singh A, Danrad R, Hahn PF, Blake MA, Mueller PR, Novelline RA. MR imaging of the acute abdomen and pelvis: acute appendicitis and beyond. Radiographics. 2007;27:1419–1431.
24. Acute pelvic pain in the reproductive age group. American College of Radiology (ACR) Appropriateness Criteria. 2008. Cited 2012. http://www.acr.org/~/media/ACR/Documents/AppCriteria/Diagnostic/AcutePelvicPainReproductiveAgeGroup.pdf. Accessed October 5, 2012.
25. Moore MM, Gustas CN, Choudhary AK, et al. MRI for clinically suspected pediatric appendicitis: an implemented program. Pediatr Radiol. 2012;42:1056–1063.
26. Johnson AK, Filippi CG, Andrews T, et al. Ultrafast 3-T MRI in the evaluation of children with acute lower abdominal pain for the detection of appendicitis. AJR Am J Roentgenol. 2011;198:1424–1430.
27. Krishnamoorthi R, Ramarajan N, Wang NE, et al. Effectiveness of a staged US and CT protocol for the diagnosis of pediatric appendicitis: reducing radiation exposure in the age of ALARA. Radiology. 2011;259(1):231–239.
28. Bhatia NN, Chow G, Timon SJ, Watts HG. Diagnostic modalities for the evaluation of pediatric back pain: a prospective study. J Pediatr Orthop. 2008;28:230–233.
29. Kjaer P, Wedderkopp N, Korsholm L, Leboeuf-Yde C. Prevalence and tracking of back pain from childhood to adolescence. BMC Musculoskelet Disord. 2011;12:98–108.
30. Davis PJ, Williams HJ. The investigation and management of back pain in children. Arch Dis Child Educ Pract Ed. 2008;93:73–83.
31. Sorantin E, Robi T, Lindbichler F, Riccabona M. MRI of the neonatal and paediatric spine and spinal canal. Eur J Radiol. 2008;68:227–234.
32. Myelopathy. American College of Radiology (ACR) Appropriateness Criteria. 1996. Cited 2012. http://www.acr.org/~/media/ACR/Documents/AppCriteria/Diagnostic/Myelopathy.pdf. Accessed October 5, 2012.
33. Even-Sapir E. Imaging of malignant bone involvement by morphologic, scintigraphic, and hybrid modalities. J Nucl Med. 2005;46:1356–1367.
34. Gafur OA, Copley LA, Hollmig ST, Browne RH, Thornton LA, Crawford SE. The impact of the current epidemiology of pediatric musculoskeletal infection on evaluation and treatment guidelines. J Pediatr Orthop. 2008;28(7):777–785.
35. Browne LP, Mason EO, Kaplan SL, Cassady CI, Krishnamurthy R, Guillerman RP. Optimal imaging strategy for community-acquired Staphylococcus aureus musculoskeletal infections in children. Pediatr Radiol. 2008;38:841–847.
36. Chung T. Magnetic resonance imaging in acute osteomyelitis in children. Pediatr Infect Dis J. 2002;21(9):869–870.
37. Jaramillo D. Infection: musculoskeletal. Pediatr Radiol. 2011;41(suppl 1):S127–S134.
38. Mentzel HJ, Kentouche K, Sauner D, et al. Comparison of whole-body STIR-MRI and 99mTc-methylene-diphosphonate scintigraphy in children with suspected multifocal bone lesions. Eur Radiol. 2004;14:2297–2302.
39. Willinek WA, Schild HH. Clinical advantages of 3.0T MRI over 1.5 T. Eur J Radiol. 2008;65:2–14.
40. Chavhan GB, Babyn PS, Singh M, Vidarsson L, Shroff M. MR imaging at 3.0 T in children: technical differences, safety issues, and initial experience. Radiographics. 2009;29:1451–1466.
41. Smith-Bindman R, Miglioretti DL, Johnson E, et al. Use of diagnostic imaging studies and associated radiation exposure for patients enrolled in large integrated health care systems, 1996-2010. JAMA. 2012;307(22):2400–2409.
42. Thomas KE. CT utilization—trends and developments beyond the United States’ borders. Pediatr Radiol. 2011;41(suppl 2):S562–S566.