Emily C. MacNeill
HIGH-YIELD FACTS
• Hypertension is defined as blood pressures ≥90th percentile for age- and height-matched normal values. Stage 2 hypertension (≥99th percentile) requires urgent evaluation and treatment.
• The differential diagnosis of hypertension changes with the age of the patient; the clinician should focus on the cause of hypertension and evaluate the patient for signs of end-organ damage.
• Initiation of oral antihypertensive agents should be done in conjunction with the physician who will be following up with the patients.
• Patients with a hypertensive emergency should be aggressively treated and admitted to a pediatric nephrologist or other hypertension specialist.
Hypertension is an unusual finding in younger pediatric patients while becoming more common in teenagers. When present, it must be quickly recognized and treated to avoid damage to the renal, cardiovascular, and neurologic systems. In the emergency department (ED) setting, it is not common practice to routinely take blood pressures of children younger than 3 years of age. Hypertension is more common in obese teenagers and may be more like adult hypertension or be secondary to other causes. Blood pressures must be measured accurately and abnormal values confirmed before initiating an evaluation. The normal ranges for blood pressure change with age and height, and not all elevated pressures require immediate treatment. An understanding of the etiologies of and a stepwise approach to hypertensive children ensures that patients will receive appropriate management.
MEASURING BLOOD PRESSURE
Management of hypertension in children requires an accurate measurement of blood pressure. Accuracy requires a seated and relaxed patient as well as selection of the appropriate-size cuff. Cuffs that are too large will yield an erroneously low blood pressure and conversely, cuffs that are too small will yield a high reading. The bladder width should be approximately 40% of the circumference of the width of the arm at mid-point between the acromion and the olecranon process. The length of the bladder should reach around 80% to 100% of the circumference of the arm.1
Many EDs utilize automated oscillometric devices that can be very accurate at all age ranges as long as they are calibrated regularly. Any abnormal reading must be repeated by manual sphyngomanometry. In addition, abnormally high readings should be correlated with blood pressure measurements obtained from both upper extremities as well as at least one lower extremity.
DEFINING HYPERTENSION
Although there has been some debate over the years as to defining pediatric hypertension, the National High Blood Pressure Education Program (NHBPEP) put forth the following definitions of hypertension in the Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents: hypertension is either a systolic (sBP) or diastolic pressure (dBP) ≥95th percentile of age- and height-matched normal values and prehypertension is between the 90th and 95th percentile (Fig. 43-1). Hypertension is then further broken down into two stages: stage 1 hypertension is defined as sBP or dBP between the 95th and 99th percentile and stage 2 hypertension is ≥99th percentile. Because these values change with age, it can be difficult for the ED physician to recognize hypertension during the ED visit; this is unfortunate, as ensuring proper referral for these patients is vital.2Although all stages of hypertension require some further evaluation, many patients with stage 1 hypertension can be safely discharged from the ED with close follow-up. Stage 2 hypertensive patients require more urgent evaluation and treatment. This terminology differs from the vague concept of hypertensive urgency versus emergency. Hypertensive urgency describes a state of elevated pressures with potential to cause end-organ damage without any evidence of damage. Hypertensive emergency, on the other hand, is used to describe a state where end-organ damage is apparent.
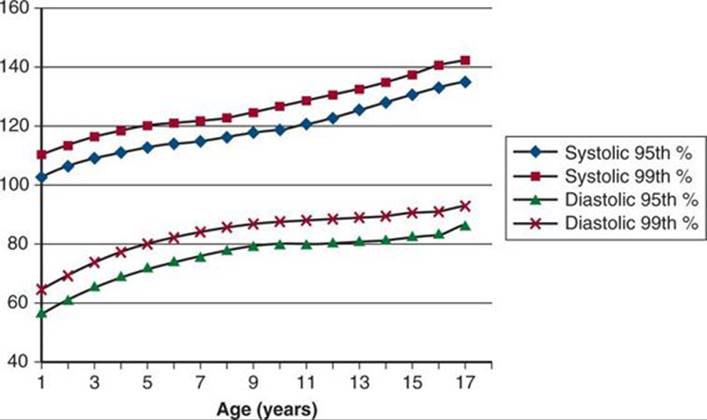
FIGURE 43-1. Hypertensive values according to age. From the Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents from 2004. Data points are taken from males at the 50th percentile for height. Females and smaller children will have slightly lower blood pressure thresholds.
Primary or essential hypertension is the most common cause of elevated blood pressure in adult populations, as secondary hypertension is a rare entity; this is not so in children. Although there appears to be a rise in pediatric hypertension linked to multiple factors—obesity, uric acid levels, dietary sodium intake, and genetics—emergency physicians must look for disease processes that can cause secondary hypertension in pediatric patients.1,3,4 This is especially true for very young children, children with stage 2 hypertension, and children with signs or symptoms of concurrent illnesses. It is important for the emergency physician to know that patients with essential hypertension often present differently than those with secondary disease. Patients with primary hypertension usually present with mild stage 1 hypertension with few, if any, symptoms. These children are usually older (adolescent age range), have a family history of hypertension or cardiovascular disease, and often have an elevated body mass index.1Although these patients will likely be discharged from the ED without treatment, it is imperative that they have close follow-up with their medical home as undertreatment of these patients leads to significant morbidity and mortality.4,5 Patients with secondary hypertension often present with stage 2 hypertension and can have more overt signs of end-organ damage: encephalopathy, seizure, congestive heart failure, chest pain, hematuria, or edema to name a few.
DIFFERENTIAL DIAGNOSIS
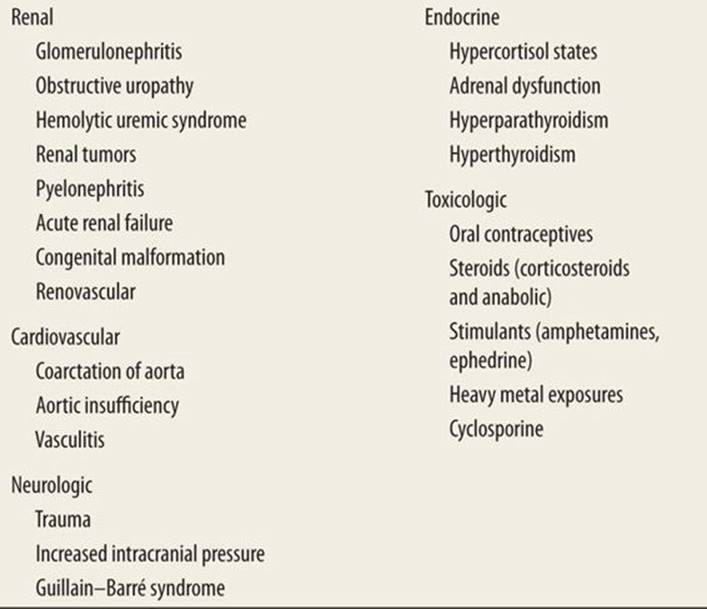
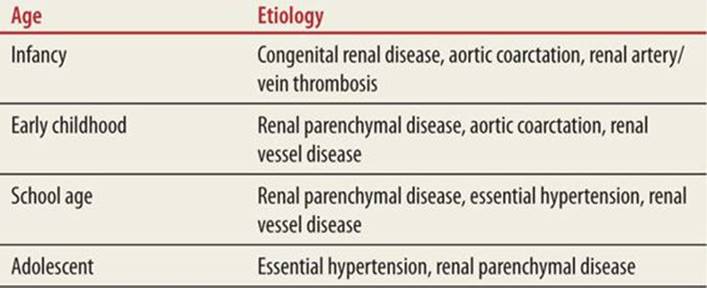
The differential diagnosis for the etiology of secondary hypertension in the pediatric patient is broad (Table 43-1). As with many pediatric diseases, the differential diagnosis for hypertension is dependent on the age of the patient. Table 43-2 demonstrates the most prominent causes of hypertension among patients of different ages. In the neonatal population, the most common causes are renal vessel thromboses/stenoses, coarctation of the aorta, and congenital renal anomalies. Renal parenchymal abnormalities are uncommon in early infancy but become the most common cause of hypertension in the school-age child. Essential hypertension is becoming more prevalent in the adolescent patient.
|
TABLE 43-1 |
Etiology of Secondary Hypertension in Children |
|
TABLE 43-2 |
Common Etiology of Hypertension in Children According to Age |
Be aware that there are numerous, less common causes, of hypertension in children. Endocrine abnormalities, such as hyperthyroidism, and hypercortisol states (from endogenous production or exogenous exposure) can be imminently dangerous. Heavy-metal poisoning is also associated with hypertension and exposure to substances such as lead should be ascertained.
ASSESSMENT
![]() HISTORY
HISTORY
Focus the history on elucidating the cause and effect (if any) of hypertension in the child. First and foremost, ascertain use of hypertensive medication as sudden withdrawal of medication can lead to pathologic increase in blood pressures. Numerous studies have demonstrated substantial usage of and safety of angiotensin-converting enzyme (ACE) inhibitors, angiotensin-receptor blockers (ARBs), and calcium-channel blockers in pediatric patients with essential hypertension. Although generally considered safe, these medicines have the same potential complications in children as they do in adults.6 A full medication history of both prescription and recreational drugs is important; oral contraceptives and steroids as well as cocaine and amphetamines can cause elevated pressures. Birth history indicating problems such as umbilical artery catheterization as well as with chronic lung disease risk factors for high blood pressure. Renal disease can be both cause and effect of elevated pressures. Thus, ask about symptoms of renal disease, specifically gross hematuria, edema, generalized fatigue, and recent infections. Endocrine problems can cause symptoms in addition to hypertension such as flushing, tachycardia and weight changes. It is especially important in the obese patient to inquire about sleep disturbance as sleep-disordered breathing is associated with hypertension.
The effects of elevated blood pressures on the pediatric patient can be quite vague. The kidneys can be profoundly affected by prolonged high pressures with few signs. Symptoms are more often recognized in the cardiovascular and neurologic systems. Chest pain, exertional dyspnea, and palpitations can occur. Ask about a history of headaches, visual disturbances, and in more severe cases, altered mental status and seizures.
![]() PHYSICAL EXAMINATION
PHYSICAL EXAMINATION
Carefully look for clues to the etiology and the effects of high blood pressure. Pay attention to the vital signs. Blood pressure measurements should be performed in both upper extremities and at least in one lower extremity. Leg pressures should measure at least 10 to 20 mm Hg higher than arm pressures and, if not, could signify coarctation of the aorta. Tachycardia can point toward an endocrine etiology, whereas bradycardia can signify increased intracranial pressure and impending herniation. After vital signs, the most important part of the physical examination is the neurologic examination, especially in the younger child, as altered mental status can be a cause or a result of pathologically elevated pressures. Fundoscopic examination should be attempted to look for elevated intracranial pressure as well as signs of long-term hypertension. Examination of the cardiovascular system includes checking pulses in all four extremities, evaluation for murmurs and gallops, as well as location of the cardiac apex.
Other physical findings can provide important clues. Adenotonsillar hypertrophy causes sleep disturbance that can lead to hypertension. Signs of heart failure should be noted, such as pulmonary edema or hepatomegaly. Edema in the lower extremities or periorbitally can indicate renal disease. Evaluate the skin for striae, flushing, acne, hirsutism, and acanthosis nigricans, all of which are signs of endocrine abnormalities. Young children should also undergo a urogenital examination to evaluate for ambiguous genitalia.
![]() TESTING
TESTING
Two things must be accomplished in the ED: the initiation of testing for the etiology and for end-organ damage and deciding whether the child requires admission or can be safely discharged with follow-up (Fig. 43-2). The results of initial screening examinations can help with this decision. An electrocardiogram, a CBC, and a basic metabolic panel as well as urinalysis and urine culture should be done on every patient with blood pressures >95th percentile prior to deciding disposition from the ED. Electrocardiogram can show left ventricular hypertrophy in the cases of prolonged or severe hypertension and can be a useful tool for deciding whether a child requires more urgent reduction in blood pressure. Electrolytes can evaluate for mineralocorticoid function and an elevated glucose, in the setting of obesity, can point toward diabetes with primary hypertension. BUN and creatinine are vital, as acute renal failure and numerous parenchymal and glomerular kidney disorders can cause hypertension. A CBC should be performed to look for signs of anemia and infection.
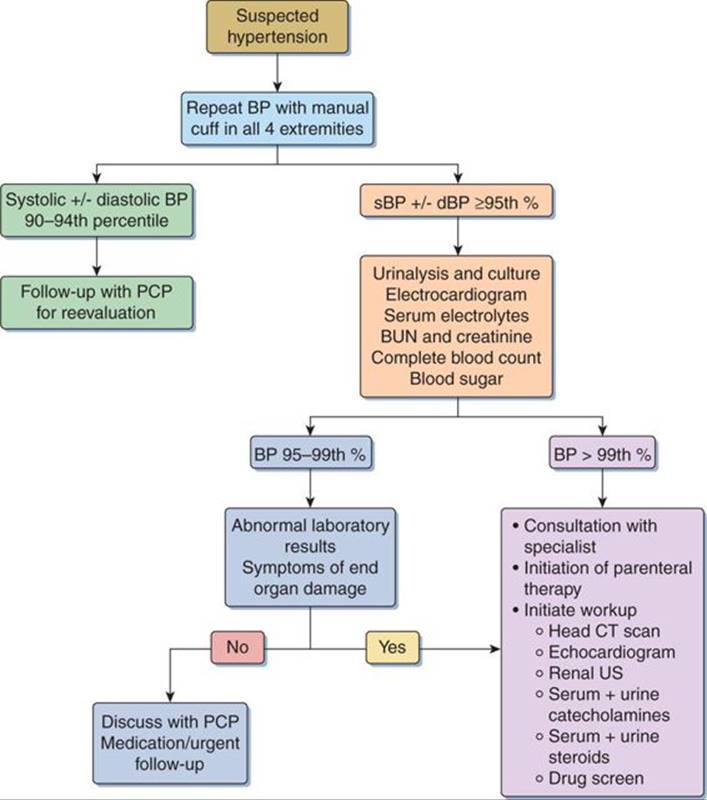
FIGURE 43-2. Algorithm for the assessment of pediatric hypertension.
If a child is admitted with hypertensive urgency or emergency, consider obtaining other tests that the child will require for the workup. These tests include rennin levels, plasma and urine steroids, plasma and urine catecholamines, drug screening, and heavy metal levels, if deemed appropriate. Clearly, if the child shows signs of neurologic dysfunction, a head CT scan is mandatory. Patients with severe hypertension will need an echocardiogram, but if the child is not in extremis and has neither critical valvular disease nor aortic coarctation, this can be completed as part of the inpatient evaluation.
TREATMENT
![]() GOALS
GOALS
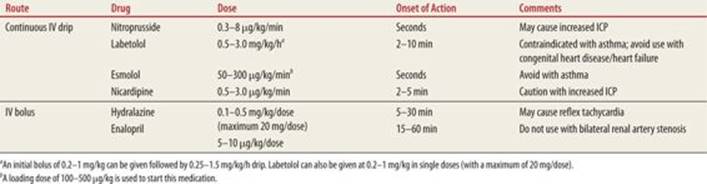
It is crucial for the ED physician to be comfortable using parenteral antihypertensive medications in the setting of hypertensive emergency. The medications used are similar to those used in adults; however, side effects and indications can be different in the pediatric patient. Thus, it is important to know not only the medications but also to be aware of doses and side effects for each drug (Table 43-3). ED physicians should also have some degree of familiarity with oral agents, including their side effects as many patients will present on these medications or they may require initiation of therapy by the ED physician in conjunction with a specialist (Table 43-4).6
|
TABLE 43-3 |
Medications Useful in Hypertensive Emergency |
|
TABLE 43-4 |
Oral Agents for the Management of Pediatric Hypertension |
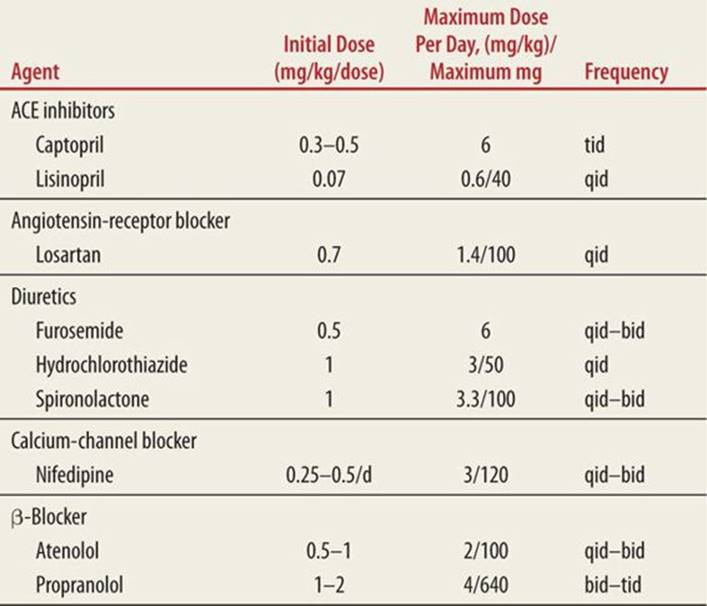
According to the Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents, parenteral medications should be reserved for patients with hypertensive emergencies. The goal of treatment should be a relatively slow reduction of pressure so as not to underperfuse vital organs. The blood pressure should decrease by 25% over the first 8 hours; medications can then be titrated to normalization of blood pressure over the next 24 to 48 hours. Children with stage 2 hypertension who have no evidence of end-organ damage may be started on oral antihypertensive agents.1
INDIVIDUAL AGENTS
![]() SODIUM NITROPRUSSIDE
SODIUM NITROPRUSSIDE
Sodium nitroprusside lowers blood pressure by dilating both the arterial and venous side of the circulation, dramatically increasing the size of the capillary beds and decreasing systemic vascular resistance. Its quick onset of action makes it a very useful drug for hypertensive emergencies. The short half-life of the drug allows for easy titration and in fact, blood pressures will return to baseline within minutes of turning off a sodium nitroprusside drip. In addition, as it does not act as a negative inotrope, it is an ideal candidate for patients with congenital heart malformations.7 The starting dose of nitroprusside is 0.3 to 0.5 μg/kg/min with a maximum of 10 μg/kg/min.8
Side effects for nitroprusside include an increase in intracranial pressure, so it should be used with caution in the setting of head injury or hypertensive encephalopathy. Also, nitroprusside is metabolized into cyanide by the red blood cells, which is then metabolized into thiocyanate by the liver and then excreted by the kidneys. Prolonged use and/or higher doses in small children can lead to cyanide poisoning. Thiocyanate levels need to be followed in prolonged administration and the drug should be discontinued after approximately 48 hours. Because of its metabolic pathway, it should be used with caution in children with renal insufficiency or liver impairment.9
![]() α- OR β-BLOCKADE
α- OR β-BLOCKADE
Labetolol has been used for many years in both adult and pediatric hypertensive crises. It acts as both an α and a β-blocker; smooth muscle relaxation peripherally allows a decrease in blood pressure with little reflex tachycardia or reduction in peripheral perfusion. Despite its efficacy, there are a few drawbacks to this drug. Its half-life is quite a bit longer than that of nitroprusside, approximately 3 to 5 hours. Thus, overshooting the desired blood pressure decrease cannot be easily reversed. It may precipitate hyperkalemia or hypoglycemia, and because of its β-blockade, it is contraindicated in children who suffer from asthma or chronic lung disease.7 It also is a negative inotrope and should probably not be used with children with congenital heart disease.8
Esmolol is a selective β-blocker that appears to be more cardioselective, and some people recommend its use in children with hypertensive crisis in the setting of congenital heart disease, especially coarctation of the aorta.7
There are drugs such as prazosin and clonidine that are selective α-inhibitors that have the benefit of not worsening bronchospasm. The main drawback with clonidine is its oral administration and a severe rebound hypertension once the drug is withdrawn.
![]() CALCIUM-CHANNEL BLOCKADE
CALCIUM-CHANNEL BLOCKADE
There are two drugs in the calcium-channel blocker class that can be used to treat hypertension in children: nicardipine and nifedipine. Nicardipine is administered intravenously and can be titrated carefully with its rapid onset of action and short half-life. Also, because it has some cardiac activity, it can decrease the systemic vascular resistance (SVR) without causing an increase in heart rate.7 There is little published data on the use of this drug in children but case reports have been published especially for those in whom other agents are contraindicated. Nifedipine is an oral agent available in liquid-filled capsules and is not used often in acute settings. The capsule can be opened and administered sublingually as a last resort for children with hypertensive emergency, when IV access is an issue. This agent should be used with great caution as it can be difficult to dose and can cause excessive drop in blood pressure.10 Also, it has a short half-life with potential for rebound hypertension.8 Its use is better restricted to long-term management of hypertension in its extended release form.
![]() ACE INHIBITORS
ACE INHIBITORS
This class of drugs inhibits ACE that converts renin to angiotensin. Angiotensin is a potent vasoconstrictor, so the result of inhibiting ACE is vascular relaxation and decrease in blood pressure. There are many oral forms that have been studied and are both efficacious and safe in pediatric populations. There is also an intravenous version of enalopril (enaloprilat) that can theoretically be used for pediatric hypertensive emergency, although it is found to be most effective with children who have high renin states.9
![]() HYDRALAZINE
HYDRALAZINE
Hydralazine is a drug that has, in the past, been given for rapid lowering of blood pressure; this is accomplished by pure arteriolar dilatation. It appears to be no more effective than sodium nitroprusside, can have a less predictable effect on blood pressure, and can also cause significant tachycardia.9 At this time, there are numerous superior choices to hydralazine for blood pressure lowering, however it may be useful as an oral agent while IV agents are being prepared.7
![]() DIURETICS
DIURETICS
Diuretics work by decreasing intra- and extravascular volumes. Unfortunately, the body becomes accustomed to this effect, leading to medication resistance. The most commonly used agents are loop diuretics, thiazides, and potassium-sparing diuretics, and all are safe to use initially. Side effects of these medications are mainly electrolyte imbalances that should be evaluated in patients who take them for prolonged periods of time. Both loop diuretics and thiazides can cause hypokalemia and hyperlipidemia; loop diuretics also cause hypercalcemia and thiazides can cause calciuria.9
SUMMARY
As the incidence of hypertension in the pediatric population is increasing, it is vital that the emergency physicians recognize and treat pathologically elevated pressures. This requires knowledge of the normal blood pressures in children and the differential diagnosis of hypertension appropriate for that patient’s age group. Although definitive diagnosis and treatment of hypertension often does not occur in the ED, the responsibility of initial screening for both life-threatening causes (such as aortic coarctation) and end-organ damage lies with the emergency physician. Patients can then be routed to the appropriate specialist as an inpatient or with an outpatient referral for long-term management. The emergency medicine physician should be familiar with and comfortable with the treatment of hypertensive emergency.
REFERENCES
1. National High Blood Pressure Education Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114:555–576.
2. Ricke TL, Hendry PL, Kalynych C, et al. Incidence and recognition of elevated triage blood pressure in the pediatric emergency department. Pediatr Emerg Care. 2011;27(10):922–927.
3. Chiolero A, Bovet P, Paradis G, et al. Has blood pressure increased in children in response to the obesity epidemic. Pediatrics. 2007;119(3):544–553.
4. Feber J, Ahmed M. Hypertension in children: new trends and challenges. Clin Sci. 2010;119:151–161.
5. Hansen ML, Gunn PW, Kaelber DC. Underdiagnosis of hypertension in children and adolescents. JAMA. 2007;298(8):874–879.
6. Meyers RS, Siu A. Pharmacotherapy review of chronic pediatric hypertension. Clin Ther. 2011;33(10):1331–1353.
7. Thomas CA. Drug treatment of hypertensive crisis in children. Pediatr Drugs. 2011;13(5):281–290.
8. Constantine E, Linakis J. The assessment and management of hypertensive emergencies and urgencies in children. Pediatr Emerg Care. 2005;21(6):391–396.
9. Temple ME, Nahate MC. Treatment of pediatric hypertension. Pharmacotherapy. 2000;20(2):140–150.
10. Adelman RD, Coppo R, Dillon MJ. The emergency management of severe hypertension. Pediatr Nephrol. 2000;14:422–427.