Heather B. Conrad
P. Jamil Madati
HIGH-YIELD FACTS
• Staphylococcus and Streptococcus are, by far, the most common bacteriological etiologic agents of most superficial skin infections.
• The marked increase in prevalence of CA-MRSA has made it necessary to consider using an antibiotic that targets this resistant organism (clindamycin or trimethoprim/sulfamethoxazole) when using an oral agent to treat severe, recurrent, or disseminated infections.
• Poststreptococcal glomerulonephritis is caused by nephritogenic strains of streptococci which can cause skin infections and pharyngitis. It presents a couple of weeks after the primary infection.
• Tinea corporis can be treated effectively with topical antifungals, but tinea capitis requires long courses (4–8 weeks) of systemic antifungal therapy.
IMPETIGO
![]() ETIOLOGY
ETIOLOGY
Impetigo is a common childhood superficial skin infection seen in preschool and school-aged children that is classically caused by Staphylococcus aureus bacteria but can also be caused by Group A Streptococcus species (Streptococcus pyogenes) which usually peaks in incidence during the summer and fall seasons.1 Given the steady increase in the prevalence of Community Acquired Methicillin Resistant S. aureus (CA-MRSA) over the past two decades, including reports of 40% to 70% prevalence in some areas, antibiotic selection must take into account this prevailing resistance pattern within the community.2–4
![]() PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
Impetigo infections occur when bacteria, that is usually present on the surface of the skin, enters into the epidermal layer through areas of skin breaks or microabrasions or at sites of skin trauma. The bacteria then replicates beneath the skin causing the characteristic crusted “honey colored” gold lesions. Transmission of infection occurs through direct contact or fomites.1
![]() RECOGNITION
RECOGNITION
The classic impetigo rash begins with erythematous macular or papular lesions that then progress to superficial vesicles or bullae which then rupture leaving crusted “honey colored” gold lesions. Lesions can be solitary, arranged in clusters, or confluent. Typical distribution include the face, extremities, and/or distal fingers or toes for nonbullous impetigo and intertriginous areas of the neck, diaper area, or axillae for bullous impetigo.1,4
![]() MANAGEMENT
MANAGEMENT
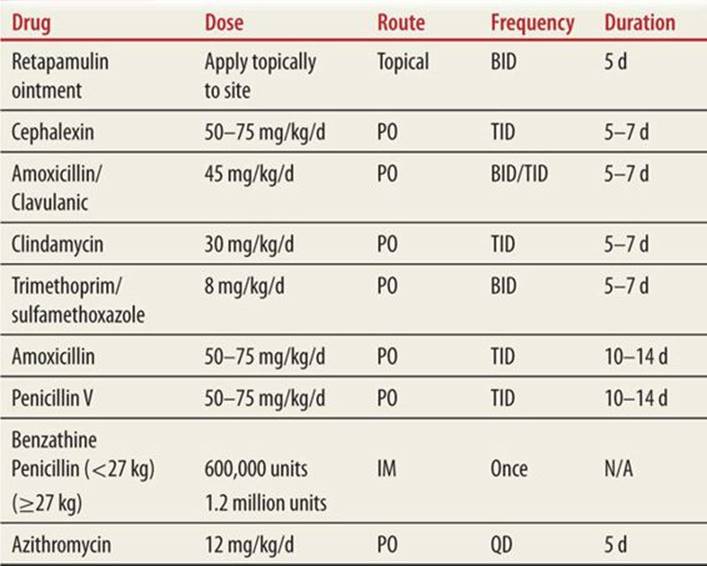
Reports indicate that in 15% to 50% of cases, impetigo is a benign self-limited disease lasting 2 to 3 weeks. However, it is easily transmitted to others and some studies report a 5% chance of Group A Strep impetigo leading to acute glomerulonephritis.1,4 Maintaining good skin hygiene, using antibacterial soaps, and/or dilute bleach baths have shown varying degrees of success in eradicating colonization. Over-the-counter topical agents such as bacitracin or neomycin tend to be ineffective due to the emergence of MRSA. Mupirocin or fusidic acid (not approved in the United States) ointments have been the mainstay of topical treatment for impetigo and, in a recent Cochrane review, has evidence of being the most effective treatment.5 Due to reported resistance to mupirocin, a newer agent that has shown promise for the treatment of resistant impetigo is retapamulin (apply ointment topically to the site BID for 5 days).4 Oral antibiotics should be reserved for treatment of moderate/severe cases or refractory cases of impetigo. Oral agents that are effective include cephalosporins and beta lactamase resistant penicillins such as amoxicillin/clavulanic acid. In communities with a high incidence of MRSA, treatment with clindamycin or Trimethoprim/sulfamethoxazole should be initiated to target this specific bacterial etiology.4,6 Please refer to Table 90-1 for specific dosing and duration of therapy.
|
TABLE 90-1 |
Antibiotic Regimens for Soft-Tissue Infections6 |
![]() ANCILLARY STUDIES
ANCILLARY STUDIES
A wound culture from crusted lesions or from the nasopharynx may grow Group A Streptococcus or Staphylococcus which can sometimes help guide treatment choices for recurrent or refractory cases of impetigo.
CELLULITIS/ERYSIPELAS
![]() ETIOLOGY
ETIOLOGY
Cellulitis is an infection of the subcutaneous tissue caused by bacteria that results in warm, tender, and erythematous skin at the site of bacterial inoculation. Typical bacterial etiologic agents include Haemophilus influenza, Group A Streptococci, and S. aureus.
![]() PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
Bacteria enter the dermal and subcutaneous tissues of the skin through small breaks in the patient’s skin. Increased redness, warmth, swelling, and tenderness ensues 1 to 3 days after inoculation.1 The resultant infection can progress into deeper tissues, leading to bacteremia and the onset of systemic symptoms such as fever, chills, and malaise.
Erysipelas is a dermal infection typically caused by Group A Streptococci but can also be caused by S. aureus, Pneumococcus, K. pneumoniae, Yersinia enterolitica, or H. influenzae. The bacteria enters the dermis through breaks in the skin or from the pharynx leading to a well-demarcated erythematous, hot and tender plaque on the face, cheeks, bridge of nose, or lower extremities. Histopathology of the lesions show marked swelling within the dermis with neutrophilic infiltrate.1
![]() RECOGNITION
RECOGNITION
Cellulitis and erysipelas are characterized by an area of skin with marked erythema, warmth, and sometimes tenderness and swelling. The area could also have lymphatic streaking associated with it. Regional lymph nodes maybe enlarged and in the case of severe or deep tissue infections, there can also be associated fever and malaise. Typical locations for cellulitis are the extremities, face, neck, or other sites of trauma or injury. Erysipelas is classically located on the face.
![]() MANAGEMENT
MANAGEMENT
An outpatient course of oral antibiotics remain the mainstay of treating mild or moderate cellulitis infections. Choice of antibiotics should include agents with good gram-positive coverage such as cephalosporins, amoxicillin/clavulanic. If there is a concern for MRSA, clindamycin or TMP/SMX may be considered.6 Erysipelas can be treated with penicillin or amoxicillin. Refer to Table 90-1 for specific dosing and duration of therapy. For patients exhibiting systemic symptoms, refractory cases, or for infections involving the eye, inpatient hospitalization with initiation of intravenous (IV) antibiotics (cephalosporin, clindamycin, or vancomycin if MRSA is suspected) is indicated.6,7
![]() ANCILLARY STUDIES
ANCILLARY STUDIES
For mild cases, no ancillary studies are necessary. For moderate or severe cases, particularly if patient is exhibiting systemic symptoms, a CBC, sedimentation rate, and/or C-reactive protein could help in assessing the severity of the illness as well as trending to see if there is resolution of these inflammatory markers with treatment. Blood cultures in patients with systemic symptoms can help guide appropriate antimicrobial therapy. Skin cultures by needle aspiration or skin biopsy at the leading edge may also recover the inciting organism to further help guide treatment.1
FOLLICULITIS, FURUNCLES, AND CARBUNCLES
![]() ETIOLOGY
ETIOLOGY
Folliculitis is an infection of the tissues surrounding the hair follicles. This infection occurs on wet, occluded, or macerated skin. The common offending bacterial agents are usually Staphylococcus or Pseudomonas.
Furuncles are deep red, hot, and tender, perifollicular purulent inflammatory nodules that usually result from a worsening folliculitis. Carbuncles are larger lesions of coalesced furuncles.1Furuncles/Carbuncles are commonly caused by Staphylococcus except in the anogenital region where the anaerobic bacteria are the predominant etiologic agent.
![]() PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
Folliculitis and furuncles are commonly found in areas of the skin that are moist, hot or humid, or areas of the skin where there is poor hygiene or constant friction. These areas include the axilla, groin, buttocks, neck, waist/belt line, and face. Lesions start out as inflammation around the base of the follicle (folliculitis) but with constant friction or trauma (shaving, waxing, etc.) in the setting of warm, moist conditions, progress to tender pus-filled subcutaneous nodules.
![]() RECOGNITION
RECOGNITION
Folliculitis lesions are pink or red papular lesions in the above distribution that are usually non tender but sometimes pruritic. Furuncles and carbuncles are larger, nodular, erythematous and tender lesions that sometimes have associated purulent discharge.
![]() MANAGEMENT
MANAGEMENT
Treatment for folliculitis involves removal of occlusive dressings and avoiding activities that result in continual trauma or irritation to the area such as shaving or waxing. Topical antibiotic ointments such as bacitracin or mupirocin as well as cleansing the area with antibacterial soaps or washes (benzoyl peroxide or chlorhexidine) have been used with varying degrees of success. Early or small furuncles and carbuncles can usually be treated with warm compresses. Fluctuant or deep lesions may require incision and drainage to relieve the infection. Oral antibiotics are reserved for those lesions that exhibit a cellulitic component, those patients who exhibit systemic symptoms or those patients with recurrent or persistent lesions. Antibiotic choices include cephalosporins or in the setting of MRSA, the use of TMP/SMX or clindamycin is recommended.1,2,6
![]() ANCILLARY STUDIES
ANCILLARY STUDIES
Usually, no further studies are needed. Cultures of purulent drainage from furuncles or carbuncles can be sent to help guide antibiotic therapy for persistent or recurrent cases.
SCARLET FEVER AND PERIANAL STREP
![]() ETIOLOGY
ETIOLOGY
Group A Streptococcus, and to a lesser extent S. aureus, are the bacteria most commonly associated with the characteristic exanthem seen with scarlet fever.8 The scarlet fever rash, also known as scarlatina, is usually seen in children 1 to 10 years of age and is a toxin mediated rash that usually starts on the torso and spreads to the extremities. In contrast, the rash seen in perianal strep, which is also caused by Group A Streptococci, is not toxin mediated.
![]() PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
The toxin mediated rash of scarlet fever tends to appear several days after the onset of tonsillitis.
![]() RECOGNITION
RECOGNITION
Scarlet fever initially starts as a punctate “sand-paper” rash that progresses to confluent erythematous patches spreading from the torso to extremities. The rash is characteristically accentuated on the pressure points or body folds. By day 4 or 5 of illness, the rash begins to fade and results in desquamation of the skin on the body and extremities. Systemic symptoms include fever, malaise, pharyngitis, headache, and vomiting.1
The typical rash seen with perianal strep is a well-demarcated red perianal rash that is pruritic, itchy, and sometimes painful in a child that is typically younger than 4 years old.
![]() MANAGEMENT
MANAGEMENT
Recommended treatment in both cases involves a 10- to 14-day course of oral antibiotics penicillin or amoxicillin, or in penicillin-allergic patients a macrolide, such as azithromycin, can be used.6
![]() ANCILLARY STUDIES
ANCILLARY STUDIES
Pharyngeal swab or perianal skin culture can grow the offending organism. For patients suspected of having scarlet fever, in addition to nasal or pharyngeal swabs, the evaluation can include blood cultures, ASO titers, in order to make a definitive diagnosis of a Streptococcus infection.1
INSECT BITES: PEDICULOSIS, SCABIES, BED BUGS
![]() PEDICULOSIS
PEDICULOSIS
Etiology Pediculosis is a superficial infestation caused by lice. The three types of lice that contribute to human disease are Pediculus humanus capitis (head louse) (Fig. 90-1), Pediculus humanus corporis(body louse) (Fig. 90-2), and Pthirus pubis (pubic or crab louse) (Fig. 90-3). The head louse is, by far, the most common louse infection seen in children. The prevalence of head lice is about 10% in school children with 6 to 11 year olds the most affected age group.9 Females are preferentially affected which is thought to be due to their longer hair and greater sharing of fomites.9 Contrary to popular belief, head lice can also be found in children with proper hygiene.9,10

FIGURE 90-1. Adult female human head louse (Pediculus capitis) on a nit (louse egg) comb.

FIGURE 90-2. Pediculosis humanus corporis, the body louse.

FIGURE 90-3. Pediculosis Phthirus pubis, the crab louse.
Pathophysiology Lice are bloodsucking obligate parasites of humans. They attach their eggs (nits) firmly to hair shafts of their hosts, close to the skin (Fig. 90-4). They are transmitted by direct human contact or the sharing of clothing or other personal articles. Lice require a hair-bearing surface to survive, with the adult viable for only 2 days and the nit for 10 days off of the host. The female may lay up to 300 nits (eggs) which will hatch in 6 to 10 days and assume the adult form 10 days after hatching. Itching is the most common patient complaint but local erythema or papules at the site of infection is sometimes reported.10

FIGURE 90-4. Pediculosis capitis: multiple nits on scalp hair. Myriads of nits (oval, grayish-white egg capsules) are firmly attached to the hair shafts, visualized with a lens. On close examination, these have a bottle shape.
Recognition The diagnosis of a head lice infestation is made by checking the patient’s scalp for nits and live lice. A confirmation of the diagnosis is made only when live lice are found. The scalp may be examined by combing through the hair with a fine toothed comb (louse comb) looking for live lice. Most of the eggs are laid at the nape of the neck or behind the ears, so the clinician should inspect these areas with particular attention. Eggs may remain after the larvae have hatched therefore the detection of nits alone does not confirm an infestation.10
Management When the diagnosis of head lice is made, a concerted effort to decontaminate the environment is recommended. Furniture needs to be vacuumed and clothing dried at >60°C. Clothing and fomites that cannot be dried should be placed in a bag for at least 3 days and possibly 13 to prevent hatching of nits.9 Boiling of hairbrushes will kill the lice and nits.9 An adjunctive treatment to chemical agents is wet-combing of hair with a fine-toothed comb every 3 to 4 days to remove live lice as they hatch.10 It is recommended that all close the contacts of the affected individual be treated as well to increase cure rates. Permethrin supplied as a 1% cream rinse is a more potent pediculocidal agent than natural pyrethrins and has a residual activity of 2 weeks. Cure rates are increased if reapplied a week after the initial application. It is applied to the scalp on shampooed hair and washed off after 10 minutes. The patient may experience burning, tingling, numbness, and erythema after application. There are reports of increasing resistance to permethrin.11 Recently a new pediculocidal medication spinosad (Natroba) topical suspension 0.9% has been approved by the Federal Drug Administration for the treatment of lice.9This medication is often effective with one dose and unlike permethrin, parents do not have to comb for nit removal.9 Spinosad can cause benzyl alcohol toxicity and is not recommended for patients younger than 6 months of age.9 Lindane is a topical ovicidal agent that has been encountering resistance and is therefore no longer recommended for treatment in children due to potential neurotoxicity.9 Malathion has been used to treat lice infestations as well but because of its flammability, bad odor, and 8 to 12 hours application time, it is not as popular as other options.11
Ancillary Studies Typically, no ancillary studies are necessary to diagnose pediculosis.
![]() SCABIES
SCABIES
Etiology Sarcoptes scabiei (scabies) are human mites which cause superficial skin infestation. There are an estimated 300 million infected individual worldwide with no predilection for age, gender, or socioeconomic class.10
Pathophysiology Scabies are primarily transmitted by direct close and prolonged human contact but can also be spread by fomites. Human scabies may survive for 24 to 36 hours off of a host.9 Although it only takes a mite 30 minutes to create a burrow, patients are often not symptomatic until 4 to 6 weeks after infestation because of a delayed immune response.9,10 Scabies can cause secondary skin infection, sepsis, or even glomerulonephritis.10
Recognition Symptoms of scabies infection include pruritis, which is worse at night, infants will often sleep poorly, rubbing their hands and feet together because of the itching. Small red, raised, papules are formed which may progress to vesicles and pustules. Secondary excoriations are also commonly present. There are three forms of scabies—classical, crusted, and nodular. Classical scabies is the most common and reflects a lower mite burden while crusted scabies generally reflects a higher mite burden and is often seen in the immunocompromised and mentally/physically handicapped.9 Classic scabies presents as a rash in the interdigital web spaces, in the genital region, or around the nipples.10 The burrow made by the female mite is the pathognomonic sign of scabies.10 Nodular scabies is the least common and appear as red/brown nodules representing a hypersensitivity reaction to the mites and their byproducts.9 The diagnosis of scabies is made clinically. One may also scrape burrows or papules overlaid with mineral oil and inspect the scraping for adults, eggs, and excreta for confirmation (Fig. 90-5). Of note, scabies in infants and very young children may not be seen in the classic skin areas and instead are seen as vesicles, papules, and pustules in the hands, feet, body folds, the head, and behind the ears.10
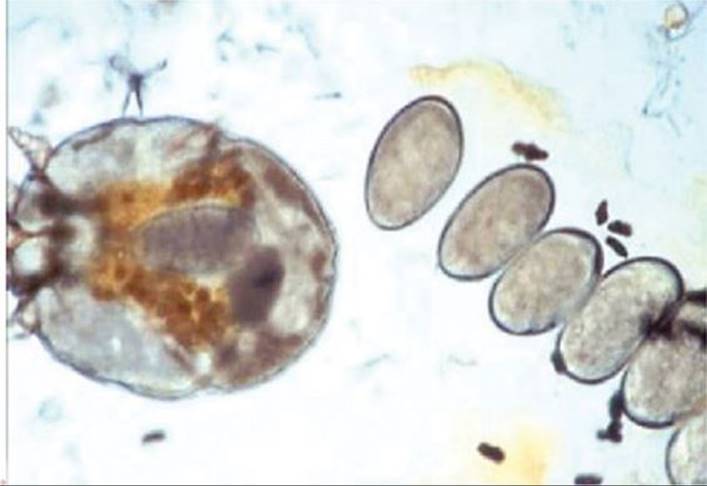
FIGURE 90-5. Scabies. Microscopic examination of a mineral oil preparation after scraping a burrow reveals a gravid female mite with oval, gray eggs and fecal pellets
Management A single application of 5% permethrin cream is curative for children older than 2 months. The cream may be applied to the face and scalp and needs to be left for 8 hours. Permethrin has been found to have a 97.8% cure rate with one application.9 Permethrin may cause burning and stinging as well as exacerbation of itching although it is generally very well tolerated and has low potential for toxicity.10 Younger children may be treated with sulfur precipitated in petrolatum.9 The long incubation period makes treating the entire family advisable. Because the parasite lives for only 24 to 36 hours off the host, environmental decontamination may not be necessary; however, it is recommended that fomites be dried at 60°C for 10 minutes and surfaces such as furniture should be vacuumed.9
Ancillary Studies A clinical diagnosis of scabies should be confirmed by obtaining a skin sample demonstrating the presence of the mite, its eggs, or feces in skin samples. To find the mite, one may either use a scalpel or sterile needle to remove the mite from its burrow or perform skin scrapings. It is preferable to use mineral oil or saline to visualize evidence of a scabies infection. 11
![]() BED BUGS
BED BUGS
Etiology Cimex lecularius is the blood-feeding insect parasite that causes the symptoms associated with bed bugs. The adult is flat and reddish brown and can be visualized without a microscope. Bed bugs have recently emerged as a problem in developed countries in part due to increased travel and insecticide resistance. They rely on the human host for survival.9,12
Pathophysiology Bed bugs preferentially feed on the blood of their human hosts at night. They are not known to transmit disease such as HIV and hepatitis. Patients usually present with an allergic reaction to the bites which are usually clustered in small areas of exposed skin. The skin reactions are varied and may appear as anything from macules to indurated bullous lesions.9
Recognition A bed bug infestation is usually discovered when a patient presents with pruritis and bug bites with an unknown etiology. Confirmation of an infestation occurs when one sees the insect and/or their fecal specks in the seams of the mattress or box spring. Blood spots may also be found on the mattress.9,12
Management Treatment of bed bug bites is largely symptomatic with antihistamines and glucocorticoids treating pruritis; however, secondary infections should be treated with systemic oral antibiotics. To eradicate bed bugs, a professional exterminator should be utilized and the environment should be vacuumed and clothing/bedding dried at a high temperature.9,12
Ancillary Studies No ancillary studies are typically necessary to diagnose bed bug’s infections.
TINEA CAPITIS, TINEA CORPORIS, TINEA PEDIS, AND TINEA UNGUIUM
![]() ETIOLOGY
ETIOLOGY
Tinea is a dermatophytic infection caused by fungi that infect the keratinous layers of the skin. Tinea infections are usually classified based on their anatomical location: Tinea capitis is found on the scalp, tinea corporis on the body, tinea pedis on the feet, and tinea unguium on the nails.13
![]() PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
Three dermatophyte genera generally cause tinea infections and they are Trichophyton, Mircrosporum, and Epidermophyton. This chapter will focus on the most common infections found in children: tinea capitis and tinea corporis. Tinea capitis is caused by Trichophyton tonsurans in more than 90% of children while Microsporum species account for less than 5%.13 Superficial tinea infections are generally spread by direct person to person contact.14
![]() RECOGNITION
RECOGNITION
Tinea capitis will affect both the skin and hair shafts. Patients may present with localized scaling and hair loss as well as broken hair in the affected area. The differential diagnosis of tinea capitis includes alopecia, trichotillomania, alopecia areata, and traction alopecia. Tinea corporis is also called ringworm and is caused by Trichophyton species. It is seen as an annular patch or plaque with a raised, erythematous scaling border with central clearing.13
MANAGEMENT
Treatment of tinea capitis needs to be with oral medication because of hair shaft involvement. Griseofulvin is historically the treatment of choice but terbinafine has been found to be as effective and has a shorter duration of treatment, 4 to 6 weeks as opposed to 6 to 8 weeks.14,15 Griseofulvin is the first line of therapy. Baseline liver function tests need not be drawn but if treatment goes over 8 weeks it is recommended to check a complete blood count, liver function tests with bilirubin, and a blood urea nitrogen and creatinine.14 The dose for microsize griseofulvin 20 mg/kg/d and for ultramicrosize griseofulvin is 10 to 15 mg/kg/d as a once-daily dosing secondary to resistance of T. tonsurans to the drug.15 Once a day oral terbinafine, is approved for patients over 4 years of age with dosing recommendations of 125 mg granules for patients <25 kg, 187.5 mg for patients 25 to 35 kg, or 250 mg for patients weighing 35 kg or above.14,15 Before starting terbinafine liver function tests need to be drawn and a complete blood count should be checked if treatment is for more than 6 weeks.14
Tinea corporis is treated with topical antifungals. Antifungal agents should be applied to an area 2 cm outside of the lesion for 1 week after clearance of the lesion.14 Newer fungicidal medications such as butenafine and terbinafine are more effective than fungistatic medications such as miconazole and clotrimazole.14
![]() ANCILLARY STUDIES
ANCILLARY STUDIES
Patients are diagnosed clinically but potassium hydroxide (KOH) microscopy of skin scraping and hair shafts may be helpful if the diagnosis is in question.13,14 Historically, the Wood lamp had been used to diagnose tinea capitis and pityriasis versicolor. However, the changing epidemiology of tinea capitis in the United States has made the use of the Wood lamp less beneficial as Trichophyton does not fluoresce.14
PITYRIASIS VERSICOLOR
![]() ETIOLOGY
ETIOLOGY
Pityriasis versicolor, formerly known as tinea versicolor, is a superficial fungal infection caused by the yeast form of Malassezia.14
![]() PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
Pityriasis versicolor is a superficial skin infection where the organism develops filaments and damages the stratum corneum. The stratum corneum is damaged by tissue invasion, dyspigmentation, and inflammation. Earlier, it was believed that Malassezia furfur was the causative agent however molecular studies are now implicating Malassezia globus.16
![]() RECOGNITION
RECOGNITION
An infection may be seen as multiple oval hypo- or hyper-pigmented scaling lesions on the trunk and arms. Often, a herald patch may be seen before the rest of the lesions. The infection becomes most noticeable in the temperate months as the patient becomes tan and the affected lesions remain without pigmentation. Unlike other superficial tinea infections, pityriasis versicolor may be seen yellow/green with a Wood lamp. A KOH prep confirms the diagnosis when the classic “spaghetti and meatballs” appearance of hyphae and spores are seen.14
![]() MANAGEMENT
MANAGEMENT
Selenium sulfide 2.5% shampoo applied on the skin for 10 minutes for 1 to 2 weeks is usually effective for treatment.14
![]() ANCILLARY STUDIES
ANCILLARY STUDIES
A Wood lamp can help in diagnosis of pityriasis versicolor as it will fluoresce a pale yellow. A KOH preparation is confirmatory and will show hyphae and clusters of spores typically described as “spaghetti and meatballs.”14
REFERENCES
1. Kane KS, Lio PA, Stratigos AJ, Johnson RA. Color Atlas & Synopsis of Pediatric Dermatology. 2nd ed. New York, NY: McGraw-Hill Companes Inc; 2009.
2. Moran GJ, Krishnadasan A, Gorwitz RJ, et al. Methicillin-resistant S. aureus infections among patients in the emergency department N Engl J Med. 2006;355(7):666–674.
3. Johnson JK, Khoie T, Shurland S, Kreisel K, Stine OC, Roghmann MC. Skin and soft tissue infections caused by methicillin-resistant Staphylococcus aureus USA300 clone. Emerg Infect Dis. 2007;13(8):1195–1200.
4. Bangert S, Levy M, Hebert AA. Bacterial resistance and impetigo treatment trends: a review. Pediatr Dermatol. 2012;29(3):243–248.
5. Koning S, van der Sande R, Verhagen AP, et al. Interventions for impetigo. Cochrane Database Syst Rev. 2012;1:CD003261.
6. Bradley JS, Nelson JD. Nelson’s Pediatric Antimicrobial Therapy. 19th ed. American Academy of Pediatrics; 2012–2013.
7. Kilburn SA, Featherstone P, Higgins B, Brindle R. Interventions for cellulitis and erysipelas. Cochrane Database Syst Rev. 2010;(6):CD004299.
8. Heath C, Desai N, Silverberg NB. Recent microbiological shifts in perianal bacterial dermatitis: Staphylococcus aureus predominance. Pediatr Dermatol. 2009;26(6):696–700.
9. Shmidt E, Levitt J. Dermatologic infestations. Int J Dermatol. 2012;51(2):131–141.
10. Orion E, Marcos B, Davidovici B, Wolf R. Itch and scratch: scabies and pediculosis. Clin Dermatol. 2006;24(3):168–175.
11. Orion E, Matz H, Wolf R. Ectoparasitic sexually transmitted diseases: scabies and pediculosis. Clin Dermatol. 2004;22(6):513–519.
12. Goddard J, de Shazo R. Bed bugs (Cimex lectularius) and clinical consequences of their bites. Jama. 2009;301(13):1358–1366.
13. Andrews MD, Burns M. Common tinea infections in children. Am Fam Physician. 2008;77(10):1415–1420.
14. Kelly BP. Superficial fungal infections. Pediatr Rev. 2012;33(4):e22–e37.
15. Pickering LK, Baker CJ, Kimberlin DW, Long SS. Red Book: Report of the Committee on Infectious Diseases. 29th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2012.
16. Hay RJ. Malassezia, dandruff and seborrhoeic dermatitis: an overview. Br J Dermatol. 2011;165(Suppl 2):2–8.