Approach to the Problem
Physicians caring for children frequently see patients who have complaints about the ear, including pain, itching, drainage, and decreased hearing. Often, the initial concern is focused on middle ear abnormalities, but external auditory canal (EAC) abnormalities may cause complaints that are similar to those caused by middle ear pathology. Common diseases of the EAC include otitis externa (affecting up to 10% of the population), impacted cerumen, trauma, and foreign bodies in the ear.
There are many variations in cerumen, and canal size and shape. Flaky, dry cerumen may be found in East Asian patients. In some cases, as in Down syndrome, the canals may be narrowed, making it difficult for the examiner to evaluate the tympanic membrane on routine otoscopy.
Key Points in the History
• School-aged children may be exceptionally precise in their description of pain. Therefore, it is important to ask them to describe what they are feeling. Often, when parents report pain, the child instead reports ringing or fullness. For example, one child with water in his ear reported, “It sounds like I am under water.”
• The use of cotton swabs or other objects to clean the ear may result in trauma to the EAC and tympanic membrane, and retained pieces of cotton may cause irritation and/or subsequent inflammation.
• The placement of a foreign body in the ear may lead to trauma and most often presents with pain. If the foreign body is not promptly removed, the EAC may become infected.
• Tinnitus and bleeding, in addition to pain, may be symptoms that occur from trauma to the external ear canal.
• Decreased hearing often occurs with cerumen impaction, fluid in the external canal, or otitis externa, but it may also be seen in trauma, particularly when perforation of the tympanic membrane exists.
• Drainage from the EAC may occur in acute otitis media with perforation, otitis externa, and external fluid in the canal (residual from swimming or bathing).
• The drainage seen with acute otitis media with perforation is often described as brownish and sticky, but at other times may be whitish and creamy.
• Pseudomonal and fungal infections should be considered in children with chronic symptoms of otitis externa.
• History of frequent swimming or submersion of ears while in the bathtub is suggestive of otitis externa (also known as swimmer’s ear). Water from the pool or tub is believed to cause alterations in the normal flora of the EAC.
• Patients with eczema, seborrhea, or psoriasis may have the involvement of the epidermis of the EAC and may complain of pruritus.
• The use of medication or topical substances to the ear may result in an eczematous dermatitis.
• Earrings, particularly those made of alloy metals, may cause inflammation at the earring site and an eczematous dermatitis of the surrounding tissues.
• Pain preceding development of a vesicular rash suggests varicella zoster virus infection, which when associated with an acute facial neuropathy is known as Ramsay Hunt syndrome.
Key Points in the Physical Examination
• It is important to note that there may be variations in the amount, color, and consistency of cerumen.
• If blood is present, suspect trauma and carefully inspect the tympanic membrane for perforation or other injury.
• Pain elicited from pressure on the tragus and/or outward traction on the pinna is suggestive of otitis externa.
• Edema and inflammation of the ear canal are typically seen with otitis externa.
• When a significant amount of discharge is present, it may be difficult to differentiate acute otitis media with perforation from otitis externa.
• Greasy scales, dry or flaky skin, excoriation, and crusting of the external ear canal and pinna may be seen with eczematous or psoriatic dermatitis and seborrhea.
• Pustules on the outer portion of the EAC suggest furunculosis.
• Vesicular lesions suggest reactivation of varicella zoster or herpes simplex virus.
|
PHOTOGRAPHS OF SELECTED DIAGNOSES |
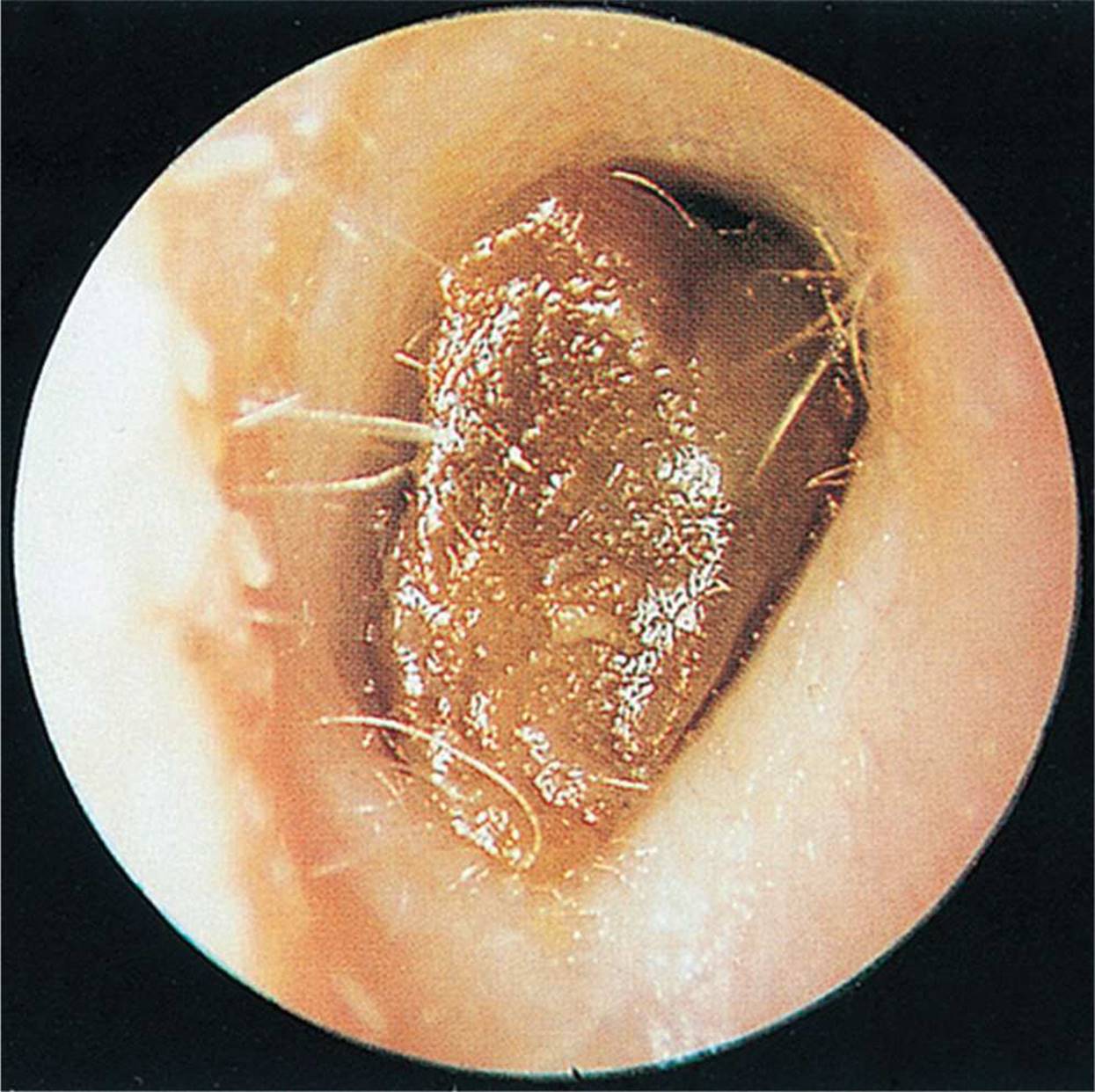
Figure 20-1 Cerumen impaction of the ear canal. (From Weber JR. Nurses’ Handbook of Health Assessment. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009.)
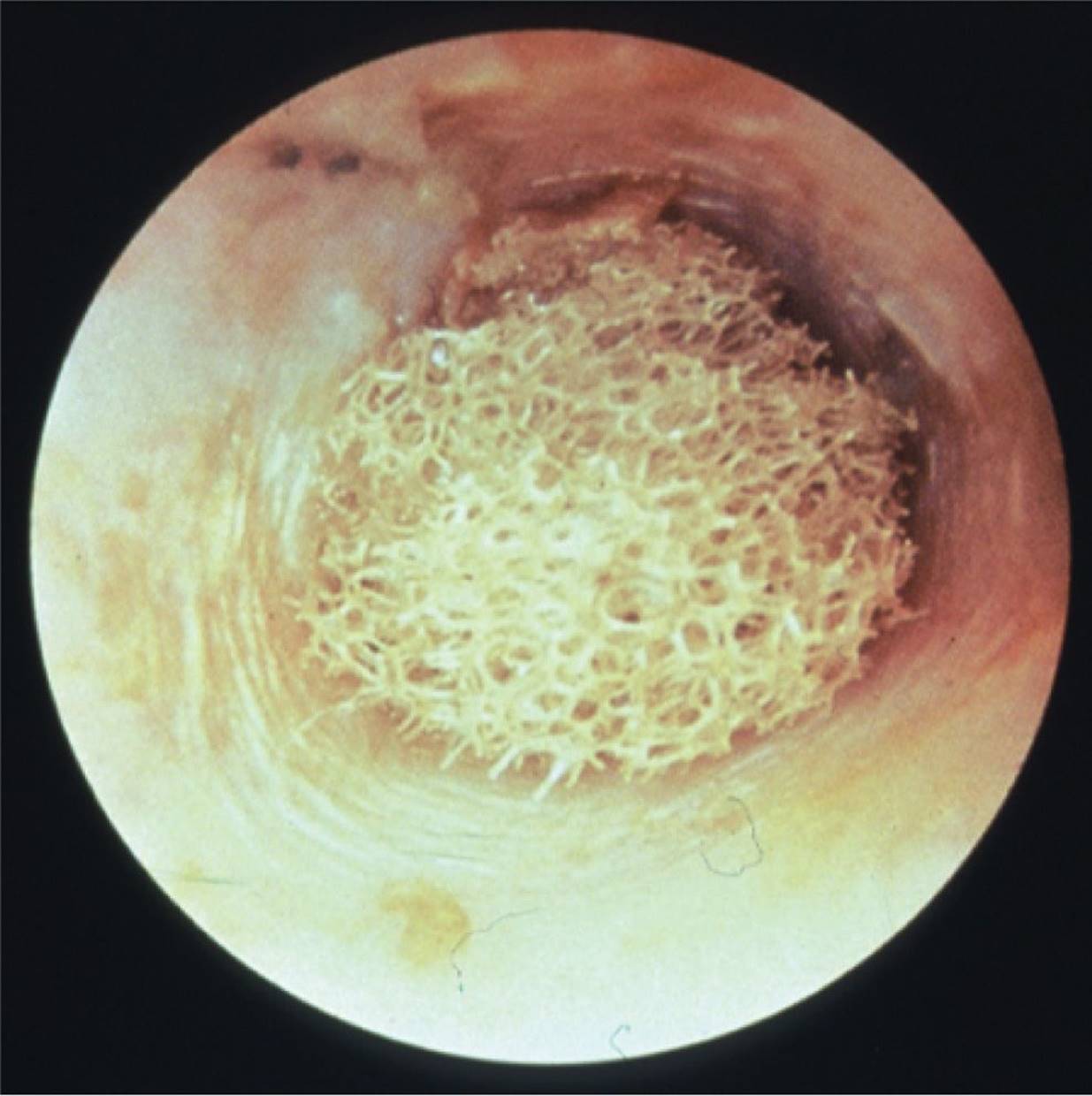
Figure 20-2 Foreign body in ear canal. (Courtesy of Welch Allyn, Inc. Skaneatleles Falls, NY.)
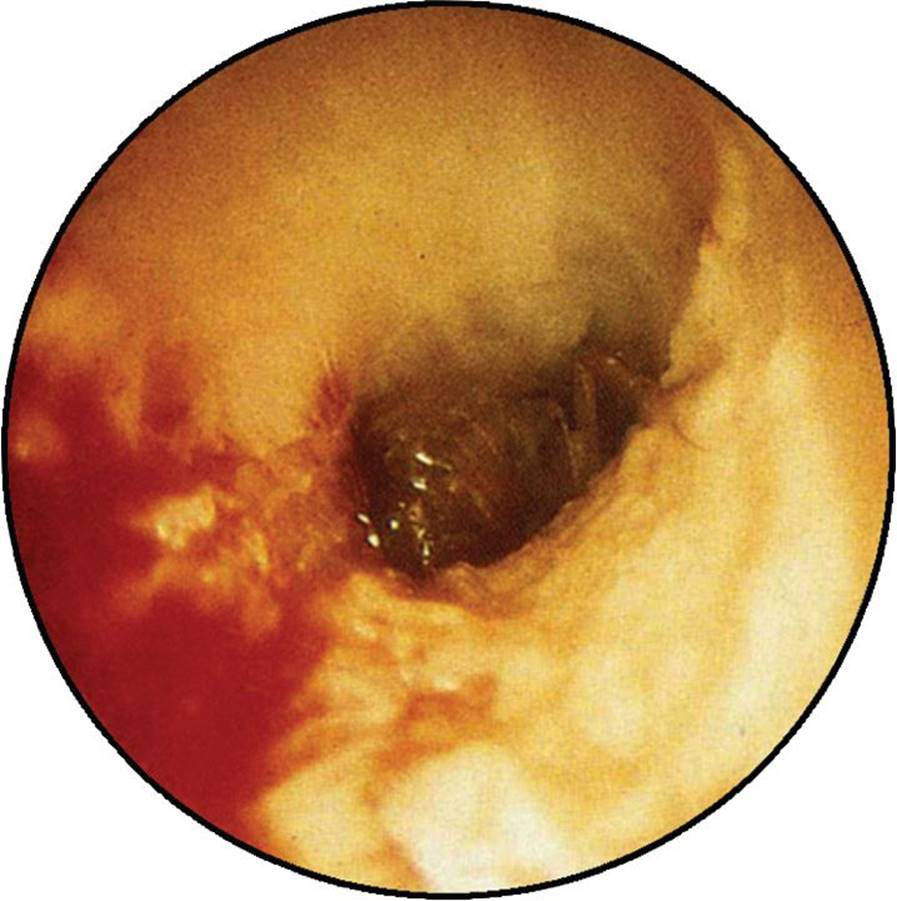
Figure 20-3 Cockroach in external canal. Note the visible body and legs from the cockroach. There is also surrounding edema and hyperemia. (Courtesy of Ellen Deutsch, MD.)

Figure 20-4 Acute otitis externa. Note that the EAC is edematous with narrowing. There is also discharge present. (Courtesy of Steven D. Handler, MD, MBE.)

Figure 20-5 Otorrhea associated with a cholesteatoma. Note the white-colored discharge visible at the os of the EAC, as well as crust on the antitragus. (Courtesy of Ellen Deutsch, MD.)

Figure 20-6 Mycotic otitis externa. Fungal overgrowth produces a moist appearing, whitish plaque. (Used with permission from Handler SD, Myer CM. Atlas of Ear, Nose and Throat Disorders in Children. Hamilton: BC Decker; 1998:24.)
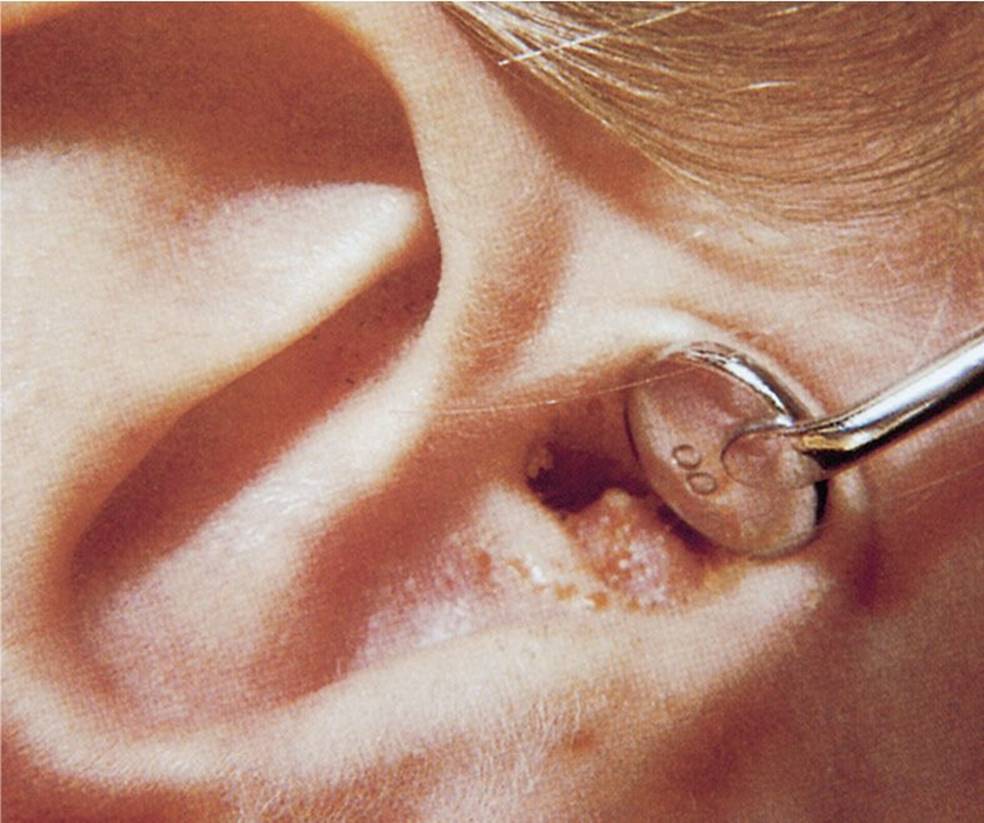
Figure 20-7 Furuncle of the EAC. Note the large erythematous papule with a pustular tip. (Used with permission from Handler SD, Myer CM. Atlas of Ear, Nose and Throat Disorders in Children. Hamilton: BC Decker; 1998:24.)

Figure 20-8 Ramsay Hunt syndrome. Vesicles in the external ear canal in a case of geniculate herpes. (From Campbell WW. DeJong’s The Neurologic Examination. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2012.)

Figure 20-9 External auditory canal exostoses. Note the nontender nodular swellings covered by normal skin deep in the ear canal. (From Bickley LS, Szilagyi P. Bates’ Guide to Physical Examination and History Taking. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003.)
DIFFERENTIAL DIAGNOSIS

Other Diagnoses to Consider
• Osteomyelitis
• Acne
• Cholesteatoma
• EAC exostosis
• Malignant otitis externa
When to Consider Further Evaluation or Treatment
• In immunocompromised patients, consider parenteral treatment for EAC infections, and consider less common organisms as possible etiologic agents.
• If penetrating injury is suspected, consider imaging and consultation with subspecialists from trauma surgery, neurosurgery, and/or otolaryngology to evaluate for further injury.
• If acute otitis media with perforation is suspected, treat with oral antibiotics, and consider the use of topical antibiotic drops to the EAC.
• If symptoms do not improve within 48 to 72 hours of initiating treatment, consider other etiologies and referral to an otolaryngologist.
• Permanent facial nerve paralysis may be seen with reactivated varicella zoster virus in Ramsay Hunt syndrome. Early treatment with steroids and oral acyclovir and referral to an otolaryngologist should be considered.
SUGGESTED READINGS
Ely JW, Hansen MR, Clark EC. Diagnosis of ear pain. Am Fam Physician. 2008;77(5):621–628.
Handler SD, Myer CM. Atlas of Ear, Nose, and Throat Disorders in Children. Hamilton: BC Decker; 1998:22–27.
Kaushik V, Malik T, Saeed SR. Interventions for acute otitis externa. Cochr Database Syst Rev. 2010;(1):CD004740. doi:10.1002/14651858.CD004740.pub2.
Miravalle AA. Ramsay Hunt Syndrome. http://emedicine.medscape.com/article/1166804-overview. Accessed November 11, 2013.
Osguthorpe JD, Nielsen DR. Otitis externa: Review and clinical update. Am Fam Physician. 2006;74(9):1510–1516.
Sharpe SJ, Rochette LM, Smith GA. Pediatric battery-related emergency department visits in the United States, 1990–2009. Pediatrics. 2012;129:1111–1117.
Stoner MJ, Dulaurier M. Pediatric ENT emergencies. Emer Med Clin N Am. 2013;31:795–808.
Sweeney CJ, Gilden DH. Ramsay Hunt syndrome. J Neurol Neurosurg Psychiatr. 2001;71:149–154.