Approach to the Problem
Diffuse red rashes are a common complaint. The differential diagnosis for this type of rash is wide, including minor, self-resolving illnesses that can be managed safely in the outpatient setting to life-threatening conditions that require prompt and aggressive intervention. Diffuse red rashes are most often a result of exposure to sunlight, a number of infections, or medications. In some cases, the combination of exposure to sunlight and medication is the reason for the rash.
Key Points in the History
• The timing of the rash in the setting of medication ingestion is often helpful in determining the etiology.
• Exanthematous drug eruptions usually occur within 5 to 14 days after starting medications. Medications most commonly implicated in drug eruptions include antibiotics (penicillins, sulfonamides), nonsteroidal anti-inflammatory drugs (NSAIDs), and anticonvulsants (carbamazepine, phenytoin). Pruritus is often an associated symptom.
• A severe form of drug eruption known as DRESS (drug rash with eosinophilia and systemic symptoms) usually occurs 2 to 8 weeks after a medication is initiated, most commonly after exposure to anticonvulsants.
• In the majority of cases, the onset of Red Man syndrome is within 60 minutes of initiation of vancomycin infusion.
• The typical prodrome of measles (rubeola) includes fever, malaise, cough, coryza, conjunctivitis, and Koplik spots (small red lesions on mucous membranes with a white central spot) followed on day 3 by the rash that spreads in a cephalocaudal fashion.
• The diffuse painful, sometimes painless, erythema of sunburn occurs 3 to 5 hours after exposure and usually peaks at 12 to 24 hours, after ultraviolet (UV) radiation of as little as 30 minutes duration.
• Drug- and chemical-induced photosensitivity similar in appearance to a typical sunburn results from the combination of UVA light exposure and the use of photosensitizing medications such as NSAIDs, sulfonamides, quinolones, tetracyclines, furosemide, griseofulvin, thiazides, amiodarone, and isoniazid.
• Polymorphous light eruption is a light-induced, nonscarring, pruritic eruption that tends to be most severe at the beginning of the sunny season and lessens in severity as the season progresses.
• Initial symptoms of staphylococcal scalded skin syndrome (SSSS) include fever, malaise, irritability, conjunctivitis, pharyngitis, and impetigo prior to the onset of the rash. SSSS can present at any age but preferentially affects newborns during their first week of life and children under age 5.
• In toxic shock syndrome (TSS), there is typically a focus of infection such as a tampon, soft tissue infection, abscess, or burn.
Key Points in the Physical Examination
• Drug-related rashes usually manifest as generalized morbilliform eruptions, generally starting on the face and trunk, and then spreading distally.
• DRESS is a severe form of a drug reaction that is characterized by fever, erythroderma, lymphadenopathy, facial edema, transaminitis, leukocytosis with eosinophilia, and visceral involvement.
• Erythema, flushing, and pruritus of the face and upper body are typical of Red Man syndrome. Severe reactions include generalized erythema, intense pruritus, and hypotension.
• The typical rash seen in measles is a nonpruritic, blotchy, erythematous, blanching, maculopapular rash that spreads in a cephalocaudal manner. Koplik spots are considered pathognomonic for measles.
• The appearance of erythema on sun-exposed areas that become painful and that spare areas of covered skin aids with diagnosing sunburn as well as drug- and chemical-induced photosensitivity.
• Polymorphous light eruption is limited to sun-exposed areas such as the face, posterior neck, and extremities. Rash occurs within hours and occasionally 1 to 2 days after sun exposure with pruritus as a key finding.
• Parvovirus B19 infection, or erythema infectiosum, causes an intense erythema specifically on the face and a reticulated erythematous rash on the rest of the body.
• Tonsillopharyngitis with fever and sore throat followed by the development of a blanching, confluent erythematous rash with a sandpaper quality is consistent with scarlet fever. Pastia lines are accentuated erythema with petechiae in a linear pattern in skin folds in areas such as the antecubital fossa and axilla.
• The widespread erythroderma of SSSS appears similar to a sunburn, is tender to touch, and is notably prominent in the perioral and flexural areas. The rash then progresses to flaccid bullae that easily rupture. Nikolsky sign (separation of the upper epidermis with gentle pressure or friction) is a classic finding.
• The diffuse blanching erythroderma of TSS, which can also resemble a sunburn, is distinguished by high fevers, abdominal distress, myalgias, headache followed by hypotension, and multisystem organ involvement, as well as subsequent desquamation of the rash.
• The typical petechial rash of Rocky Mountain spotted fever may start as a maculopapular eruption peripherally, which then spreads centrally before becoming petechial.
|
PHOTOGRAPHS OF SELECTED DIAGNOSES |

Figure 63-1 Sunburn. Diffuse erythema on lateral aspect of arm. (Courtesy of George A. Datto, III, MD.)

Figure 63-2 Photosensitivity. Edematous and erythematous sharp-bordered lesion that developed on ankle after sun exposure. (Courtesy of George A. Datto, III, MD.)

Figure 63-3 Drug rash. Erythroderma with fine morbilliform rash that developed after antibiotic exposure. (Courtesy of George A. Datto, III, MD.)

Figure 63-4 Rash seen with scarlet fever. Note the diffuse distribution of this rash that is more intense in the lower abdomen and groin. (Courtesy of Esther K. Chung, MD, MPH.)
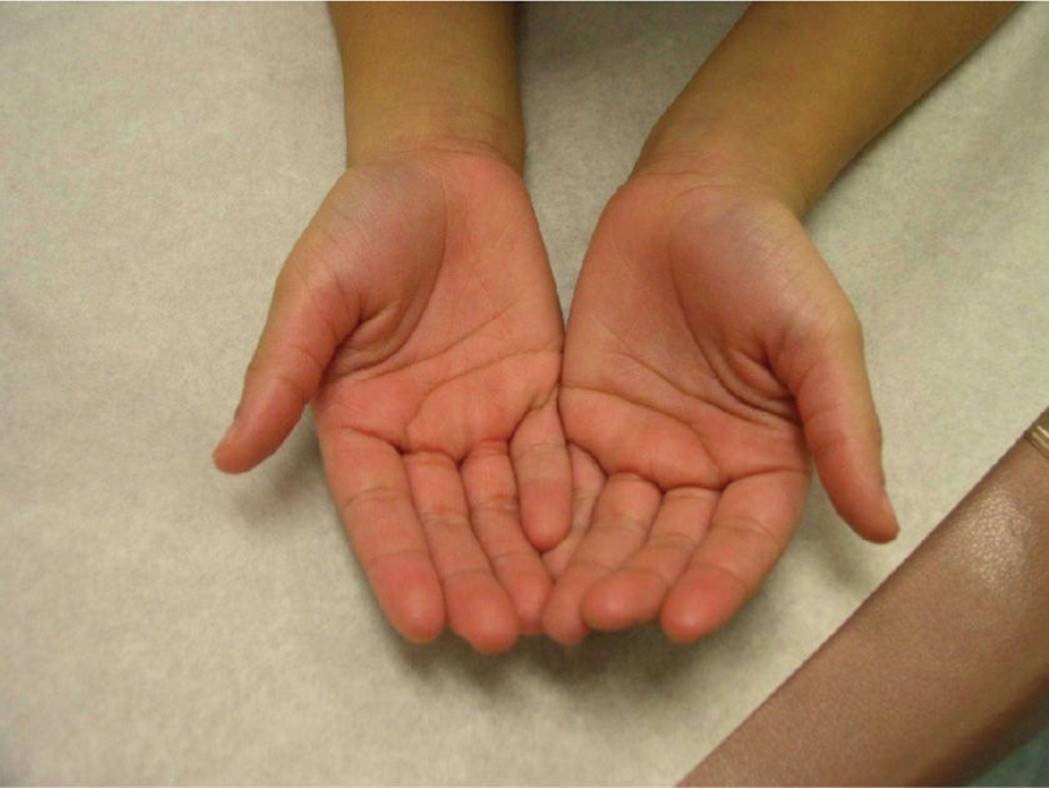
Figure 63-5 Palmar erythema. Note the intense palmar redness seen in a child with scarlet fever. (Courtesy of Esther K. Chung, MD, MPH.)

Figure 63-6 Staphylococcal scalded skin syndrome. A 4-year-old boy with the characteristic erythema and skin sloughing seen with SSSS. (Courtesy of Bethlehem Abebe-Wolpaw, MD.)

Figure 63-7 Measles. Child with measles (rubeola) showing the characteristic conjunctivitis, coryza, and red, blotchy rash that appear around day 3 of illness, first on the face and then becoming more generalized. (Used with permission from Centers for Disease Control and Prevention Public Health Image Library.)
DIFFERENTIAL DIAGNOSIS

Other Diagnoses to Consider
• Systemic lupus erythematosus
• Dermatomyositis
• Kawasaki disease
• Infectious mononucleosis
• Porphyrias
• Stevens–Johnson syndrome
• Toxic epidermal necrolysis
• Sézary syndrome, a type of cutaneous T-cell lymphoma
• Omenn syndrome, a form of severe combined immunodeficiency with desquamation
When to Consider Further Evaluation or Treatment
• Avoid sun exposure until the resolution of sunburn or photosensitivity rash. Liberal use of sunscreen with minimum of SPF 30 is encouraged. In those with severe or extensive findings, oral and/or topical steroids may be considered.
• Discontinuation of the causative agent in drug-related eruptions is imperative for resolution of symptoms. Antihistamines and topical steroids can alleviate symptoms.
• Diagnosis of streptococcal pharyngitis and/or scarlet fever warrants treatment with penicillin to reduce infectivity, hasten resolution, and prevent rheumatic fever.
• SSSS usually requires hospitalization for young patients, IV antibiotics, as well as close attention to fluid and electrolyte status because of increased fluid losses seen in this syndrome. The rash requires topical wound care similar to that for thermal burns, including analgesics, emollients, and gentle handling.
• Watch for aplastic crisis in patients with hemoglobinopathies who present with parvovirus B19 infection.
• Prompt recognition of TSS is essential to enable immediate treatment in an intensive care setting with fluid resuscitation, antibiotics, and vasopressors as well as removal of focus of infection (tampons, drainage of abscesses).
SUGGESTED READINGS
Aber C, Connelly EA, Schachner LA. Fever and rash in a child: when to worry? Pediatr Ann. 2007;36:30–38.
Aronson PL, Florin TA. Pediatric dermatologic emergencies: a case-based approach for the pediatrician. Pediatr Ann. 2009;38:109–116.
Berk DR, Bayliss SJ. MRSA, staphylococcal scalded skin syndrome, and other cutaneous bacterial emergencies. Pediatr Ann. 2010;39:627–633.
Grossberg AL. Update on pediatric photosensitivity disorders. Curr Opin Pediatr. 2013;25:474–479.
Kress DW. Pediatric dermatology emergencies. Curr Opin Pediatr. 2011;23:403–406.
Pacha O, Hebert AA. Pediatric photosensitivity disorders. Dermatol Clin. 2013;31:317–326.
Segal AR, Doherty KM, Leggott J, et al. Cutaneous reactions to drugs in children. Pediatrics. 2007;120:e1082–e1096.
Seth D, Kamat D, Montejo J. DRESS syndrome: a practical approach for primary care practitioners. Clin Pediatr. 2008;47:947–952.