The human nervous system is the most complex of all systems in the body and is responsible for perceiving, processing, and transmitting information throughout the organism and generating responses to the information. The nervous system is divided into the peripheral nervous system (PNS) and the central nervous system (CNS) (Fig. 9-1). The PNS is subdivided into the autonomic nervous system (ANS), which controls automatic functioning, like breathing and heart rate, and the somatic nervous system, which receives sensory information and sends information to the CNS and from the CNS to skeletal muscles. The CNS is comprised of the brain and spinal cord and integrates and controls all bodily functions as well as thought processes. All these systems are interconnected and work together.
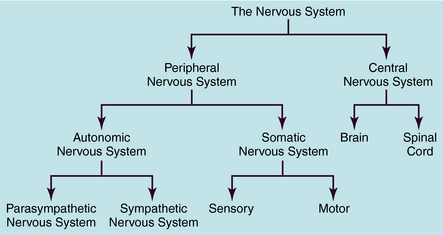
FIGURE 9–1 Divisions of the nervous system.
The ANS innervates the heart, blood vessels, visceral organs, exocrine glands, and virtually all other organs that contain smooth muscle. Smooth muscle function is also controlled by chemical substances released locally or systemically. The ANS controls key visceral processes, including cardiac output, blood flow to specific organs, glandular secretions, waste removal, and activities related to reproduction. Regulation of the functions of these organs is generally not under conscious control, which is why the ANS is often referred to as the “involuntary” nervous system. Although the ANS innervates most bodily structures, it does not innervate skeletal muscle fibers, which are under the voluntary control of higher centers in the CNS. Nerves that control skeletal muscles are called somatic motor nerves and are functionally and anatomically different from autonomic nerves. Sensory nerves are divided into somatosensory and special senses such as hearing and vision. Somatosensory nerves are located throughout the body and convey touch, temperature, position in space, and pain.
DIVISIONS OF THE AUTONOMIC NERVOUS SYSTEM
The two major divisions of the ANS, the parasympathetic and sympathetic systems, function in parallel to maintain homeostasis by regulating bodily functions. Stimulation of the sympathetic system expends energy and leads to “flight, fright, or fight” responses characterized by increased heart rate, blood pressure, and respiration; increased blood flow to skeletal muscles; and
|
Abbreviations |
|
|
ACh |
Acetylcholine |
|
AChE |
Acetylcholinesterase |
|
ANS |
Autonomic nervous system |
|
cAMP |
Cyclic adenosine monophosphate |
|
CNS |
Central nervous system |
|
COMT |
Catechol-O-methyltransferase |
|
DA |
Dopamine |
|
DOPA |
Dihydroxyphenylalanine |
|
Epi |
Epinephrine |
|
GI |
Gastrointestinal |
|
MAO |
Monoamine oxidase |
|
NE |
Norepinephrine |
|
PNS |
Peripheral nervous system |
|
SA |
Sinoatrial |
dilation of the pupil (mydriasis). In contrast, stimulation of the parasympathetic system conserves energy (“rest and digest”) and leads to responses characterized by decreased heart rate, blood pressure, and respiration; increased secretions; and constriction of the pupil (miosis).
Although the parasympathetic and sympathetic systems differ both anatomically and functionally, they also share some features. The outflow of both divisions from the CNS consists of two neuron relays named after their anatomical location relative to the autonomic ganglia, or relay centers. Preganglionic neurons have their cell bodies in the spinal cord and the brainstem and their nerve terminals at autonomic ganglia, where they relay information to cell bodies of postganglionic neurons. Postganglionic neurons send their axons directly to effector organs (heart, blood vessels, visceral organs, and glands), where they relay information to these cells; these synapses are often referred to as neuroeffector junctions. Thus the preganglionic fibers of both the sympathetic and parasympathetic systems synapse with postganglionic fibers at autonomic ganglia. However, the location of the ganglia differs for the two systems, with parasympathetic ganglia located close to the organ innervated and most sympathetic ganglia located near the spinal cord. Due to the different ganglionic locations, the lengths of the preganglionic fibers relative to the postganglionic fibers also differ. Both sympathetic and parasympathetic preganglionic neurons release acetylcholine (ACh) as the neurotransmitter at ganglia. However, parasympathetic postganglionic neurons release ACh to relay their information at the neuroeffector junction, whereas most sympathetic postganglionic fibers release norepinephrine (NE, also called noradrenaline).
Parasympathetic and sympathetic neurons are defined anatomically, with parasympathetic neurons arising from the sacral region of the spinal cord and from the brainstem and sympathetic neurons arising from thoracic and lumbar regions of the spinal cord. They are not defined by the neurotransmitter released, and sympathetic fibers that innervate some sweat glands release ACh rather than NE. An anatomical representation of the sympathetic and parasympathetic systems is shown in Figure 9-2, and the commonalities and differences between the systems are summarized in Table 9-1.

FIGURE 9–2 Schema of the autonomic nervous system depicting the functional innervation of peripheral effector organs and the anatomical origin of peripheral autonomic nerves from the spinal cord. The Roman numerals on nerves originating in the tectal region of the brainstem refer to the cranial nerves that provide parasympathetic outflow to the effector organs of the head, neck, and trunk.
TABLE 9–1 Comparison of the Parasympathetic and Sympathetic Divisions of the Autonomic Nervous System (ANS)

The enteric nervous system is often considered to be a third division of the ANS. This system is composed of a meshwork of fibers innervating the gastrointestinal (GI) tract, pancreas, and gall bladder. The enteric nervous system releases a variety of different neurotransmitters and is independent of CNS control. Although components of the enteric system are innervated by parasympathetic preganglionic fibers, local control appears to dominate function.
Although many consider the ANS to be an efferent system, almost all peripheral nerves (both autonomic and somatic) have afferent sensory fibers that provide feedback to the CNS. These visceral afferent fibers are unmyelinated and have their cell bodies in the dorsal root ganglia of the spinal nerves and in cranial nerve ganglia. These sensory neurons and nerve fibers function as a feedback system to autonomic efferent control centers in the CNS, mediating sensation and vasomotor, respiratory, and viscerosomatic outflow.
Parasympathetic Nervous System
Cell bodies giving rise to preganglionic parasympathetic nerves exit the CNS at cranial and sacral levels (see Fig. 9-2). The cranial portion of the parasympathetic outflow (cranial nerves III, VII, IX, and X) innervates structures in the head, neck, thorax, and abdomen. The sacral division of the parasympathetic nervous system forms the pelvic nerve and innervates the remainder of the GI tract and the pelvic viscera, including the bladder and reproductive organs.
The preganglionic neurons of the parasympathetic nervous system are myelinated and very long, such that parasympathetic ganglia are located in or near the effector organs. Consequently, postganglionic parasympathetic neurons, which are generally unmyelinated, are short.
Sympathetic Nervous System
Cell bodies for preganglionic sympathetic neurons originate in the intermediolateral cell column of the spinal cord at the thoracic and lumbar levels from T1 to L2 (see Fig. 9-2). Relatively short preganglionic, usually myelinated, neurons project to the sympathetic ganglia outside the spinal vertebrae. Most of these neurons synapse in the 22 segmentally arranged ganglia that form two chains located bilaterally adjacent to the spinal cord, and are often called the paravertebral chain. Postganglionic sympathetic neurons are generally unmyelinated and send long postganglionic fibers to their effector organs. Although most preganglionic sympathetic neurons synapse in the paravertebral sympathetic ganglia, several are prevertebral and lie near the bony vertebral column in the abdomen and pelvis (celiac, superior and inferior mesenteric, and aorticorenal), while a few (cervical ganglia and ganglia connected to urinary bladder and rectum) lie near the organs innervated.
The adrenal medulla is also a part of the sympathetic nervous system. It contains chromaffin cells that are embryologically and anatomically similar to sympathetic ganglia. Chromaffin cells are innervated by typical preganglionic sympathetic nerves and synthesize and secrete epinephrine (Epi, also called adrenaline) into the blood, analogous to postganglionic sympathetic neurons, which release NE.
Autonomic Regulation of Peripheral Organs
Both parasympathetic and sympathetic nerves innervate most organs of the body. Generally, these two branches of the ANS produce opposing responses in effector organs. There is generally a balance between sympathetic and parasympathetic effects on most organs, such that inhibition of one often leads to an increase in the response mediated by the other. However, there are some exceptions where the two systems cause similar responses. Some organs, such as the vasculature and spleen, receive only one type of innervation, which, in these cases, is sympathetic.
The importance of the dual innervation of most organs is evidenced by hypertension, which may involve an increase in sympathetic relative to parasympathetic control of the heart. Increased sympathetic effects can be produced by changes in neural firing rate, catecholamine concentrations at the neuroeffector junction or postjunctional receptors, or signal transduction pathways. Although there is support for each of these mechanisms, the first two are likely most important. Thus drugs that inhibit sympathetically mediated cardiovascular effects are useful for treating hypertension (see Chapters 11 and 12).
One sympathetic preganglionic neuron may ramify and ultimately synapse with many postganglionic sympathetic neurons, leading to diffuse responses. By contrast, parasympathetic preganglionic neurons generally form only single synapses with postganglionic neurons, resulting in more discrete and localized responses. This anatomical distinction has profound physiological significance. Activation of sympathetic outflow, triggered by anger, fear, or stress, causes a state of activation characteristic of the “fight, flight, or fright” response. Heart rate is accelerated, blood pressure is increased, perfusion to skeletal muscle is augmented as blood flow is redirected from the skin and splanchnic region, the blood glucose concentration is elevated, bronchioles and pupils are dilated, and piloerection occurs.
In contrast, activation of parasympathetic outflow is associated with conservation of energy and maintenance of function during periods of lesser activity. Activation of parasympathetic outflow reduces heart rate and blood pressure, activates GI movements, and results in emptying of the urinary bladder and rectum. Furthermore, lacrimal, salivary, and mucous cells are activated, and the smooth muscle of the bronchial tree is contracted. Although the parasympathetic nervous system is essential for life, the sympathetic nervous system is not. Animals completely deprived of their sympathetic nervous system can survive in a controlled environment but have difficulty responding to stressful conditions.
NEUROTRANSMISSION AND NEUROTRANSMITTERS IN THE AUTONOMIC NERVOUS SYSTEM
Neurotransmission
Neurotransmission is the process of effective transfer and integration of information in the nervous system. Neurotransmitters are endogenous substances released from nerve terminals, which act onreceptors present on the membrane of postsynaptic cells. It is the interaction of the released neurotransmitter with the receptor that produces a functional change in the cell (Fig. 9-3).
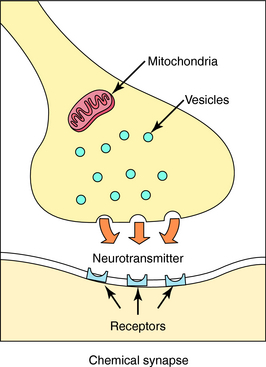
FIGURE 9–3 The process of chemical neurotransmission. Neurotransmitter molecules are released from synaptic vesicles within the nerve terminal into the synaptic cleft, where they diffuse to the postjunctional side and interact with their receptors.
Depolarization of a presynaptic nerve terminal leads to release of a neurotransmitter into the extracellular fluid between the presynaptic and postsynaptic cells (the synaptic cleft). Calcium (Ca++) provides the essential link between depolarization and transmitter release. When a nerve terminal is depolarized, there is a large influx of Ca++ caused by opening of voltage-dependent Ca++ channels in the membrane. This influx promotes fusion of transmitter-containing synaptic vesicles with the plasma membrane resulting in exocytosis, which releases neurotransmitter into the synapse. After exocytosis, the voltage-dependent Ca++ channels inactivate rapidly, and the intracellular Ca++ concentration returns to normal by sequestration into intracellular compartments and active extrusion from the cell. The steps linking the arrival of an action potential to neurotransmitter release are summarized in Figure 9-4.
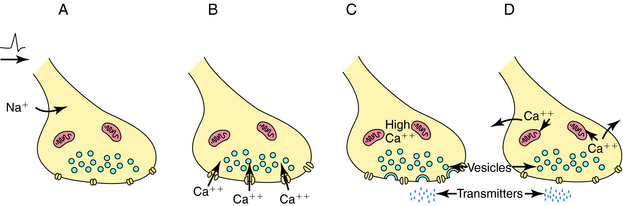
FIGURE 9–4 Sequence of events linking nerve terminal depolarization to release of neurotransmitter. A, The action potential arrives at the nerve terminal and depolarizes the membrane. B, Voltage-gated Ca++ channels open, allowing the influx of Ca++ down its concentration gradient. C, The increased intracellular Ca++ concentration promotes the fusion of transmitter-containing synaptic vesicles with the plasma membrane, resulting in exocytosis of the vesicular contents. D, The Ca++ channels rapidly inactivate, and the intracellular Ca++ concentration is returned to normal by both sequestration into mitochondria and active extrusion from the cell.
It is important to understand that voltage-dependent Ca++ channels in nerve terminals differ from those in other tissues. The Ca++ channel antagonists are an important class of drugs that block voltage-dependent Ca++ channels in cardiac and smooth muscle (see Chapter 20). However, there are distinct subtypes of these channels that can be distinguished by their electrical and pharmacological properties. The Ca++ channel antagonists block the channels most often found in cardiac and smooth muscle (L type) and have no effect on most of the voltage-dependent Ca++ channels found in nerve terminals (N type). This is fortunate, because if Ca++ channel antagonists also blocked neurotransmitter release, their toxicity would undoubtedly prevent them from being useful therapeutically.
After release, the neurotransmitter diffuses across the synaptic cleft to interact with specific receptors on the dendrites and cell body of the postganglionic neuron or on cells of the effector organ. The postsynaptic cell responds in an appropriate fashion to the received message. Thus the nerve terminal has mechanisms for storing and releasing neurotransmitters in response to depolarization, and the postsynaptic cell has receptors for detecting the presence and identity of different neurotransmitters and initiating appropriate changes in physiology or metabolism. Nerve terminals also have efficient mechanisms for the degradation and reutilization (reuptake) of neurotransmitters to ensure the rapid termination of arriving messages. These processes, neurotransmitter synthesis, storage, release, reuptake, and degradation, represent the sites of action of many drugs.
Neurotransmission at autonomic ganglia and neuroeffector junctions is illustrated in Figure 9-5. In both sympathetic and parasympathetic ganglia, preganglionic stimulation leads to the release of ACh, which activates postjunctional nicotinic acetylcholine receptors on postganglionic neurons to increase ion permeability, resulting in generation of an action potential that is propagated down the postganglionic nerve. When the action potential reaches the neuroeffector junction, either ACh or NE is released to activate muscarinic cholinergic or adrenergic receptors, respectively, on cells of the effector organ to produce an appropriate response.
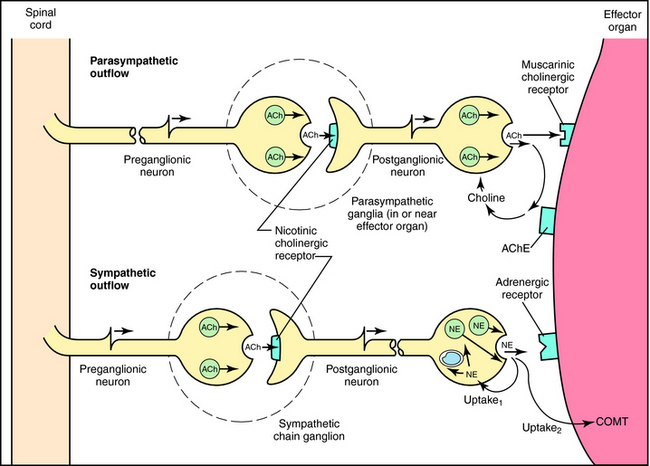
FIGURE 9–5 Neurochemical transmission in the parasympathetic and sympathetic divisions of the ANS. Upon the arrival of an action potential at the preganglionic nerve terminal, the neurotransmitter ACh is released by both parasympathetic and sympathetic ganglia. ACh diffuses across the synaptic cleft to interact with nicotinic cholinergic receptors on postganglionic neurons (often referred to as ganglionic receptors). This interaction results in the generation and propagation of action potentials down postganglionic neurons to elicit the release of neurotransmitter at the postganglionic nerve terminal (neuroeffector junction). The neurotransmitter released from postganglionic parasympathetic nerves is ACh, which diffuses across the synaptic cleft and activates muscarinic cholinergic receptors on the effector organ. The liberated ACh is rapidly metabolized by AChE to acetic acid and choline; the latter is transported into the parasympathetic nerve terminal and is used to resynthesize ACh. At the postganglionic sympathetic neuroeffector junction, the neurotransmitter released is NE, which diffuses across the neuroeffector junction to stimulate adrenergic receptors and elicit the end-organ response. Most of the liberated NE is transported back into the sympathetic nerve terminal (uptake1) and is either stored in vesicles or metabolized by MAO located in the mitochondria. A smaller amount of the liberated NE may diffuse away and be accumulated by extraneuronal cells (uptake2), after which it may be metabolized by COMT.
Neurotransmitter Synthesis, Storage, and Inactivation
Acetylcholine
ACh is synthesized in cholinergic nerve terminals by the acetylation of choline, a process catalyzed by the enzyme choline acetyltransferase. As shown in Figure 9-6, acetyl coenzyme A provided by mitochondria serves as the acetyl donor; choline is provided by both high-affinity uptake after ACh hydrolysis and phospholipid hydrolysis within the neuron.
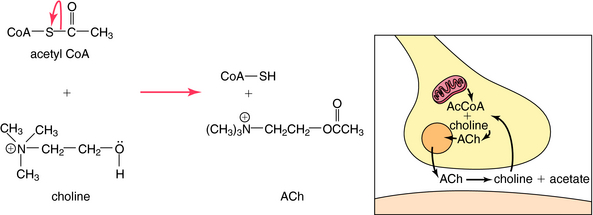
FIGURE 9–6 Synthesis, storage, and inactivation of ACh. ACh is synthesized in cholinergic nerve terminals through the acetylation of choline, a process catalyzed by the enzyme choline acetyltransferase. Acetyl coenzyme A (AcCoA) is provided by mitochondria and serves as the acetyl donor, whereas the choline comes from the cytoplasm and is provided by both high-affinity choline uptake and phospholipid hydrolysis within the neurons. After the release of ACh and its interaction with its receptors, it is hydrolyzed by AChE to acetate and choline; the latter is taken back up into the nerve terminal and is reused for ACh synthesis.
After synthesis, ACh is stored in vesicles in cholinergic nerve terminals, from which it is released upon depolarization. The action of ACh is terminated by the enzyme acetylcholinesterase (AChE), which rapidly hydrolyzes ACh into acetic acid and choline. Acetic acid diffuses from the synaptic cleft, whereas most of the choline is taken back up into the nerve terminal by the high-affinity choline transporter. Once inside the nerve terminal, choline can be reused for ACh synthesis.
Norepinephrine and Epinephrine
NE is synthesized in adrenergic nerve terminals by a series of enzymatic reactions beginning with the precursor tyrosine, as depicted schematically in Figure 9-7 and chemically in Figure 9-8. The first step, which takes place in the cytoplasm of postganglionic sympathetic nerve terminals, involves hydroxylation of tyrosine in the meta position by tyrosine hydroxylase to form the catechol derivative 3,4-dihydroxyphenylalanine (DOPA). Tyrosine hydroxylase is rate-limiting for the biosynthesis of all catecholamines including NE, Epi, and dopamine (DA). DOPA is subsequently decarboxylated by L-aromatic amino acid decarboxylase to form DA, which is actively taken up into storage vesicles in the sympathetic nerve terminals. Inside the vesicle, a hydroxyl group is added by dopamine-β-hydroxylase to form NE, which is retained in the vesicle associated with ATP until released by arrival of an action potential. Dopamine-β-hydroxylase is the last enzyme in the biosynthesis of NE in postganglionic sympathetic neurons, which release only NE. In the adrenal medulla and some neurons within the CNS, NE and Epi coexist. The synthesis of Epi from NE occurs by the action of phenylethanolamine-N-methyltransferase, which methylates NE. In adult humans, Epi constitutes approximately 80% of the catecholamines in the adrenal medulla, with NE making up the remainder.
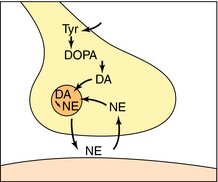
FIGURE 9–7 Synthesis, storage, and termination of the action of NE. NE is synthesized in adrenergic nerve terminals by a sequence of reactions beginning with the conversion of tyrosine to DOPA and DOPA to DA in the cytoplasm. DA is transported into storage vesicles in sympathetic nerve terminals, where it is converted to NE. After the release of NE and interaction with its receptors, the action of NE is terminated by neuronal reuptake into the nerve terminal.
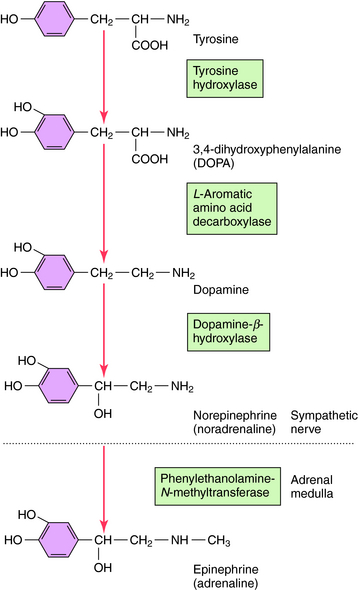
FIGURE 9–8 Steps in the enzymatic biosynthesis of the catecholamines DA, NE, and Epi. The enzymes involved in each catalytic step are enclosed in boxes. The first three enzymatic steps occur in postganglionic sympathetic nerve terminals, leading to the synthesis of NE; all four steps occur in the adrenal medulla, resulting in the synthesis of Epi.
The action of NE is terminated by a combination of neuronal reuptake into the sympathetic nerve terminal by an energy-dependent pump (uptake1) and diffusion and uptake by an extraneuronal process (uptake2), as depicted in Figure 9-5. NE taken back up into sympathetic nerves may be oxidatively deaminated by the enzyme monoamine oxidase (MAO) present in mitochondria within nerve terminals, or it may be sequestered in vesicles for subsequent release. NE that diffuses to the extraneuronal uptake site may be inactivated by the enzyme catechol-O-methyltransferase (COMT). The metabolism of NE and Epi by MAO and COMT is depicted in Figure 9-9; numerous inactive metabolites are formed and excreted in blood and urine.
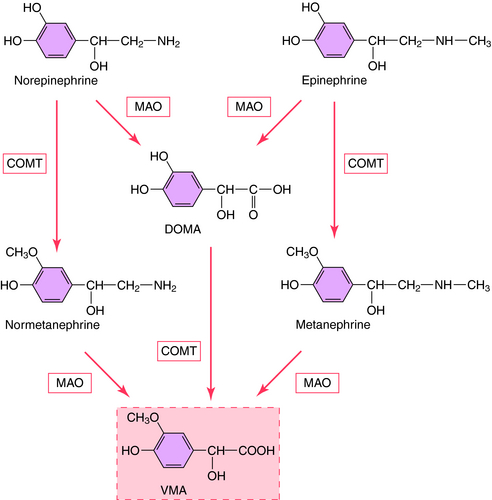
FIGURE 9–9 Major metabolic pathways for NE and Epi in the periphery. The major pathway for NE is on the left, whereas that for Epi is on the right. Both NE and Epi can be metabolized by monoamine oxidase (MAO) to dihydroxymandelic acid (DOMA), which is then converted by catechol-o-methyltransferase (COMT) to 3-methoxy-4-hydroxymandelic acid (VMA). Alternatively, NE may be converted to normetanephrine by COMT, followed by metabolism to VMA by MAO, whereas Epi may be converted to metanephrine by COMT, followed by metabolism to VMA by MAO. VMA is the final common metabolite for each of these catecholamines.
NEUROTRANSMITTER RECEPTORS IN THE AUTONOMIC NERVOUS SYSTEM
ACh and NE use different receptors to mediate their end-organ responses, and each neurotransmitter may interact with many distinct receptor subtypes (see Chapter 1). The many receptor subtypes are classified by pharmacological studies using selective agonists and antagonists and by their amino acid sequences. The genes that code for each of these receptors have now been cloned. It should be emphasized that the end-organ response is as much a function of the type of receptor present as of the neurotransmitter involved. Classification of cholinergic and adrenergic receptor subtypes is presented in Figure 9-10.
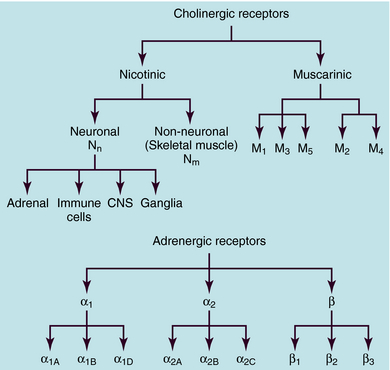
FIGURE 9–10 Classification of cholinergic and adrenergic receptor types and subtypes.
Cholinergic Receptors
ACh produces different effects at various sites throughout the body, often resulting from differences in the cholinergic receptors involved. The actions of ACh are mimicked in certain organs, including autonomic ganglia, by the plant alkaloid nicotine, hence the name nicotinic. The response to ACh in effector organs is more closely mimicked by the plant alkaloid muscarine, leading to the namemuscarinic. Thus responses to exogenous ACh or activation of the parasympathetic nervous system are described as being mediated by nicotinic or muscarinic receptors. Nicotinic receptors are ligand-gated ion channels, which, when activated by ACh, allow the influx of Na+ and Ca++. In contrast, muscarinic receptors are G-protein–coupled receptors which, when activated by ACh, activate G-proteins to induce downstream effects. These actions are illustrated schematically in Figure 9-11.
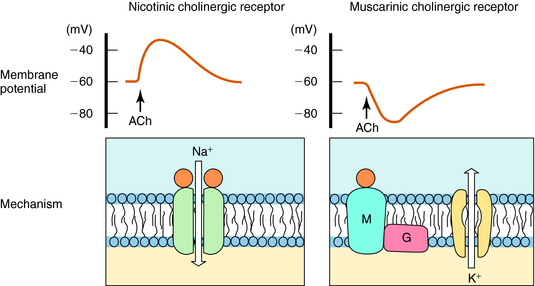
FIGURE 9–11 Activation of nicotinic and muscarinic cholinergic receptors by ACh can cause opposite effects on membrane potential. Activation of the nicotinic cholinergic (ionotropic) receptor (left) opens a ligand-gated channel to allow Na+ to enter and depolarize the cell. Activation of the muscarinic (M) cholinergic (metabotropic) receptor (right) activates a G-protein (G), which in turn can open a potassium (K+) channel, leading to K+ efflux and hyperpolarization.
The primary actions of ACh at both parasympathetic and sympathetic ganglia are mediated by activation of ganglionic nicotinic cholinergic receptors. These receptors are similar structurally and functionally to the nicotinic receptors in the CNS and on immune cells but differ from nicotinic receptors in skeletal muscle at the neuromuscular junction. These different types of nicotinic receptors can be stimulated or blocked selectively by different agonists and antagonists. Drugs affecting ganglionic nicotinic receptors are discussed in Chapter 10, and agents that affect skeletal muscle nicotinic receptors are discussed in Chapter 12.
The receptors mediating responses to ACh at parasympathetic neuroeffector junctions are muscarinic and consist of five subtypes (M1 to M5) based on their pharmacological specificities, amino acid sequences, and genes. Stimulation of M1, M3, and M5 receptors leads to activation of Gq and the phospholipase C-mediated generation of diacylglycerol and inositol-1,4,5-trisphosphate. Activation of M2and M4 receptors leads to inhibition of adenylyl cyclase through Gi and decreases in intracellular cyclic adenosine monophosphate (cAMP). The M2 receptor Gi protein is also linked directly to the opening of K+ channels.
In general, M1 receptors are located in autonomic ganglia (where they modulate effects of nicotinic receptor activation), M2 receptors are located in the heart, and M3 receptors are located in many glands and smooth muscles. The locations of the M4 and M5 receptors are less certain, although all five muscarinic receptor subtypes are found in the CNS. Drugs affecting muscarinic receptors are discussed inChapter 10.
Adrenergic Receptors
The first evidence that NE and Epi could activate more than one type of adrenergic receptor was provided by Ahlquist in 1948 by comparing the effects of Epi, NE, and the agonist isoproterenol on different tissues. The rank order of potency for activation of responses in some tissues was Epi > NE > isoproterenol, whereas the rank order of potency in other tissues was isoproterenol > Epi > NE. These results suggested the existence of two types of adrenergic receptors, which were termed α and β. The existence of these distinct subtypes was later confirmed by development of selective antagonists.
Subsequent studies have shown that there are many adrenergic receptor subtypes (see Fig. 9-10). β adrenergic receptors can be subdivided into three subtypes, β1, β2, and β3, and selective agonists and antagonists have been developed with different potencies at these receptors. Stimulation of each β adrenergic receptor subtype leads to activation of Gs, an increase in cAMP, and activation of cAMP-dependent protein kinase, leading to the phosphorylation of various intracellular proteins.
Pharmacological studies further subdivided α adrenergic receptors into two major types, α1 and α2, each of which is now known to comprise three additional subtypes (see Fig. 9-10), a classification that has been confirmed by cloning and comparing genes for these proteins. Thus, there are a total of nine adrenergic receptors, subdivided into three subfamilies (α1, α2, and β), each of which contains three distinct subtypes encoded by separate genes. Amino acid sequences are very similar among the subtypes within a given subfamily.
The α1 adrenergic receptors produce their effects the same way as M1, M3, and M5 receptors, by activation of Gq and phospholipase C-mediated generation of diacylglycerol and inositol-1,4,5-trisphosphate. The α2 adrenergic receptors usually produce their effects the same way as M2 and M4 receptors, by inhibiting adenylyl cyclase through Gi and decreasing intracellular cAMP. However, α2adrenergic receptors may also use other mechanisms of signal transduction. For example, in blood vessels, α2 receptor stimulation leads to the activation of a membrane Ca++ channel, resulting in Ca++influx.
Prejunctional Autoreceptors
Although adrenergic receptors mediating the actions of NE at sympathetic neuroeffector junctions are located postsynaptically on the organ innervated, prejunctional α2 adrenergic receptors have been identified on both adrenergic and cholinergic nerve terminals. Activation of these receptors by released NE or by administered α2 adrenergic receptor agonists decreases further release of neurotransmitter. This presynaptic inhibitory “autoreceptor” mechanism may be involved in the normal regulation of neurotransmitter release, because blockade of prejunctional α2 receptors leads to enhanced NE release. Presynaptic α2 receptors also exist on most cholinergic nerve terminals, and when these receptors are activated, release of ACh is inhibited. These prejunctional α2 receptors on cholinergic nerves may be activated by administered α2 receptor agonists, or by NE released from postganglionic sympathetic neurons synapsing near parasympathetic nerve terminals.
FUNCTIONAL RESPONSES MEDIATED BY THE AUTONOMIC NERVOUS SYSTEM
As mentioned, many organs receive both cholinergic and adrenergic innervation, and responses in these organs represent a complex interplay between the parasympathetic and sympathetic nervous systems. Often an organ is under the predominant control of a single division of the ANS, although both components are usually present and can influence any given response. Organs innervated by both sympathetic and parasympathetic nerves include the heart, eye, bronchial tree, GI tract, urinary bladder, and reproductive organs. Some structures, such as blood vessels, the spleen, and piloerector muscles, receive only a single type of innervation, generally sympathetic. The responses to nerve stimulation in each organ are mediated by the particular muscarinic cholinergic or adrenergic receptors present.
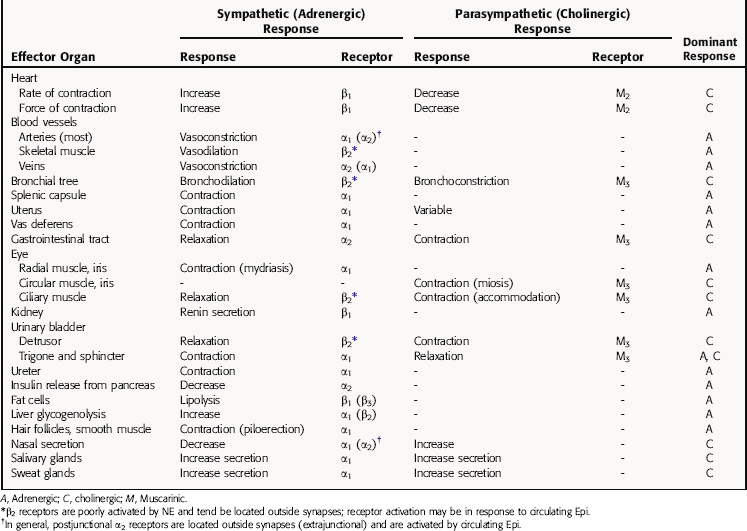
The responses to parasympathetic and sympathetic stimulation that occur in many important organs of the body are presented in Table 9-2. In most instances sympathetic and parasympathetic nerves mediate physiologically opposing effects. Thus, if one system inhibits a certain function, the other enhances it. It is important to note that the responses listed represent only those mediated by stimulation of nerves in innervated tissues, and that activation of autonomic receptors located in tissues lacking nerve innervation can also lead to responses. For example, although vascular smooth muscle has no parasympathetic innervation, it expresses muscarinic cholinergic receptors, which are functional and mediate responses to exogenously administered drugs; they probably play little or no normal physiological role.
TABLE 9–2 Responses Elicited in Effector Organs by Stimulation of Sympathetic and Parasympathetic Nerves
Drugs Acting on Autonomic Nerves and Receptors
Drugs that alter the sympathetic and parasympathetic systems and autonomic ganglia are discussed in detail in Chapters 10 11. This introduction will briefly review the types of pharmacological interventions possible and provide a few examples of drugs that act by different mechanisms.
Ganglionic Blockers
Drugs that block autonomic ganglia interfere with the transmission of nerve impulses from preganglionic nerve terminals to the cell bodies of postganglionic neurons. Because the neurotransmitter (ACh) and receptor (nicotinic) are identical in sympathetic and parasympathetic ganglia, ganglionic blockers inhibit both divisions of the ANS equally. However, the end-organ response may show a predominant adrenergic or cholinergic effect, because one system is generally dominant in a given organ (Table 9-3). Therefore interruption of ganglionic transmission selectively eliminates the dominant component, leading to a response characteristic of the less dominant component. For example, in the heart, the cholinergic system generally dominates at the level of the sinoatrial (SA) node. When a ganglionic blocker is administered, its greatest effect is on this cholinergic component, resulting in an apparent adrenergic effect (tachycardia). The classic ganglionic blockers are hexamethonium and mecamylamine (Table 9-4), which have limited clinical use because of their many actions.
TABLE 9–3 Effects of Ganglionic Blockade on Major Organ Systems
|
Organ System |
Predominant Tone |
Effect of Ganglionic Blockade |
|
Cardiovascular System |
||
|
Atria; SA node |
Parasympathetic |
Tachycardia |
|
Ventricle |
Sympathetic |
Reduced force of contraction |
|
Blood vessels |
Sympathetic |
Vasodilation; decreased venous return; hypotension |
|
Eye |
||
|
Ciliary muscle |
Parasympathetic |
Focused for far vision |
|
Iris |
Parasympathetic |
Mydriasis |
|
Glands |
||
|
Sweat |
Sympathetic |
Decreased sweat |
|
Salivary |
Parasympathetic |
Dry mouth |
|
Gastrointestinal Tract |
||
|
Smooth muscle |
Parasympathetic |
Decreased contractions; constipation |
|
Secretions |
Parasympathetic |
Decreased gastric and pancreatic secretions |
TABLE 9–4 Mechanisms of Action of Pharmacological Compounds Affecting the Autonomic Nervous System (ANS)
|
Action |
Mechanism(s) of Action |
Example |
|
Ganglionic blockade |
Interferes with transmission of nerve impulses between preganglionic and postganglionic neurons |
Hexamethonium Mecamylamine |
|
Inhibits neurotransmitter synthesis |
Inhibits enzymes involved in NE biosynthesis |
α-Methyltyrosine (inhibits tyrosine hydroxylase) Carbidopa (inhibits L-aromatic amino acid decarboxylase) |
|
Inhibits availability of choline for ACh synthesis |
Hemicholinium-3 |
|
|
Inhibits neurotransmitter release |
Interferes with adrenergic transmission |
Guanethidine |
|
Interferes with exocytosis of ACh-containing vesicles |
Botulinum toxin |
|
|
Promotes neurotransmitter release |
Activates ganglionic nicotinic receptors |
Nicotine |
|
Releases NE from cytoplasmic stores |
Tyramine Amphetamine |
|
|
Releases ACh from storage vesicles |
Black widow spider venom (latrotoxins) |
|
|
Inhibits neurotransmitter storage |
Blocks vesicular NE uptake |
Reserpine |
|
Blocks vesicular ACh uptake |
Vesamicol |
|
|
Inhibits neuronal reuptake |
Blocks NE reuptake pump |
Imipramine Cocaine |
|
Inhibits neurotransmitter metabolism |
Inhibits NE catabolism |
Pargyline (inhibits MAO) Tolcapone (inhibits COMT) |
|
Inhibits ACh hydrolysis by inhibiting AChE |
Pyridostigmine Rivastigmine |
|
|
Stimulates autonomic receptors |
Stimulates adrenergic receptors |
Phenylephrine (α1) Clonidine (α2) Isoproterenol (β) Dobutamine (β1) Terbutaline (β2) |
|
Stimulates cholinergic receptors |
Muscarine (muscarinic) Bethanechol (muscarinic) Nicotine (nicotinic) Carbachol (nicotinic) |
|
|
Blocks autonomic receptors |
Blocks adrenergic receptors |
Phentolamine (α1 and α2) Prazosin (α1) Yohimbine (α2) Propranolol (β1 and β2) |
|
Blocks cholinergic receptors |
Atropine (muscarinic) Hexamethonium (nicotinic) |
Drugs that Inhibit Neurotransmitter Synthesis
Several enzymes in the biosynthesis of NE and Epi from tyrosine may be inhibited. Tyrosine hydroxylase, the rate-limiting enzyme, is inhibited by α-methyltyrosine; l-aromatic amino acid decarboxylase is inhibited by carbidopa, which is used for the treatment of Parkinson’s disease (see Chapter 28); and α-methyldopa, which is also a substrate for the decarboxylase, converting it to α-methyl-DA and α-methyl-NE, the latter a selective α2 adrenergic receptor agonist. Fusaric acid is a selective inhibitor of dopamine-β-hydroxylase and significantly reduces NE concentrations. In the adrenal medulla, phenylethanolamine-N-methyltransferase catalyzes the formation of Epi and can be inhibited by agents such as 2,3-dichloro-α-methylbenzylamine.
Although ACh is synthesized by the acetylation of choline through the action choline acetyltransferase, no potent and specific inhibitors of this enzyme are available. However, the biosynthesis of ACh can be inhibited with hemicholinium-3, which blocks the high-affinity transport of choline that provides substrate for ACh synthesis. This results in depletion of ACh in cholinergic neurons.
Drugs that Inhibit Neurotransmitter Release
The exocytotic release of NE from postganglionic sympathetic nerve terminals is inhibited by bretylium and guanethidine. These compounds are classified as adrenergic neuronal blocking agents.
The exocytotic release of ACh from all types of cholinergic nerve fibers is inhibited by botulinum toxin. Because of the essential role of the cholinergic nervous system (particularly in controlling the muscles of respiration), this toxin is lethal when administered systemically.
Drugs that Promote Neurotransmitter Release
NE release from postganglionic sympathetic nerve terminals can be increased either directly or indirectly. Nicotine directly stimulates nicotinic cholinergic receptors at sympathetic ganglia, propagating action potentials down postganglionic sympathetic fibers and releasing NE. Alternatively, the indirect acting sympathomimetics tyramine, ephedrine, and amphetamine cause an increase in the presynaptic release of NE. These compounds are taken up by sympathetic nerve terminals and displace NE from the vesicles. The increased cytosolic NE is transported into the synaptic cleft by reversal of the uptake1transporter. This release mechanism does not occur by exocytosis and is not Ca++-dependent.
The release of ACh from postganglionic cholinergic nerve terminals can also be evoked by activation of ganglionic nicotinic cholinergic receptors by nicotine. In addition, black widow spider venom contains latrotoxins, which have been shown to promote the exocytotic release of ACh.
Drugs that Interfere with Neurotransmitter Storage
Both ACh and NE are transported from the cytoplasm into storage vesicles by specific energy-dependent pumps located in the vesicle membrane. The uptake of NE into vesicles is inhibited by reserpine, thereby decreasing the amount of NE available for release, and can lead to complete depletion of catecholamines from postganglionic sympathetic nerve terminals. The uptake of ACh into vesicles is inhibited by vesamicol, a compound with no identified therapeutic action.
Drugs that Affect the Duration of Action of Neurotransmitter
After the exocytotic release of NE from postganglionic sympathetic nerve terminals, most of the released catecholamine is actively reaccumulated in the nerve terminal by uptake1, a process that represents the primary mechanism terminating the action of NE. Agents such as imipramine and cocaine block this uptake pump, thereby increasing synaptic concentrations of NE and enhancing adrenergic neurotransmission. Enzymes involved in the metabolism of the catecholamines (see Fig. 9-9) may also be inhibited, resulting in higher concentrations of NE in peripheral tissues. MAO is inhibited by pargyline, a compound used for the treatment of major depression (see Chapter 30), and COMT is inhibited by tolcapone, an agent used for the treatment of Parkinson’s disease (see Chapter 28).
The action of ACh at synapses is terminated by its hydrolysis by the enzyme AChE. By inhibiting AChE, the hydrolysis of ACh is prevented, increasing the magnitude and duration of effects elicited by stimulation of cholinergic neurons. Numerous compounds inhibit AChE, including agents such as edrophonium and pyridostigmine, which are used for the diagnosis and treatment of myasthenia gravis (seeChapter 10), and donepezil and rivastigmine, which are used for the treatment of Alzheimer’s disease (see Chapter 28).
Drugs that Stimulate Autonomic Receptors
NE activates three adrenergic receptor subtypes (α1, α2, and β1) as well as β3 receptors in fat cells; it is much less potent at β2 receptors. Epi, however, activates all adrenergic receptor subtypes with a similar potency. Phenylephrine is a selective α1 receptor agonist, and clonidine is a selective α2 receptor agonist. Isoproterenol is selective for β receptors and is equally effective at stimulating all β receptor subtypes; it does not stimulate α1 or α2 receptors. Dobutamine is a selective β1 receptor agonist, whereas terbutaline is a selective β2 receptor agonist.
ACh activates all subtypes of muscarinic and nicotinic cholinergic receptors. Muscarinic receptors are stimulated selectively by the alkaloid muscarine or by synthetic agonists such as bethanechol. Nicotinic receptors are stimulated by the alkaloids nicotine and epibatidine and by the cholinomimetic carbachol (see Chapter 10).
Drugs that Block Autonomic Receptors
The prototypical α adrenergic receptor blocker phentolamine is an antagonist at both α1 and α2 receptors. Prazosin is a selective antagonist at α1 receptors, whereas yohimbine blocks α2 receptors with relatively high selectivity. Prototypical β adrenergic receptor antagonists such as propranolol block both β1 and β2 adrenergic receptors. More selective β adrenergic receptor antagonists have been developed for the treatment of a variety of cardiovascular disorders and include metoprolol, a relatively selective β1 adrenergic receptor antagonist.
Most effector organs of the ANS that contain muscarinic cholinergic receptors are blocked in a competitive manner by atropine. Nicotinic cholinergic receptors in autonomic ganglia are selectively inhibited by hexamethonium.
New Horizons
With the sequencing of the human genome essentially complete, a major focus of research currently centers on defining polymorphisms in proteins involved in autonomic processes (enzymes, receptors, and transporters). Pharmacogenomic differences in both cholinergic and noradrenergic systems have been observed including both muscarinic and adrenergic receptor variants. Single nucleotide polymorphisms are associated with certain abnormal phenotypes (e.g., cardiovascular abnormalities). However, critical genetic determinants and their role in human pathophysiology and pharmacology remain to be established.
FURTHER READING
Eisenhofer G, Irwin J, Kopin IJ, et al. Catecholamine metabolism: A contemporary view with implications for physiology and medicine. Pharmacol Rev. 2004;56:331-349.
Kirstein SL, Insel PA. Autonomic nervous system pharmacogenomics: A progress report. Pharmacol Rev. 2004;56(1):31-52.
Small KM, McGraw DW, Liggett SB. Pharmacology and physiology of human adrenergic receptor polymorphisms. Annu Rev Pharmacol Toxicol. 2003;43:381-411.
Wess J. Allosteric binding sites on muscarinic acetylcholine receptors. Mol Pharmacol. 2005;68(6):1506-1509.
Zimmerman G, Soreq H. Termination and beyond: Acetylcholinesterase as a modulator of synaptic transmission. Cell Tissue Res. 2006;326(2):655-669.
SELF-ASSESSMENT QUESTIONS
1. Which one of the following is a characteristic of the parasympathetic nervous system?
A. NE is the neurotransmitter at parasympathetic ganglia.
B. ACh is the neurotransmitter for preganglionic neurotransmission.
C. The postganglionic neurons are long and myelinated.
D. Cell bodies for preganglionic neurons originate in the lumbar and thoracic regions of the spinal cord.
E. Parasympathetic neurons innervating the respiratory system mediate bronchodilation.
2. The sympathetic nervous system is characterized by which one of the following?
A. Cell bodies for preganglionic sympathetic neurons originate in the brain.
B. The neurotransmitter for postganglionic sympathetic neurons is NE.
C. Postganglionic sympathetic neurons are short.
D. Postganglionic sympathetic nerve terminals have an active uptake process that is specific for dopamine.
E. Nicotinic cholinergic receptors are not present at the paravertebral ganglia.
3. Which one of the following autonomic receptors are ligand-gated ion channels?
A. Nicotinic
B. Muscarinic
C. α1 adrenergic receptor
D. α2 adrenergic receptor
E. β1 adrenergic receptor
4. Stimulation of prejunctional or presynaptic α2 adrenergic receptors on postganglionic sympathetic neurons causes the following:
A. Inhibition of ACh release
B. Stimulation of Epi release
C. Stimulation of NE release
D. Inhibition of NE release
E. Has no effect on neurotransmitter release
5. Which of the following signal transduction processes is involved in synthesis of adrenergic agonists?
A. Adenylyl cyclase
B. Diacylglycerol
C. Phospholipase C
D. Phenylethanolamine-N-methyltransferase
E. cAMP
6. Activation of the parasympathetic nervous system results in which of the following responses?
A. An increase in heart rate
B. Vasoconstriction
C. Bronchoconstriction
D. Renin secretion
E. Relaxation of the GI tract