OBJECTIVES
After studying this chapter, you should be able to:
![]() Name the key hormones secreted by Leydig cells and Sertoli cells of the testes and by Graafian follicles and corpora lutea of the ovaries.
Name the key hormones secreted by Leydig cells and Sertoli cells of the testes and by Graafian follicles and corpora lutea of the ovaries.
![]() Outline the role of chromosomes, hormones, and related factors in sex determination and development.
Outline the role of chromosomes, hormones, and related factors in sex determination and development.
![]() Summarize the hormonal changes that occur at puberty in males and females.
Summarize the hormonal changes that occur at puberty in males and females.
![]() Outline the hormonal changes and their physiologic effects during perimenopause and menopause.
Outline the hormonal changes and their physiologic effects during perimenopause and menopause.
![]() Describe the physiologic changes that occur in the female reproductive organs during the menstrual cycle.
Describe the physiologic changes that occur in the female reproductive organs during the menstrual cycle.
![]() Know the general structures of 17β-estradiol and progesterone, and describe their biosynthesis, transport, metabolism, and actions.
Know the general structures of 17β-estradiol and progesterone, and describe their biosynthesis, transport, metabolism, and actions.
![]() Describe the roles of the pituitary and the hypothalamus in the regulation of ovarian function, and the role of feedback loops in this process.
Describe the roles of the pituitary and the hypothalamus in the regulation of ovarian function, and the role of feedback loops in this process.
![]() Describe the hormonal changes that accompany pregnancy and parturition.
Describe the hormonal changes that accompany pregnancy and parturition.
![]() Outline the processes involved in lactation.
Outline the processes involved in lactation.
INTRODUCTION
Modern genetics and experimental embryology make it clear that, in most species of mammals, the multiple differences between the male and the female depend primarily on a single chromosome (the Y chromosome) and a single pair of endocrine structures, namely the testes in the male and the ovaries in the female. The differentiation of the primitive gonads into testes or ovaries in utero is genetically determined in humans, but the formation of male genitalia depends on the presence of a functional, secreting testis; in the absence of testicular tissue, development is female. Evidence indicates that male sexual behavior and, in some species, the male pattern of gonadotropin secretion are due to the action of male hormones on the brain in early development. After birth, the gonads remain quiescent until adolescence, when they are activated by gonadotropins from the anterior pituitary. Hormones secreted by the gonads at this time cause the appearance of features typical of the adult male or female and the onset of the sexual cycle in the female. In human females, ovarian function regresses after a number of years and sexual cycles cease (the menopause). In males, gonadal function slowly declines with advancing age, but the ability to produce viable gametes persists.
In both sexes, the gonads have a dual function: the production of germ cells (gametogenesis) and the secretion of sex hormones. The androgens are steroid sex hormones that are masculinizing in their action; the estrogens are those that are feminizing. Both types of hormones are normally secreted in both sexes. The ovaries secrete large amounts of estrogens and small amounts of androgens, a pattern that is reversed in males. Androgens are secreted from the adrenal cortex in both sexes, and some of the androgens are converted to estrogens in fat and other extragonadal and extra-adrenal tissues. The ovaries also secrete progesterone, a steroid that has special functions in preparing the uterus for pregnancy.
Particularly during pregnancy, the ovaries secrete the polypeptide hormone relaxin, which loosens the ligaments of the pubic symphysis and softens the cervix, facilitating delivery of the fetus. In both sexes, the gonads secrete other polypeptides, including inhibin B, a polypeptide that inhibits follicle-stimulating hormone (FSH) secretion.
The secretory and gametogenic functions of the gonads are both dependent on the secretion of the anterior pituitary gonadotropins, FSH, and luteinizing hormone (LH). The sex hormones and inhibin B feed back to inhibit gonadotropin secretion. In males, gonadotropin secretion is noncyclic; but in postpubertal females an orderly, sequential secretion of gonadotropins is necessary for the occurrence of menstruation, pregnancy, and lactation.
SEX DIFFERENTIATION & DEVELOPMENT
CHROMOSOMAL SEX
The Sex Chromosomes
Sex is determined genetically by two chromosomes, called the sex chromosomes, to distinguish them from the somatic chromosomes (autosomes). In humans and many other mammals, the sex chromosomes are called X and Y. The Y chromosome is necessary and sufficient for the production of testes, and the testis-determining gene product is called SRY (for sex-determining region of the Y chromosome). SRY is a DNA-binding regulatory protein. It bends the DNA and acts as a transcription factor that initiates transcription of a cascade of genes necessary for testicular differentiation, including the gene for müllerian inhibiting substance (MIS; see below). The gene for SRY is located near the tip of the short arm of the human Y chromosome. Diploid male cells contain an X and a Y chromosome (XY pattern), whereas female cells contain two X chromosomes (XX pattern). As a consequence of meiosis during gametogenesis, each normal ovum contains a single X chromosome, but half of the normal sperm contain an X chromosome and half contain a Y chromosome (Figure 22–1). When a sperm containing a Y chromosome fertilizes an ovum, an XY pattern results and the zygote develops into a genetic male. When fertilization occurs with an X-containing sperm, an XX pattern and a genetic female results. Cell division and the chemical nature of chromosomes are discussed in Chapter 1.
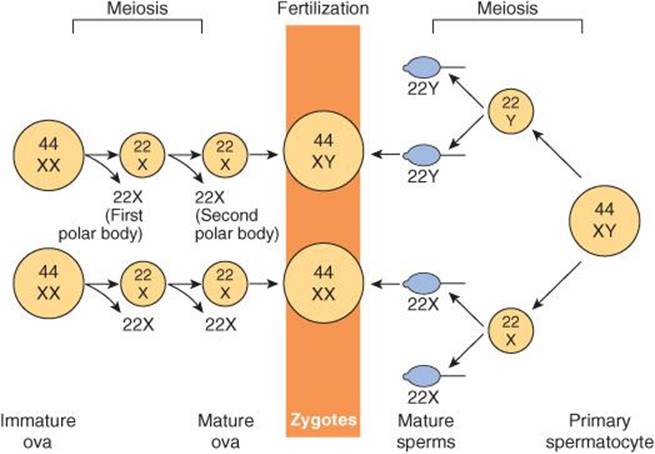
FIGURE 22–1 Basis of genetic sex determination. In the two-stage meiotic division in the female, only one cell survives as the mature ovum. In the male, the meiotic division results in the formation of four sperms, two containing the X and two the Y chromosome. Fertilization thus produces a male zygote with 22 pairs of autosomes plus an X and a Y or a female zygote with 22 pairs of autosomes and two X chromosomes. Note that for clarity, this figure and Figures 25–6 and 25–7 differ from the current international nomenclature for karyotypes, which lists the total number of chromosomes followed by the sex chromosome pattern. Thus, XO is 45, X; XY is 46, XY; XXY is 47, XXY, and so on.
Human Chromosomes
Human chromosomes can be studied in detail. Human cells are grown in tissue culture; treated with the drug colchicine, which arrests mitosis at the metaphase; exposed to a hypotonic solution that makes the chromosomes swell and disperse; and then “squashed” onto slides. Staining techniques make it possible to identify the individual chromosomes (Figure 22–2). There are 46 chromosomes: in males, 22 pairs of autosomes plus an X chromosome and a Y chromosome; in females, 22 pairs of autosomes plus two X chromosomes. The individual chromosomes are usually arranged in an arbitrary pattern (karyotype). The individual autosome pairs are identified by the numbers 1–22 on the basis of their morphologic characteristics.
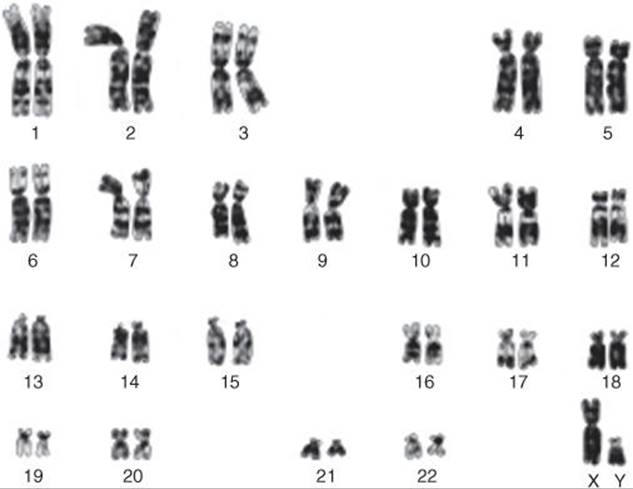
FIGURE 22–2 Karyotype of chromosomes from a normal male. The chromosomes have been stained with Giemsa’s stain, which produces a characteristic banding pattern. (Reproduced with permission, from Lingappa VJ, Farey K: Physiological Medicine. McGraw-Hill, 2000.)
Sex Chromatin
Soon after cell division has started during embryonic development, one of the two X chromosomes of the somatic cells in normal females becomes functionally inactive. In abnormal individuals with more than two X chromosomes, only one remains active. The process that is normally responsible for inactivation is initiated in an X-inactivation center in the chromosome, probably via the transactivating factor CTCF (for CCCTC-binding factor), which is also induced during gene imprinting. However, the details of the inactivation process are still incompletely understood. The choice of which X chromosome remains active is random, so normally one X chromosome remains active in approximately half of the cells and the other X chromosome is active in the other half. The selection persists through subsequent divisions of these cells, and consequently some of the somatic cells in adult females contain an active X chromosome of paternal origin and some contain an active X chromosome of maternal origin.
In normal cells, the inactive X chromosome condenses and can be seen in various types of cells, usually near the nuclear membrane, as the Barr body, also called sex chromatin (Figure 22–3). Thus, there is a Barr body for each X chromosome in excess of one in the cell. The inactive X chromosome is also visible as a small “drumstick” of chromatin projecting from the nuclei of 1–15% of the polymorphonuclear leukocytes in females but not in males (Figure 22–3).
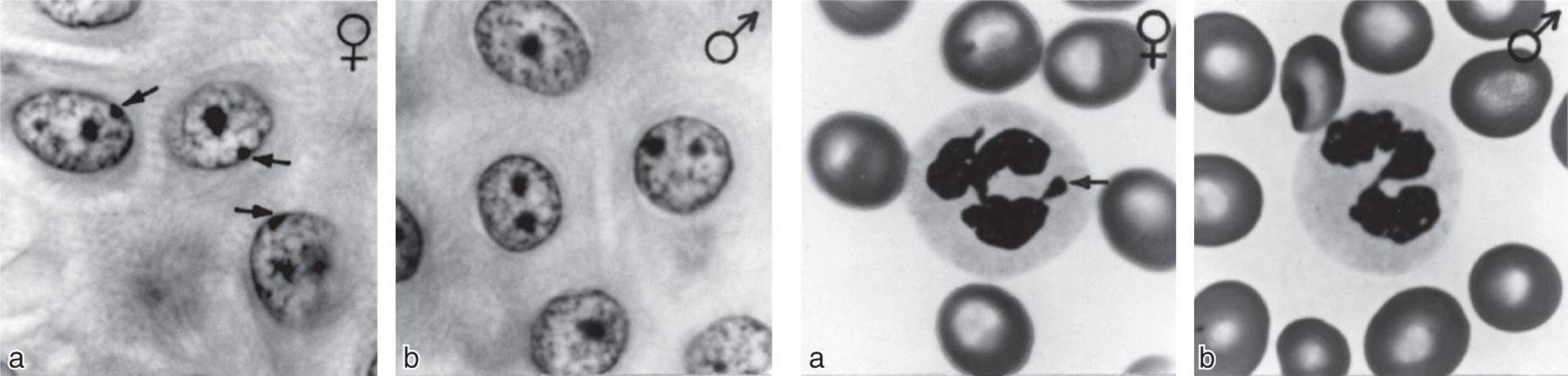
FIGURE 22–3 Left: Barr body (arrows) in the epidermal spinous cell layer. Right: Nuclear appendage (“drumstick”) identified by arrow in white blood cells. (Reproduced with permission from Grumbach MM, Barr ML: Cytologic tests of chromosomal sex in relation to sex anomalies in man. Recent Prog Horm Res 1958;14:255.)
EMBRYOLOGY OF THE HUMAN REPRODUCTIVE SYSTEM
Development of the Gonads
On each side of the embryo, a primitive gonad arises from the genital ridge, a condensation of tissue near the adrenal gland. The gonad develops a cortex and a medulla. Until the 6th week of development, these structures are identical in both sexes. In genetic males, the medulla develops during the 7th and 8th weeks into a testis, and the cortex regresses. Leydig and Sertoli cells appear, and testosterone and MIS are secreted. In genetic females, the cortex develops into an ovary and the medulla regresses. The embryonic ovary does not secrete hormones. Hormonal treatment of the mother has no effect on gonadal (as opposed to ductal and genital) differentiation in humans, although it does in some experimental animals.
Embryology of the Genitalia
The embryology of the gonads is summarized in Figures 22–4 and 22–5. In the 7th week of gestation, the embryo has both male and female primordial genital ducts (Figure 22–4). In a normal female fetus, the müllerian duct system then develops into uterine tubes (oviducts) and a uterus. In the normal male fetus, the wolffian duct system on each side develops into the epididymis and vas deferens. The external genitalia are similarly bipotential until the 8th week (Figure 22–5). Thereafter, the urogenital slit disappears and male genitalia form, or, alternatively, it remains open and female genitalia form.
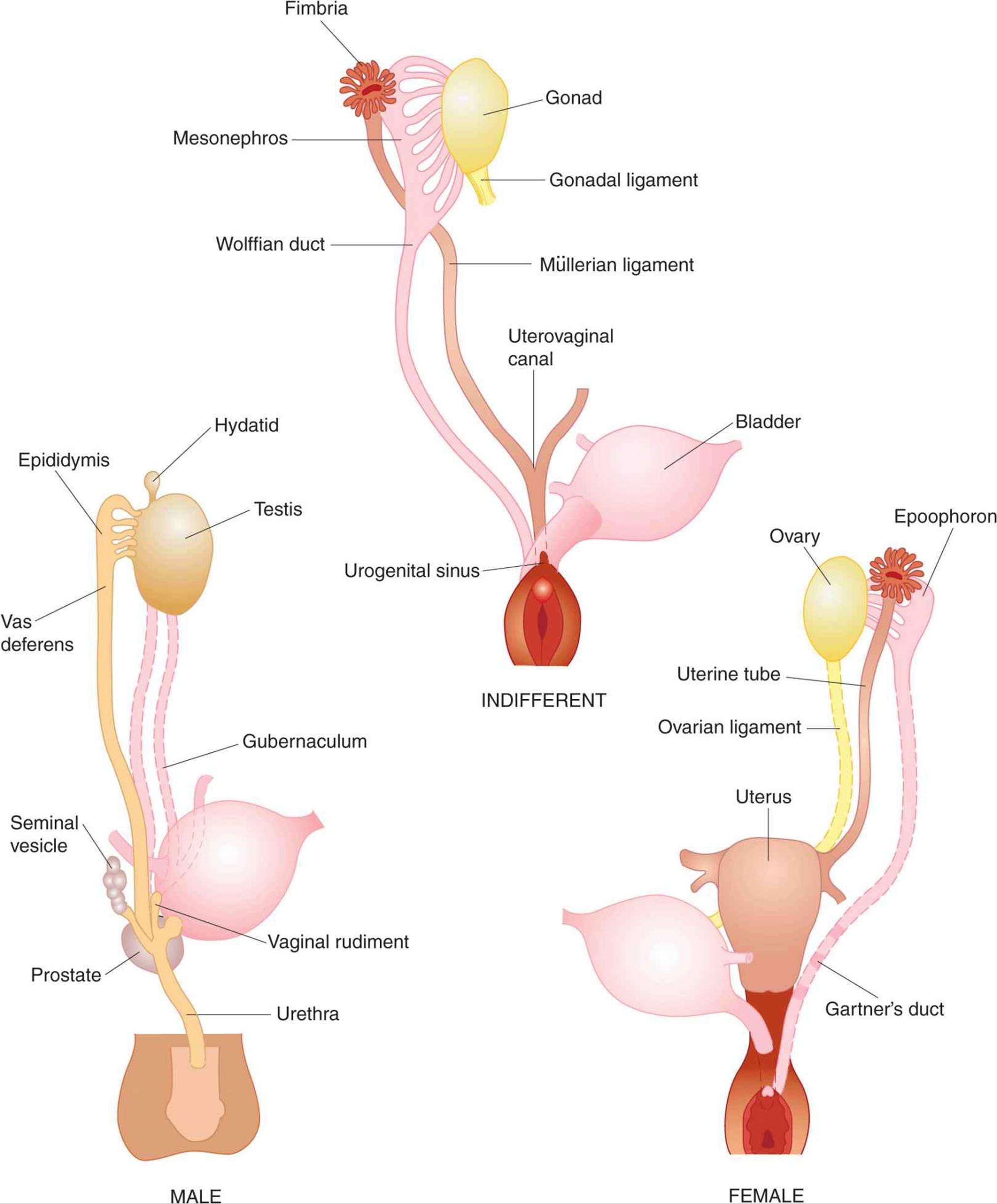
FIGURE 22–4 Embryonic differentiation of male and female internal genitalia (genital ducts) from wolffian (male) and müllerian (female) primordia. (After Corning HK, Wilkins L. Redrawn and reproduced with permission from Williams Textbook of Endocrinology, 7th ed. Wilson JD, Foster DW [editors]. Saunders, 1985.)
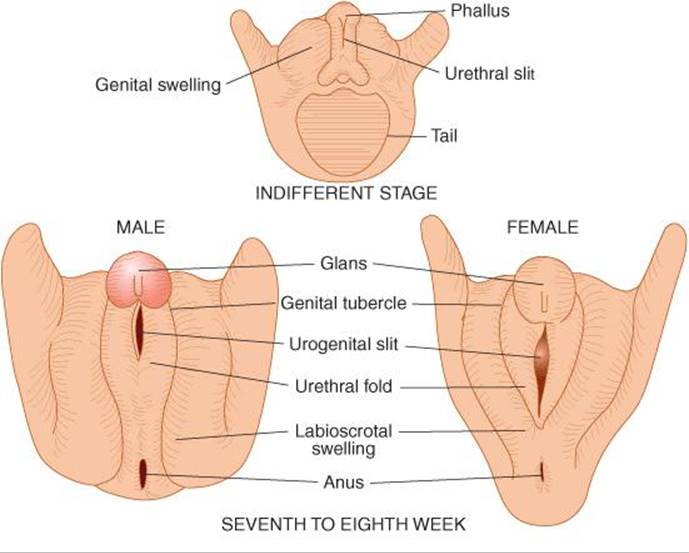
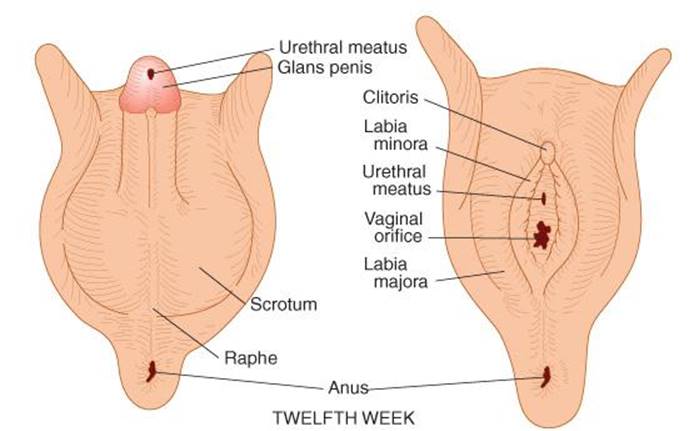
FIGURE 22–5 Differentiation of male and female external genitalia from indifferent primordial structures in the embryo.
When the embryo has functional testes, male internal and external genitalia develop. The Leydig cells of the fetal testis secrete testosterone, and the Sertoli cells secrete MIS (also called müllerian regression factor, or MRF). MIS is a 536-amino-acid homodimer that is a member of the transforming growth factor β (TGF-β) super-family of growth factors, which includes inhibins and activins.
In their effects on the internal as opposed to the external genitalia, MIS and testosterone act unilaterally. MIS causes regression of the müllerian ducts by apoptosis on the side on which it is secreted, and testosterone fosters the development of the vas deferens and related structures from the wolffian ducts. The testosterone metabolite dihydrotestosterone induces the formation of male external genitalia and male secondary sex characteristics (Figure 22–6).
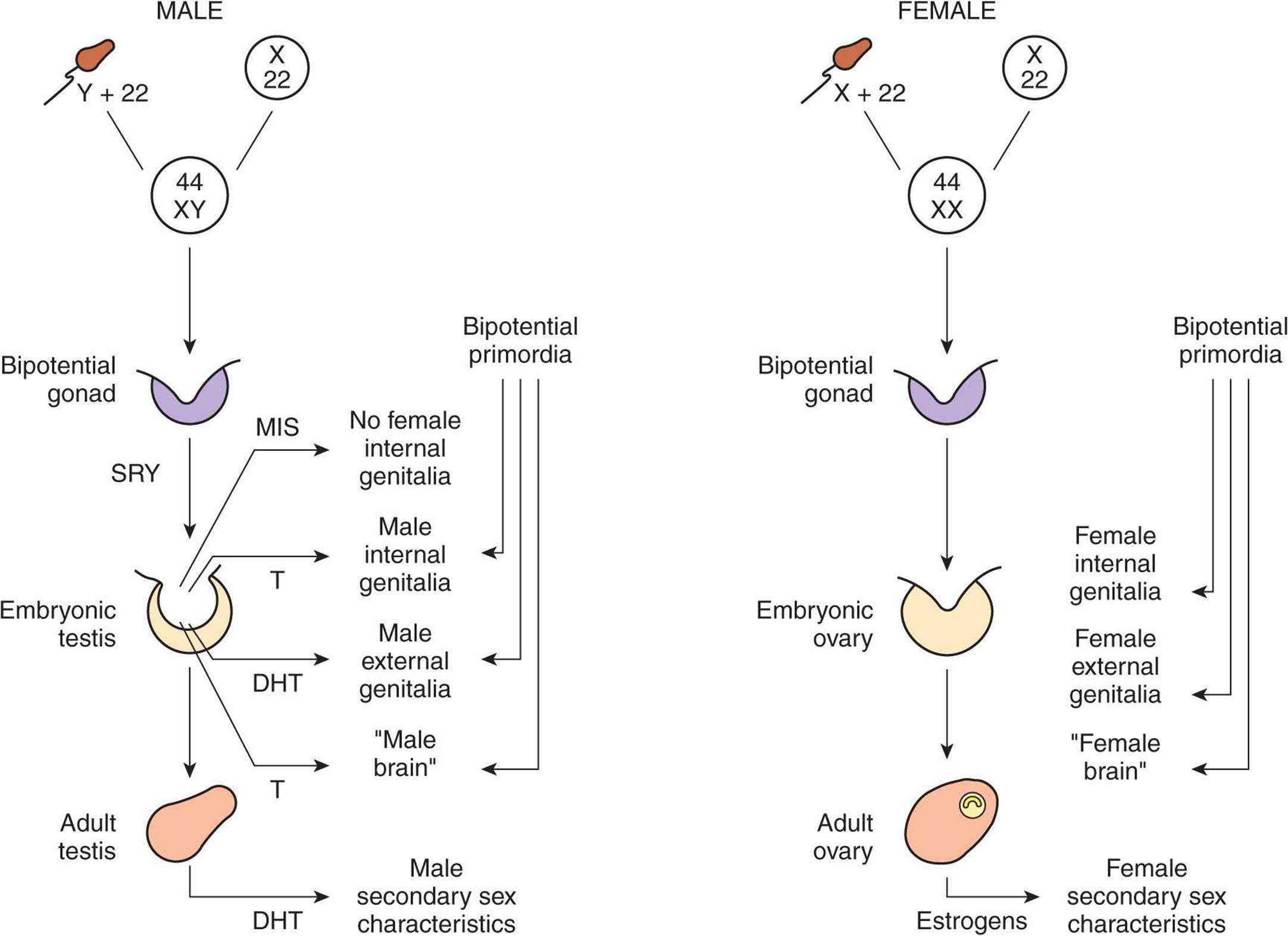
FIGURE 22–6 Diagrammatic summary of normal sex determination, differentiation, and development in humans. DHT, dihydrotestosterone, MIS, müllerian inhibiting substance; T, testosterone.
MIS continues to be secreted by the Sertoli cells, and it reaches mean values of 48 ng/mL in plasma in 1- to 2-year-old boys. Thereafter, it declines to low levels by the time of puberty and persists at low but detectable levels throughout life. In girls, MIS is produced by granulosa cells in small follicles in the ovaries, but plasma levels are very low or undetectable until puberty. Thereafter, plasma MIS is about the same as in adult men, that is, about 2 ng/mL. The functions of MIS after early embryonic life are unsettled, but it is probably involved in germ cell maturation in both sexes and in control of testicular descent in boys.
Development of the Brain
At least in some species, the development of the brain as well as the external genitalia is affected by androgens early in life. In rats, a brief exposure to androgens during the first few days of life causes the male pattern of sexual behavior and the male pattern of hypothalamic control of gonadotropin secretion to develop after puberty. In the absence of androgens, female patterns develop (see Chapter 17). In monkeys, similar effects on sexual behavior are produced by exposure to androgens in utero, but the pattern of gonadotropin secretion remains cyclical. Early exposure of female human fetuses to androgens also appears to cause subtle but significant masculinizing effects on behavior. However, women with adrenogenital syndrome due to congenital adrenocortical enzyme deficiency (see Chapter 20) develop normal menstrual cycles when treated with cortisol. Thus, the human, like the monkey, appears to retain the cyclical pattern of gonadotropin secretion despite exposure to androgens in utero.
ABERRANT SEXUAL DIFFERENTIATION
Chromosomal Abnormalities
From the preceding discussion, it might be expected that abnormalities of sexual development could be caused by genetic or hormonal abnormalities as well as by other nonspecific teratogenic influences, and this is indeed the case. The major classes of abnormalities are listed in Table 22–1.
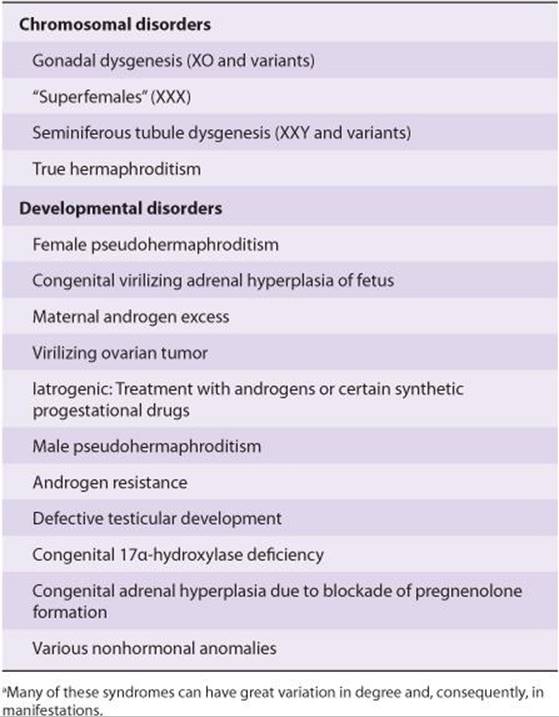
TABLE 22–1 Classification of the major disorders of sex differentiation in humans.a
Nondisjunction of sex chromosomes during the first division in meiosis results in distinct defects (see Clinical Box 22–1; Figure 22–7). Meiosis is a two-stage process, and although nondisjunction usually occurs during the first meiotic division, it can occur in the second, producing more complex chromosomal abnormalities. In addition, nondisjunction or simple loss of a sex chromosome can occur during the early mitotic divisions after fertilization. The consequence of faulty mitoses in the early zygote is mosaicism, in which two or more populations of cells have different chromosome complements. True hermaphroditism, the condition in which the individual has both ovaries and testes, is probably due to XX/XY mosaicism and related mosaic patterns, although other genetic aberrations are possible.
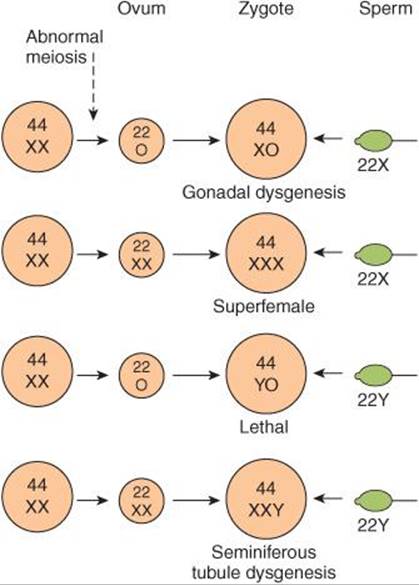
FIGURE 22–7 Summary of four possible defects produced by maternal nondisjunction of the sex chromosomes at the time of meiosis. The YO combination is believed to be lethal, and the fetus dies in utero.
CLINICAL BOX 22–1
Chromosomal Abnormalities
An established defect in gametogenesis is nondisjunction, a phenomenon in which a pair of chromosomes fail to separate, so that both go to one of the daughter cells during meiosis. Four of the abnormal zygotes that can form as a result of nondisjunction of one of the X chromosomes during oogenesis are shown in Figure 25–7. In individuals with the XO chromosomal pattern, the gonads are rudimentary or absent, so that female external genitalia develop, stature is short, other congenital abnormalities are often present, and no sexual maturation occurs at puberty. This syndrome is called gonadal dysgenesis or, alternatively, ovarian agenesis or Turner syndrome. Individuals with the XXY pattern, the most common sex chromosome disorder, have the genitalia of a normal male. Testosterone secretion at puberty is often great enough for the development of male characteristics; however, the seminiferous tubules are abnormal, and the incidence of mental retardation is higher than normal. This syndrome is known as seminiferous tubule dysgenesis or Klinefelter syndrome. The XXX (“superfemale”) pattern is second in frequency only to the XXY pattern and may be even more common in the general population, since it does not seem to be associated with any characteristic abnormalities. The YO combination is probably lethal.
Nondisjunction of chromosome 21 produces trisomy 21, the chromosomal abnormality associated with Down syndrome (mongolism). The additional chromosome 21 is normal, so Down syndrome is a pure case of gene excess causing abnormalities.
Many other chromosomal abnormalities occur as well as numerous diseases due to defects in single genes. These conditions are generally diagnosed in utero by analysis of fetal cells in a sample of amniotic fluid collected by inserting a needle through the abdominal wall (amniocentesis) or, earlier in pregnancy, by examining fetal cells obtained by a needle biopsy of chorionic villi (chorionic villus sampling).
THERAPEUTIC HIGHLIGHTS
Many of the syndromes mentioned have effects on multiple organ systems, and patients must be carefully followed with a multidisciplinary approach to avert the consequences of cardiovascular defects, infections secondary to urinary tract and renal malformations, and the psychological impact of reproductive implications. Girls with Turner syndrome and evidence of gonadal failure are also treated with low dose estrogen to evoke puberty, followed by gradual replacement of mature estrogen levels to permit feminization. Conversely, patients with Klinefelter syndrome are often supplemented with androgens to improve virilization and libido.
Chromosomal abnormalities also include transposition of parts of chromosomes to other chromosomes. Rarely, genetic males are found to have the XX karyotype because the short arm of their father’s Y chromosome was transposed to their father’s X chromosome during meiosis and they received that X chromosome along with their mother’s. Similarly, deletion of the small portion of the Y chromosome containing SRY produces females with the XY karyotype.
Hormonal Abnormalities
Development of the male external genitalia occurs normally in genetic males in response to androgen secreted by the embryonic testes, but male genital development may also occur in genetic females exposed to androgens from some other source during the 8th to the 13th weeks of gestation. The syndrome that results is female pseudohermaphroditism. A pseudohermaphrodite is an individual with the genetic constitution and gonads of one sex and the genitalia of the other. After the 13th week, the genitalia are fully formed, but exposure to androgens can cause hypertrophy of the clitoris. Female pseudohermaphroditism may be due to congenital virilizing adrenal hyperplasia (see Chapter 20), or it may be caused by androgens administered to the mother. Conversely, one cause of the development of female external genitalia in genetic males (male pseudohermaphroditism) is defective testicular development. Because the testes also secrete MIS, genetic males with defective testes have female internal genitalia.
Another cause of male pseudohermaphroditism is androgen resistance, in which, as a result of various congenital abnormalities, male hormones cannot exert their full effects on the tissues. One form of androgen resistance is a 5α-reductase deficiency, in which the enzyme responsible for the formation of dihydrotestosterone, the active form of testosterone, is decreased (Figure 22-8). The consequences of this deficiency are discussed in Chapter 23. Other forms of androgen resistance are due to various mutations in the androgen receptor gene, and the resulting defects in receptor function range from minor to severe. Mild defects cause infertility with or without gynecomastia. When the loss of receptor function is complete, the testicular feminizing syndrome, now known as complete androgen resistance syndrome, results. In this condition, MIS is present and testosterone is secreted at normal or even elevated rates. The external genitalia are female, but the vagina ends blindly because there are no female internal genitalia. Individuals with this syndrome develop enlarged breasts at puberty and usually are considered to be normal women until they are diagnosed when they seek medical advice because of lack of menstruation.
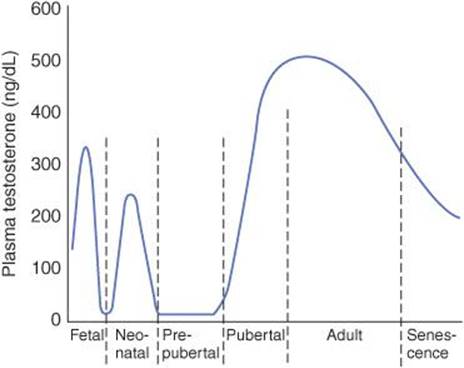
FIGURE 22–8 Plasma testosterone levels at various ages in human males.
It is worth noting that genetic males with congenital blockage of the formation of pregnenolone are pseudohermaphrodites because testicular as well as adrenal androgens are normally formed from pregnenolone. Male pseudohermaphroditism also occurs when there is a congenital deficiency of 17α-hydroxylase (see Chapter 20).
PUBERTY
As noted above, a burst of testosterone secretion occurs in male fetuses before birth (see Chapter 23). In the neonatal period there is another burst, with unknown function, but thereafter the Leydig cells become quiescent. There follows in all mammals a period in which the gonads of both sexes are quiescent until they are activated by gonadotropins from the pituitary to bring about the final maturation of the reproductive system. This period of final maturation is known as adolescence. It is often also called puberty, although puberty, strictly defined, is the period when the endocrine and gametogenic functions of the gonads have first developed to the point where reproduction is possible. In girls, the first event is thelarche, the development of breasts, followed by pubarche, the development of axillary and pubic hair, and then by menarche, the first menstrual period. Initial menstrual periods are generally anovulatory, and regular ovulation appears about a year later. In contrast to the situation in adulthood, removal of the gonads during the period from soon after birth to puberty causes only a small increase in gonadotropin secretion, so gonadotropin secretion is not being held in check by the gonadal hormones. In children between the ages of 7 and 10, a slow increase in estrogen and androgen secretion precedes the more rapid rise in the early teens (Figure 22–9).
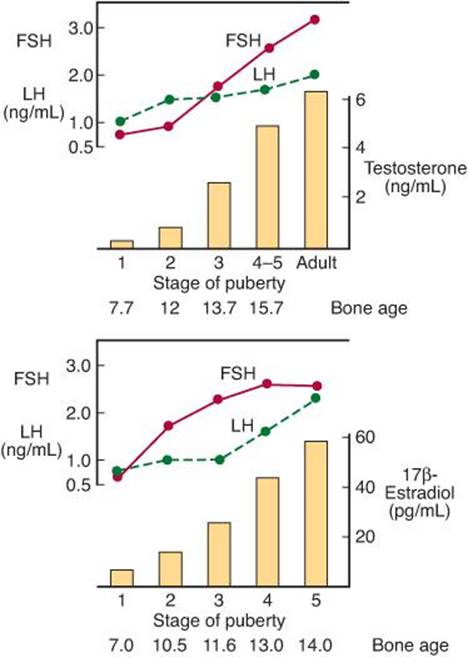
FIGURE 22–9 Changes in plasma hormone concentrations during puberty in boys (top) and girls (bottom). Stage 1 of puberty is preadolescence in both sexes. In boys, stage 2 is characterized by beginning enlargement of the testes, stage 3 by penile enlargement, stage 4 by growth of the glans penis, and stage 5 by adult genitalia. In girls, stage 2 is characterized by breast buds, stage 3 by elevation and enlargement of the breasts, stage 4 by projection of the areolas, and stage 5 by adult breasts. (Modified and reproduced with permission from Berenberg SR [editor]: Puberty: Biologic and Psychosocial Components. HE Stenfoert Kroese BV, 1975.)
The age at the time of puberty is variable. In Europe and the United States, it has been declining at the rate of 1–3 months per decade for more than 175 years. In the United States in recent years, puberty generally occurs between the ages of 8 and 13 in girls and 9 and 14 in boys.
Another event that occurs in humans at the time of puberty is an increase in the secretion of adrenal androgens (see Figure 20–12). The onset of this increase is called adrenarche. It occurs at age 8–10 years in girls and age 10–12 years in boys. Dehydroepiandrosterone (DHEA) values peak at about age 25 in females and slightly later than that in males. They then decline slowly to low values in old age. The rise appears to be due to an increase in the activity of 17α-hydroxylase.
Control of the Onset of Puberty
The gonads of children can be stimulated by gonadotropins; their pituitaries contain gonadotropins and their hypothalami contain gonadotropin-releasing hormone (GnRH) (see Chapter 17). However, their gonadotropins are not secreted. In immature monkeys, normal menstrual cycles can be brought on by pulsatile injection of GnRH, and they persist as long as the pulsatile injection is continued. Thus, it seems clear that pulsatile secretion of GnRH brings on puberty. During the period from birth to puberty, a neural mechanism is operating to prevent the normal pulsatile release of GnRH. The nature of the mechanism inhibiting the GnRH pulse generator is unknown. However, one or more genes produce products that stimulate secretion of GnRH, and inhibition of these genes before puberty is an interesting possibility (see Clinical Box 22–2).
CLINICAL BOX 22–2
Leptin
It has been argued for some time that a critical body weight must normally be reached for puberty to occur. Thus, for example, young women who engage in strenuous athletics lose weight and stop menstruating, as do girls with anorexia nervosa. If these girls start to eat and gain weight, they menstruate again, that is, they “go back through puberty.” It now appears that leptin, the satiety-producing hormone secreted by fat cells, may be the link between body weight and puberty. Obese ob/ob mice that cannot make leptin are infertile, and their fertility is restored by injections of leptin. Leptin treatment also induces precocious puberty in immature female mice. However, the way that leptin fits into the overall control of puberty remains to be determined.
PRECOCIOUS & DELAYED PUBERTY
Sexual Precocity
The major causes of precocious sexual development in humans are listed in Table 22–2. Early development of secondary sexual characteristics without gametogenesis is caused by abnormal exposure of immature males to androgen or females to estrogen. This syndrome should be called precocious pseudopuberty to distinguish it from true precocious puberty due to an early but otherwise normal pubertal pattern of gonadotropin secretion from the pituitary.
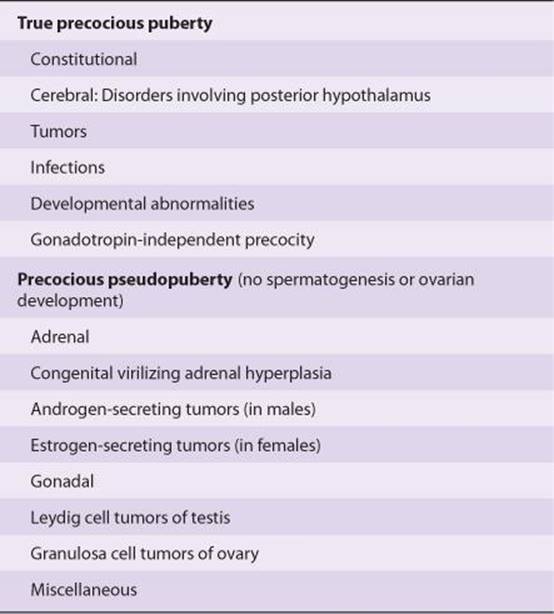
TABLE 22–2 Classification of the causes of precocious sexual development in humans.
Constitutional precocious puberty; that is, precocious puberty in which no cause can be determined, is more common in girls than in boys. In both sexes, tumors or infections involving the hypothalamus cause precocious puberty. Indeed, in one large series of cases, precocious puberty was the most common endocrine symptom of hypothalamic disease. In experimental animals, precocious puberty can be produced by hypothalamic lesions. Apparently the lesions interrupt a pathway that normally holds pulsatile GnRH secretion in check. Pineal tumors are sometimes associated with precocious puberty, but evidence indicates that these tumors are associated with precocity only when there is secondary damage to the hypothalamus.
Precocious gametogenesis and steroidogenesis can occur without the pubertal pattern of gonadotropin secretion (gonadotropin-independent precocity). At least in some cases of this condition, the sensitivity of LH receptors to gonadotropins is increased because of an activating mutation in the G protein that couples the receptors to adenylyl cyclase.
Delayed or Absent Puberty
The normal variation in the age at which adolescent changes occur is so wide that puberty cannot be considered to be pathologically delayed until the menarche has failed to occur by the age of 17 or testicular development by the age of 20. Failure of maturation due to panhypopituitarism is associated with dwarfing and evidence of other endocrine abnormalities. Patients with the XO chromosomal pattern and gonadal dysgenesis are also dwarfed. In some individuals, puberty is delayed even though the gonads are present and other endocrine functions are normal. In males, this clinical picture is called eunuchoidism. In females, it is called primary amenorrhea (see Clinical Box 22–3).
CLINICAL BOX 22–3
Hyperprolactinemia
Up to 70% of the patients with chromophobe adenomas of the anterior pituitary have elevated plasma prolactin levels. In some instances, the elevation may be due to damage to the pituitary stalk, but in most cases, the tumor cells are actually secreting the hormone. The hyperprolactinemia may cause galactorrhea, but in many individuals no demonstrable endocrine abnormalities are present. Conversely, most women with galactorrhea have normal prolactin levels; definite elevations are found in less than a third of patients with this condition.
Another interesting observation is that 15–20% of women with secondary amenorrhea have elevated prolactin levels, and when prolactin secretion is reduced, normal menstrual cycles and fertility return. Prolactin may produce amenorrhea by blocking the action of gonadotropins on the ovaries. The hypogonadism produced by prolactinomas is associated with osteoporosis due to estrogen deficiency.
As noted previously, hyperprolactinemia in men is associated with impotence and hypogonadism that disappear when prolactin secretion is reduced.
THERAPEUTIC HIGHLIGHTS
Prescription drug use is a common cause of hyperprolactinemia. Prolactin secretion in the pituitary is suppressed by the brain chemical dopamine. Use of drugs that block the effects of dopamine can cause the pituitary to secrete prolactin. Examples of some prescription drugs that can cause hyperprolactinemia include the major tranquilizers haloperidol (Haldol) and phenothiazines, most antipsychotic medications, and cisapride, which is used to treat nausea and gastro-oesophageal reflux in cancer patients. If possible, the drug suspected as causing hyperprolactinemia should be withdrawn, or the dose titrated. Regardless of the etiology, treatment should endeavor to restore normal prolactin levels to avoid suppressive effects on the ovaries and preserve bone density. Dopamine agonists also provide benefit in many cases, including prolactinoma, and can be used in patients for whom an inciting pharmaceutical agent cannot be withdrawn.
MENOPAUSE
The human ovaries become unresponsive to gonadotropins with advancing age, and their function declines, so that sexual cycles disappear (menopause). This unresponsiveness is associated with and probably caused by a decline in the number of primordial follicles, which becomes precipitous at the time of menopause (Figure 22–10). The ovaries no longer secrete progesterone and 17β-estradiol in appreciable quantities, and estrogen is formed only in small amounts by aromatization of androstenedione in peripheral tissues (see Chapter 20). The uterus and the vagina gradually become atrophic. As the negative feedback effect of estrogens and progesterone is reduced, secretion of FSH is increased, and plasma FSH increases to high levels, LH levels are moderately high. Old female mice and rats have long periods of diestrus and increased levels of gonadotropin secretion. In women, a period called perimenopause precedes menopause, and can last up to 10 years. During perimenopause FSH levels will increase before an increase in LH is observed due to a decrease in estrogen, progesterone, and inhibins and the menses become irregular. This usually occurs between the ages of 45 and 55. The average age at onset of the menopause is 52 years.
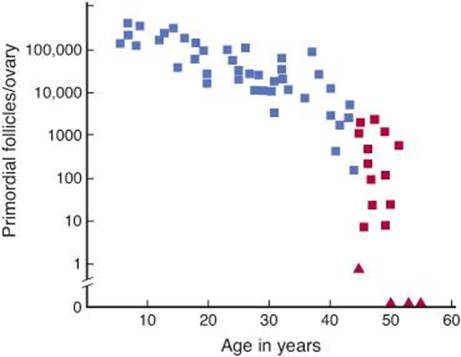
FIGURE 22–10 Number of primordial follicles per ovary in women at various ages. Blue squares, premenopausal women (regular menses); red squares, perimenopausal women (irregular menses for at least 1 year); red triangles, postmenopausal women (no menses for at least 1 year). Note that the vertical scale is a log scale and that the values are from one rather than two ovaries. (Redrawn by PM Wise and reproduced with permission from Richardson SJ, Senikas V, Nelson JF: Follicular depletion during the menopausal transition: Evidence for accelerated loss and ultimate exhaustion. J Clin Endocrinol Metab 1987;65:1231.)
The loss of ovarian function causes many symptoms such as sensations of warmth spreading from the trunk to the face (hot flushes; also called hot flashes) and night sweats. In addition, the onset of menopause increases the risk of many diseases such as osteoporosis, ischemic heart disease, and renal disease.
Hot flushes are said to occur in 75% of menopausal women and may continue intermittently for as long as 40 years. They also occur when early menopause is produced by bilateral ovariectomy, and they are prevented by estrogen treatment. In addition, they occur after castration in men. Their cause is unknown. However, they coincide with surges of LH secretion. LH is secreted in episodic bursts at intervals of 30–60 min or more (circhoral secretion), and in the absence of gonadal hormones these bursts are large. Each hot flush begins with the start of a burst. However, LH itself is not responsible for the symptoms, because they can continue after removal of the pituitary. Instead, it appears that some estrogen-sensitive event in the hypothalamus initiates both the release of LH and the episode of flushing.
Although the function of the testes tends to decline slowly with advancing age, the evidence is unclear whether there is a “male menopause” (andropause) similar to that occurring in women.
THE FEMALE REPRODUCTIVE SYSTEM
THE MENSTRUAL CYCLE
The reproductive system of women (Figure 22–11), unlike that of men, shows regular cyclic changes that teleologically may be regarded as periodic preparations for fertilization and pregnancy. In humans and other primates, the cycle is a menstrual cycle, and its most conspicuous feature is the periodic vaginal bleeding that occurs with the shedding of the uterine mucosa (menstruation). The length of the cycle is notoriously variable in women, but an average figure is 28 days from the start of one menstrual period to the start of the next. By common usage, the days of the cycle are identified by number, starting with the first day of menstruation.

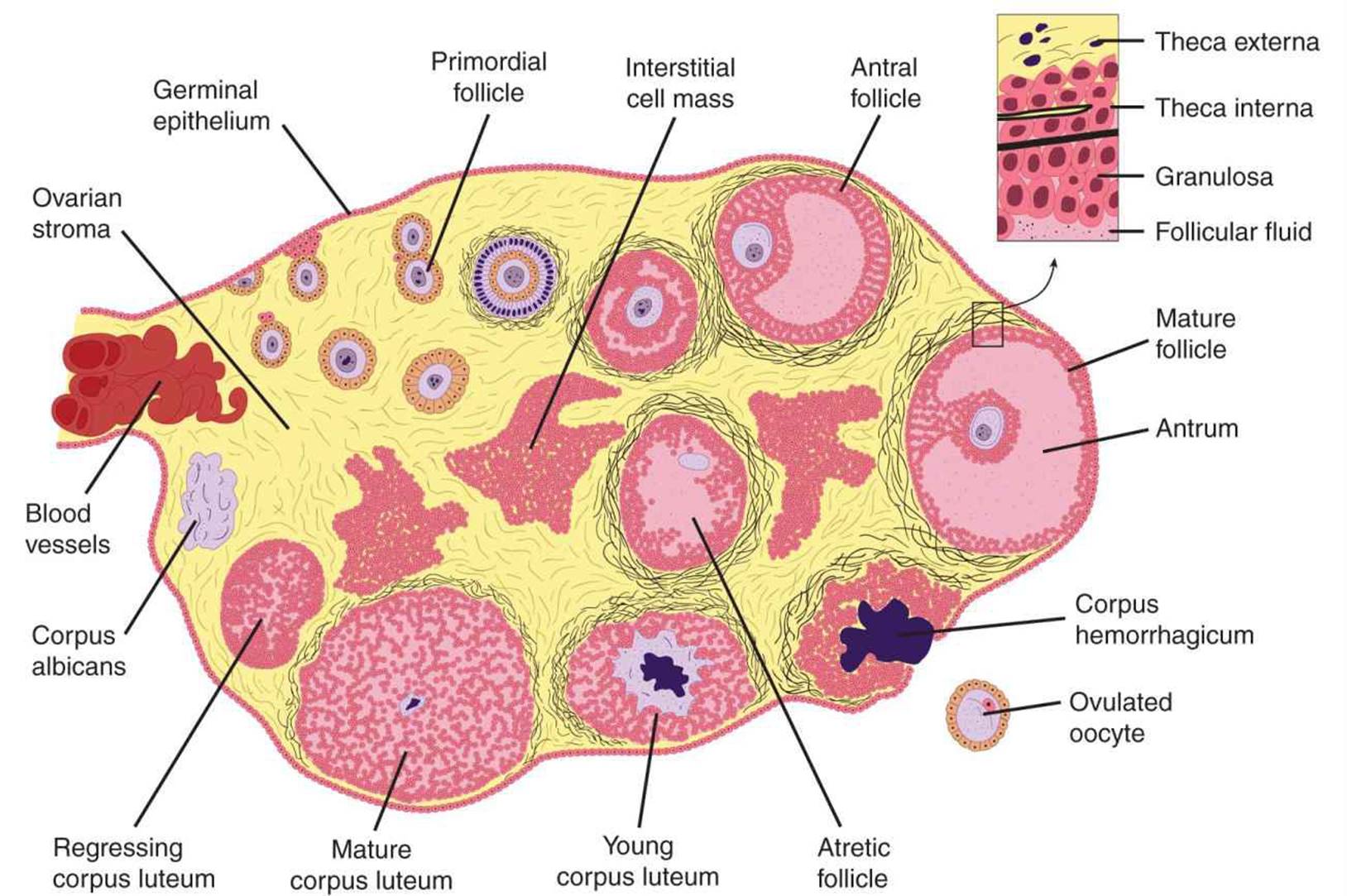
FIGURE 22–11 Functional anatomy of the female reproductive tract. The female reproductive organs include the ovaries, the uterus and the fallopian tubes, and the breast/mammary glands. The sequential development of a follicle, the formation of a corpus luteum and follicular atresia are shown.
Ovarian Cycle
From the time of birth, there are many primordial follicles under the ovarian capsule. Each contains an immature ovum (Figure 22–11). At the start of each cycle, several of these follicles enlarge, and a cavity forms around the ovum (antrum formation). This cavity is filled with follicular fluid. In humans, usually one of the follicles in one ovary starts to grow rapidly on about the 6th day and becomes the dominant follicle, while the others regress, forming atretic follicles. The atretic process involves apoptosis. It is uncertain how one follicle is selected to be the dominant follicle in this follicular phase of the menstrual cycle, but it seems to be related to the ability of the follicle to secrete the estrogen inside it that is needed for final maturation. When women are given human pituitary gonadotropin preparations by injection, many follicles develop simultaneously.
The structure of a maturing ovarian (graafian) follicle is shown in Figure 22–11. The primary source of circulating estrogen is the granulosa cells of the ovaries; however, the cells of the theca interna of the follicle are necessary for the production of estrogen as they secrete androgens that are aromatized to estrogen by the granulosa cells.
At about the 14th day of the cycle, the distended follicle ruptures, and the ovum is extruded into the abdominal cavity. This is the process of ovulation. The ovum is picked up by the fimbriated ends of the uterine tubes (oviducts). It is transported to the uterus and, unless fertilization occurs, out through the vagina.
The follicle that ruptures at the time of ovulation promptly fills with blood, forming what is sometimes called a corpus hemorrhagicum. Minor bleeding from the follicle into the abdominal cavity may cause peritoneal irritation and fleeting lower abdominal pain (“mittelschmerz”). The granulosa and theca cells of the follicle lining promptly begin to proliferate, and the clotted blood is rapidly replaced with yellowish, lipid-rich luteal cells, forming the corpus luteum. This initiates the luteal phase of the menstrual cycle, during which the luteal cells secrete estrogen and progesterone. Growth of the corpus luteum depends on its developing an adequate blood supply, and there is evidence that vascular endothelial growth factor (VEGF) (see Chapter 31) is essential for this process.
If pregnancy occurs, the corpus luteum persists and usually there are no more periods until after delivery. If pregnancy does not occur, the corpus luteum begins to degenerate about 4 days before the next menses (24th day of the cycle) and is eventually replaced by scar tissue, forming a corpus albicans.
The ovarian cycle in other mammals is similar, except that in many species more than one follicle ovulates and multiple births are the rule. Corpora lutea form in some submammalian species but not in others.
In humans, no new ova are formed after birth. During fetal development, the ovaries contain over 7 million primordial follicles. However, many undergo atresia (involution) before birth and others are lost after birth. At the time of birth, there are 2 million ova, but 50% of these are atretic. The million that are normal undergo the first part of the first meiotic division at about this time and enter a stage of arrest in prophase in which those that survive persist until adulthood. Atresia continues during development, and the number of ova in both of the ovaries at the time of puberty is less than 300,000 (Figure 22–10). Only one of these ova per cycle (or about 500 in the course of a normal reproductive life) normally reaches maturity; the remainder degenerate. Just before ovulation, the first meiotic division is completed. One of the daughter cells, the secondary oocyte, receives most of the cytoplasm, while the other, the first polar body, fragments and disappears. The secondary oocyte immediately begins the second meiotic division, but this division stops at metaphase and is completed only when a sperm penetrates the oocyte. At that time, the second polar body is cast off and the fertilized ovum proceeds to form a new individual. The arrest in metaphase is due, at least in some species, to formation in the ovum of the protein pp39mos, which is encoded by the c-mosprotooncogene. When fertilization occurs, the pp39mos is destroyed within 30 min by calpain, a calcium-dependent cysteine protease.
Uterine Cycle
At the end of menstruation, all but the deep layers of the endometrium have sloughed. A new endometrium then regrows under the influence of estrogens from the developing follicle. The endometrium increases rapidly in thickness from the 5th to the 14th days of the menstrual cycle. As the thickness increases, the uterine glands are drawn out so that they lengthen (Figure 22–12), but they do not become convoluted or secrete to any degree. These endometrial changes are called proliferative, and this part of the menstrual cycle is sometimes called the proliferative phase. It is also called the preovulatory or follicular phase of the cycle. After ovulation, the endometrium becomes more highly vascularized and slightly edematous under the influence of estrogen and progesterone from the corpus luteum. The glands become coiled and tortuous and they begin to secrete a clear fluid. Consequently, this phase of the cycle is called the secretory or luteal phase. Late in the luteal phase, the endometrium, like the anterior pituitary, produces prolactin, but the function of this endometrial prolactin is unknown.

FIGURE 22–12 Relationship between ovarian and uterine changes during the menstrual cycle. (Reproduced with permission from Windmaier EP, Raff H, Strang KT: Vander’s Human Physiology: The Mechanisms of Body Function, 11th ed. McGraw-Hill, 2008.)
The endometrium is supplied by two types of arteries. The superficial two thirds of the endometrium that is shed during menstruation, the stratum functionale, is supplied by long, coiled spiral arteries (Figure 22–13), whereas the deep layer that is not shed, the stratum basale, is supplied by short, straight basilar arteries.
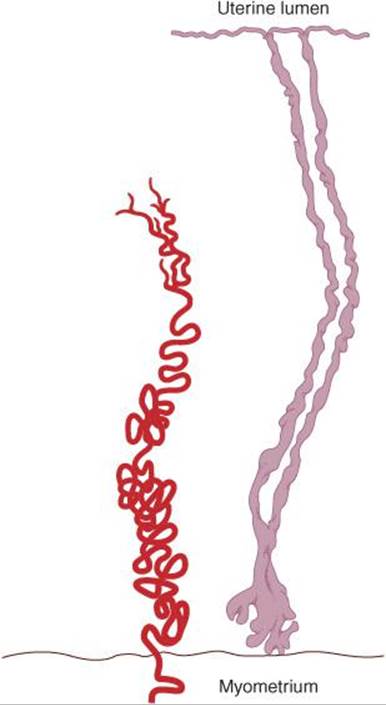
FIGURE 22–13 Spiral artery of endometrium. Drawing of a spiral artery (left) and two uterine glands (right) from the endometrium of a rhesus monkey; early secretory phase. (Reproduced with permission from Daron GH: The arterial pattern of the tunica mucosa of the uterus in the Macacus rhesus. Am J Anat 1936;58:349.)
When the corpus luteum regresses, hormonal support for the endometrium is withdrawn. The endometrium becomes thinner, which adds to the coiling of the spiral arteries. Foci of necrosis appear in the endometrium, and these coalesce. In addition, spasm and degeneration of the walls of the spiral arteries take place, leading to spotty hemorrhages that become confluent and produce the menstrual flow.
The vasospasm is probably produced by locally released prostaglandins. Large quantities of prostaglandins are present in the secretory endometrium and in menstrual blood, and infusions of prostagladin F2α (PGF2α) produce endometrial necrosis and bleeding.
From the point of view of endometrial function, the proliferative phase of the menstrual cycle represents restoration of the epithelium from the preceding menstruation, and the secretory phase represents preparation of the uterus for implantation of the fertilized ovum. The length of the secretory phase is remarkably constant at about 14 days, and the variations seen in the length of the menstrual cycle are due for the most part to variations in the length of the proliferative phase. When fertilization fails to occur during the secretory phase, the endometrium is shed and a new cycle starts.
Normal Menstruation
Menstrual blood is predominantly arterial, with only 25% of the blood being of venous origin. It contains tissue debris, prostaglandins, and relatively large amounts of fibrinolysin from endometrial tissue. The fibrinolysin lyses clots, so that menstrual blood does not normally contain clots unless the flow is excessive.
The usual duration of the menstrual flow is 3–5 days, but flows as short as 1 day and as long as 8 days can occur in normal women. The amount of blood lost may range normally from slight spotting to 80 mL; the average amount lost is 30 mL. Loss of more than 80 mL is abnormal. Obviously, the amount of flow can be affected by various factors, including the thickness of the endometrium, medication, and diseases that affect the clotting mechanism.
Anovulatory Cycles
In some instances, ovulation fails to occur during the menstrual cycle. Such anovulatory cycles are common for the first 12–18 months after menarche and again before the onset of the menopause. When ovulation does not occur, no corpus luteum is formed and the effects of progesterone on the endometrium are absent. Estrogens continue to cause growth, however, and the proliferative endometrium becomes thick enough to break down and begins to slough. The time it takes for bleeding to occur is variable, but it usually occurs in less than 28 days from the last menstrual period. The flow is also variable and ranges from scanty to relatively profuse.
Cyclical Changes in the Uterine Cervix
Although it is continuous with the body of the uterus, the cervix of the uterus is different in a number of ways. The mucosa of the uterine cervix does not undergo cyclical desquamation, but there are regular changes in the cervical mucus. Estrogen makes the mucus thinner and more alkaline, changes that promote the survival and transport of sperm. Progesterone makes it thick, tenacious, and cellular. The mucus is thinnest at the time of ovulation, and its elasticity, or spinnbarkeit, increases so that by midcycle, a drop can be stretched into a long, thin thread that may be 8–12 cm or more in length. In addition, it dries in an arborizing, fern-like pattern (Figure 22–14) when a thin layer is spread on a slide. After ovulation and during pregnancy, it becomes thick and fails to form the fern pattern.
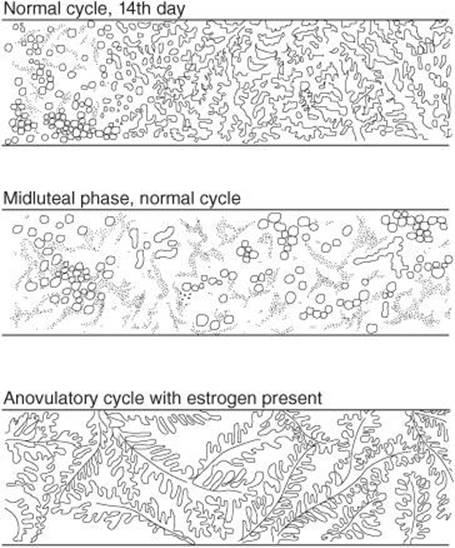
FIGURE 22–14 Patterns formed when cervical mucus is smeared on a slide, permitted to dry, and examined under the microscope. Progesterone makes the mucus thick and cellular. In the smear from a patient who failed to ovulate (bottom), no progesterone is present to inhibit the estrogen-induced fern pattern.
Vaginal Cycle
Under the influence of estrogens, the vaginal epithelium becomes cornified, and cornified epithelial cells can be identified in the vaginal smear. Under the influence of progesterone, a thick mucus is secreted, and the epithelium proliferates and becomes infiltrated with leukocytes. The cyclical changes in the vaginal smear in rats are relatively marked. The changes in humans and other species are similar but not so clear-cut.
Cyclical Changes in the Breasts
Although lactation normally does not occur until the end of pregnancy, cyclical changes take place in the breasts during the menstrual cycle. Estrogens cause proliferation of mammary ducts, whereas progesterone causes growth of lobules and alveoli. The breast swelling, tenderness, and pain experienced by many women during the 10 days preceding menstruation are probably due to distention of the ducts, hyperemia, and edema of the interstitial tissue of the breast. All these changes regress, along with the symptoms, during menstruation.
Changes During Intercourse
During sexual excitement in women, fluid is secreted onto the vaginal walls, probably because of release of VIP from vaginal nerves. A lubricating mucus is also secreted by the vestibular glands. The upper part of the vagina is sensitive to stretch, while tactile stimulation from the labia minora and clitoris adds to the sexual excitement. These stimuli are reinforced by tactile stimuli from the breasts and, as in men, by visual, auditory, and olfactory stimuli, which may build to the crescendo known as orgasm. During orgasm, autonomically mediated rhythmic contractions occur in the vaginal walls. Impulses also travel via the pudendal nerves and produce rhythmic contraction of the bulbocavernosus and ischiocavernosus muscles. The vaginal contractions may aid sperm transport but are not essential for it, since fertilization of the ovum is not dependent on female orgasm.
Indicators of Ovulation
Knowing when during the menstrual cycle ovulation occurs is important in increasing fertility or, conversely, in family planning. A convenient and reasonably reliable indicator of the time of ovulation is a change—usually a rise—in the basal body temperature (Figure 22–15). The rise starts 1–2 days after ovulation. Women interested in obtaining an accurate temperature chart should use a digital thermometer and take their temperatures (oral or rectal) in the morning before getting out of bed. The cause of the temperature change at the time of ovulation is probably the increase in progesterone secretion, since progesterone is thermogenic.
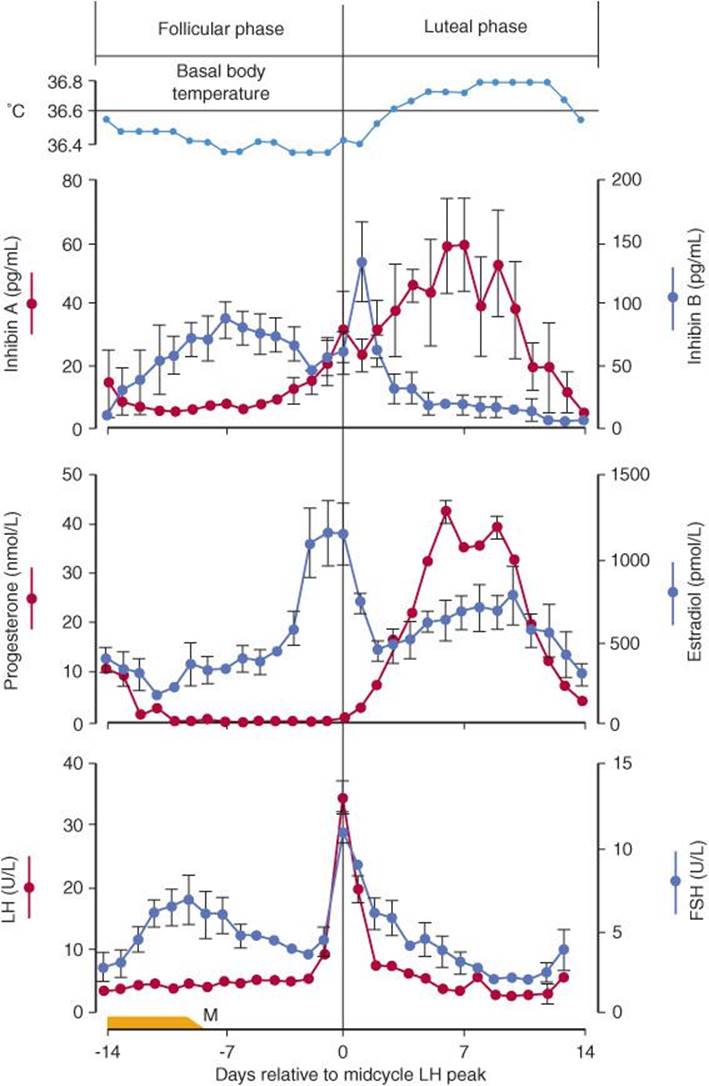
FIGURE 22–15 Basal body temperature and plasma hormone concentrations (mean ± standard error) during the normal human menstrual cycle. Values are aligned with respect to the day of the midcycle LH peak. FSH, follicle-stimulating hormone; LH, luteinizing hormone; M, menses.
A surge in LH secretion triggers ovulation, and ovulation normally occurs about 9 h after the peak of the LH surge at midcycle (Figure 22–15). The ovum lives for approximately 72 h after it is extruded from the follicle, but it is fertilizable for a much shorter time than this. In a study of the relation of isolated intercourse to pregnancy, 36% of women had a detected pregnancy following intercourse on the day of ovulation, but with intercourse on days after ovulation, the percentage was zero. Isolated intercourse on the first and second day before ovulation also led to pregnancy in about 36% of women. A few pregnancies resulted from isolated intercourse on day 3, 4, or 5 before ovulation, although the percentage was much lower, for example, 8% on day 5 before ovulation. Thus, some sperms can survive in the female genital tract and fertilize the ovum for up to 120 h before ovulation, but the most fertile period is clearly the 48 h before ovulation. However, for those interested in the “rhythm method” of contraception, it should be noted that there are rare but documented cases in the literature of pregnancy resulting from isolated coitus on every day of the cycle.
The Estrous Cycle
Mammals other than primates do not menstruate, and their sexual cycle is called an estrous cycle. It is named for the conspicuous period of “heat” (estrus) at the time of ovulation, normally the only time during which the sexual interest of the female is aroused. In spontaneously ovulating species with estrous cycles, such as the rat, no episodic vaginal bleeding occurs but the underlying endocrine events are essentially the same as those in the menstrual cycle. In other species, ovulation is induced by copulation (reflex ovulation).
OVARIAN HORMONES
Chemistry, Biosynthesis, & Metabolism of Estrogens
The naturally occurring estrogens are 17β-estradiol, estrone, and estriol (Figure 22–16). They are C18 steroids that do not have an angular methyl group attached to the 10 position or a (ê4-3-keto configuration in the A ring. They are secreted primarily by the granulosa cells of the ovarian follicles, the corpus luteum, and the placenta. Their biosynthesis depends on the enzyme aromatase (CYP19), which converts testosterone to estradiol and androstenedione to estrone (Figure 22–16). The latter reaction also occurs in fat, liver, muscle, and the brain.
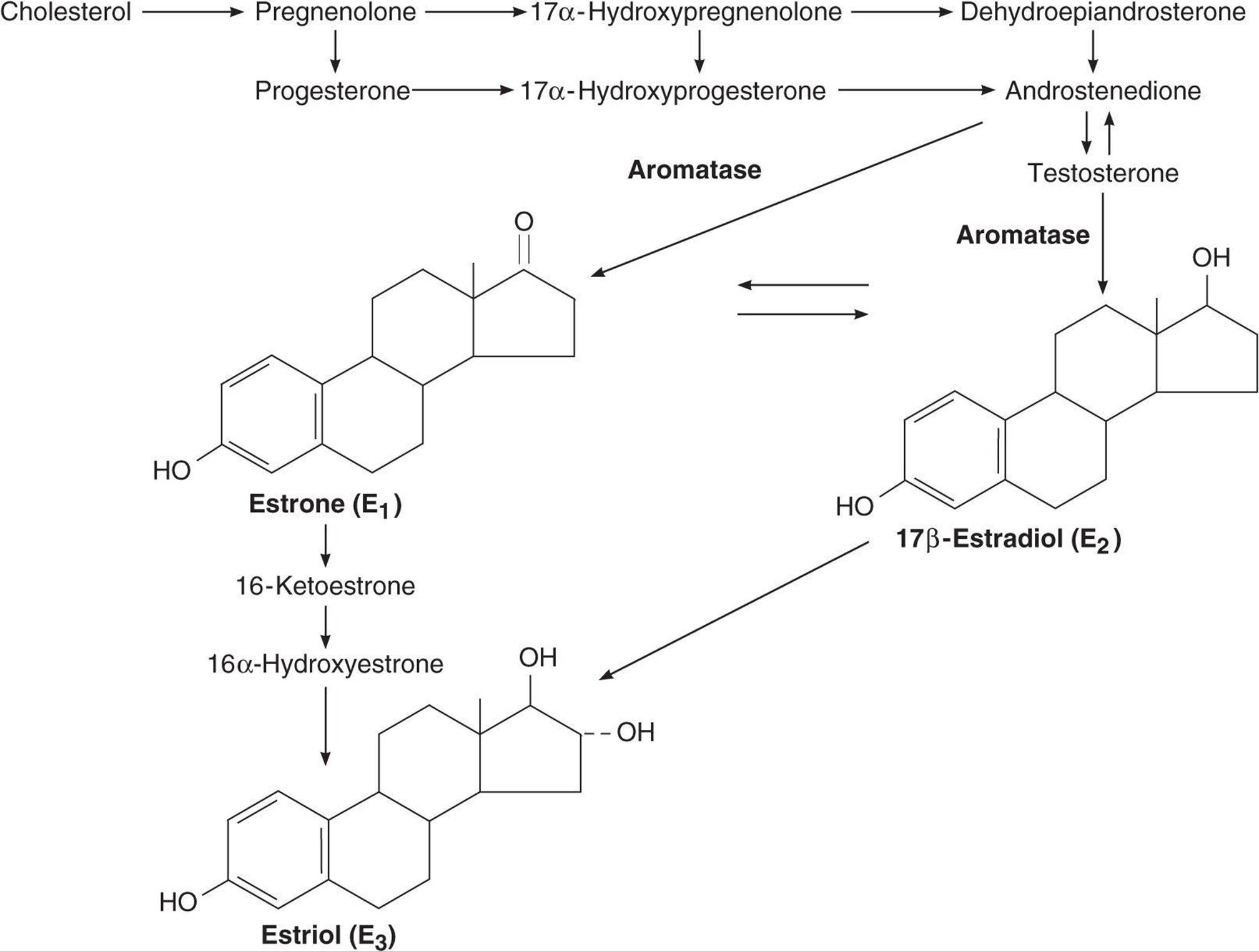
FIGURE 22–16 Biosynthesis and metabolism of estrogens. The formulas of the precursor steroids are shown in Figure 22–7.
Theca interna cells have many LH receptors, and LH acts via cAMP to increase conversion of cholesterol to androstenedione. The theca interna cells supply androstenedione to the granulosa cells. The granulosa cells make estradiol when provided with androgens (Figure 22–17), and it appears that the estradiol they form in primates is secreted into the follicular fluid. Granulosa cells have many FSH receptors, and FSH facilitates their secretion of estradiol by acting via cAMP to increase their aromatase activity. Mature granulosa cells also acquire LH receptors, and LH also stimulates estradiol production.
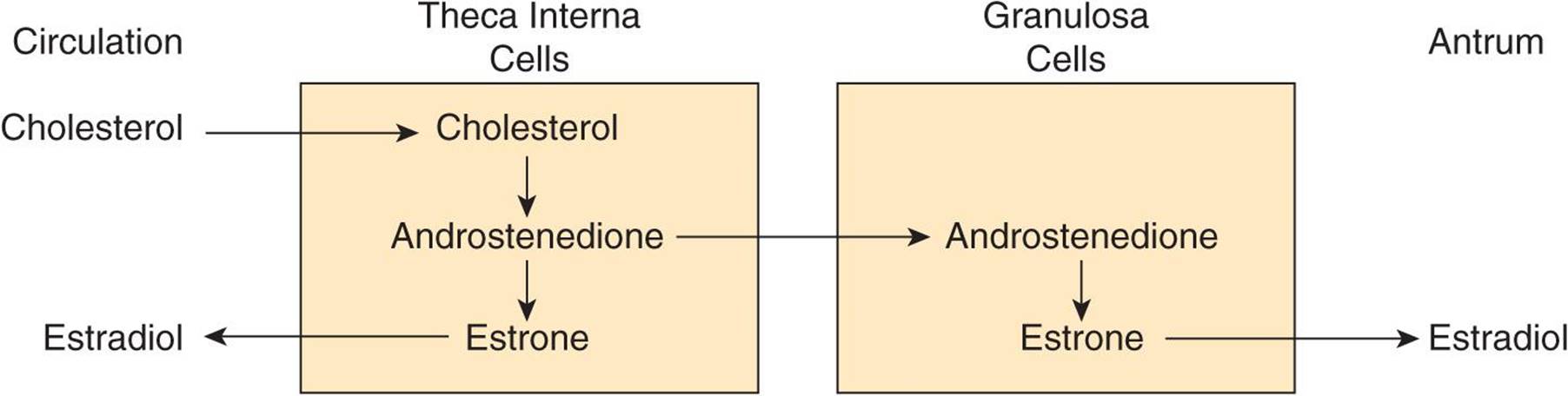
FIGURE 22–17 Interactions between theca and granulosa cells in estradiol synthesis and secretion.
Two per cent of the circulating estradiol is free, and the remainder is bound to protein: 60% to albumin and 38% to the same gonadal steroid-binding globulin (GBG) that binds testosterone.
In the liver, estradiol, estrone, and estriol are converted to glucuronide and sulfate conjugates. All these compounds, along with other metabolites, are excreted in the urine. Appreciable amounts are secreted in the bile and reabsorbed into the bloodstream (enterohepatic circulation).
Secretion
The concentration of estradiol in the plasma during the menstrual cycle is shown in Figure 22–15. Almost all of this estrogen comes from the ovary, and two peaks of secretion occur: one just before ovulation and one during the midluteal phase. The estradiol secretion rate is 36 μg/d (133 nmol/d) in the early follicular phase, 380 μg/d just before ovulation, and 250 μg/d during the midluteal phase (Table 22–3). After menopause, estrogen secretion declines to low levels.
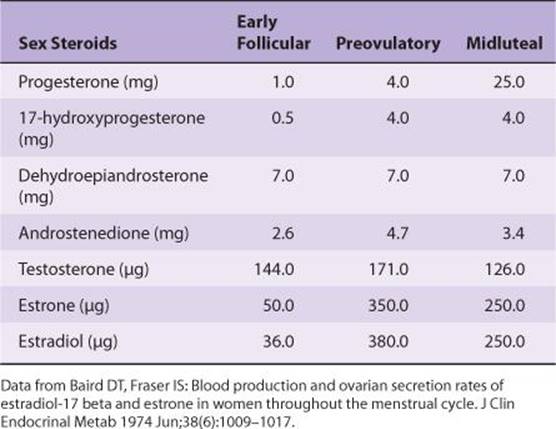
TABLE 22–3 Twenty-four-hour production rates of sex steroids in women at different stages of the menstrual cycle.
As noted previously, the estradiol production rate in men is about 50 μg/d (184 nmol/d).
Effects on the Female Genitalia
Estrogens facilitate the growth of the ovarian follicles and increase the motility of the uterine tubes. Their role in the cyclic changes in the endometrium, cervix, and vagina has been discussed previously. They increase uterine blood flow and have important effects on the smooth muscle of the uterus. In immature and castrated females, the uterus is small and the myometrium atrophic and inactive. Estrogens increase the amount of uterine muscle and its content of contractile proteins. Under the influence of estrogens, the muscle becomes more active and excitable, and action potentials in the individual fibers become more frequent. The “estrogen-dominated” uterus is also more sensitive to oxytocin.
Chronic treatment with estrogens causes the endometrium to hypertrophy. When estrogen therapy is discontinued, sloughing takes place with withdrawal bleeding. Some “breakthrough” bleeding may occur during treatment when estrogens are given for long periods. Prolonged exposure to estrogen alone (unopposed by progesterone) has been indicated as a risk factor in the development of endometrial cancer.
Effects on Endocrine Organs
Estrogens decrease FSH secretion. Under some circumstances, they inhibit LH secretion (negative feedback); in other circumstances, they increase LH secretion (positive feedback). Women are sometimes given large doses of estrogens for 4–6 days to prevent conception after coitus during the fertile period (postcoital or “morning-after” contraception). However, in this instance, pregnancy is probably prevented by interference with implantation of the ovum rather than changes in gonadotropin secretion.
Estrogens cause increased secretion of angiotensinogen and thyroid-binding globulin. They exert an important protein anabolic effect in chickens and cattle, possibly by stimulating the secretion of androgens from the adrenal, and estrogen treatment has been used commercially to increase the weight of domestic animals. They cause epiphysial closure in humans (see Chapter 21).
Effects on the Central Nervous System
The estrogens are responsible for estrous behavior in animals, and they increase libido in humans. They apparently exert this action by a direct effect on certain neurons in the hypothalamus Estrogens also increase the proliferation of dendrites on neurons and the number of synaptic knobs in rats.
Effects on the Breasts
Estrogens produce duct growth in the breasts and are largely responsible for breast enlargement at puberty in girls; they have been called the growth hormones of the breast. They are responsible for the pigmentation of the areolas, although pigmentation usually becomes more intense during the first pregnancy than it does at puberty. The role of estrogens in the overall control of breast growth and lactation is discussed below.
Female Secondary Sex Characteristics
The body changes that develop in girls at puberty—in addition to enlargement of breasts, uterus, and vagina—are due in part to estrogens, which are the “feminizing hormones,” and in part simply to the absence of testicular androgens. Women have narrow shoulders and broad hips, thighs that converge, and arms that diverge (wide carrying angle). This body configuration, plus the female distribution of fat in the breasts and buttocks, is seen also in castrate males. In women, the larynx retains its prepubertal proportions and the voice stays high-pitched. Women have less body hair and more scalp hair, and the pubic hair generally has a characteristic flat-topped pattern (female escutcheon). However, growth of pubic and axillary hair in both sexes is due primarily to androgens rather than estrogens.
Other Actions
Normal women retain salt and water and gain weight just before menstruation. Estrogens cause some degree of salt and water retention. However, aldosterone secretion is slightly elevated in the luteal phase, and this also contributes to the premenstrual fluid retention.
Estrogens are said to make sebaceous gland secretions more fluid and thus to counter the effect of testosterone and inhibit formation of comedones (“black-heads”) and acne. The liver palms, spider angiomas, and slight breast enlargement seen in advanced liver disease are due to increased circulating estrogens. The increase appears to be due to decreased hepatic metabolism of androstenedione, making more of this androgen available for conversion to estrogens.
Estrogens have a significant plasma cholesterol-lowering action, and they rapidly produce vasodilation by increasing the local production of NO. Their action on bone is discussed in Chapter 21.
Mechanism of Action
There are two principal types of nuclear estrogen receptors: estrogen receptor α (ERα) encoded by a gene on chromosome 6; and estrogen receptor β (ERβ), encoded by a gene on chromosome 14. Both are members of the nuclear receptor super-family (see Chapter 2). After binding estrogen, they form homodimers and bind to DNA, altering its transcription. Some tissues contain one type or the other, but overlap also occurs, with some tissues containing both ERα and ERβ. ERα is found primarily in the uterus, kidneys, liver, and heart, whereas ERβ is found primarily in the ovaries, prostate, lungs, gastrointestinal tract, hemopoietic system, and central nervous system (CNS). ERα and ERβ can also form heterodimers. Male and female mice in which the gene for ERα has been knocked out are sterile, develop osteoporosis, and continue to grow because their epiphyses do not close. ERβ female knockouts are infertile, but ERβ male knockouts are fertile even though they have hyperplastic prostates and loss of fat. Both receptors exist in isoforms and, like thyroid receptors, can bind to various activating and stimulating factors. In some situations, ERβ can inhibit ERα transcription. Thus, their actions are complex, multiple, and varied.
Most of the effects of estrogens are genomic, that is, due to actions on the nucleus, but some are so rapid that it is difficult to believe they are mediated via production of mRNAs. These include effects on neuronal discharge in the brain and, possibly, feedback effects on gonadotropin secretion. Evidence is accumulating that these effects are mediated by cell membrane receptors that appear to be structurally related to the nuclear receptors and produce their effects by intracellular mitogen-activated protein kinase pathways. Similar rapid effects of progesterone, testosterone, glucocorticoids, aldosterone, and 1,25-dihydroxycholecalciferol may also be produced by membrane receptors (see Chapter 16).
Synthetic and Environmental Estrogens
The ethinyl derivative of estradiol is a potent estrogen and, unlike the naturally occurring estrogens, is relatively active when given by mouth because it is resistant to hepatic metabolism. The activity of the naturally occurring hormones is low when they are administered by mouth because the portal venous drainage of the intestine carries them to the liver, where they are inactivated before they can reach the general circulation. Some nonsteroidal substances and a few compounds found in plants also have estrogenic activity. The plant estrogens are rarely a problem in human nutrition, but they may cause undesirable effects in farm animals. Dioxins, which are found in the environment and are produced by a variety of industrial processes, can activate estrogen response elements on genes. However, they have been reported to have antiestrogenic as well as estrogenic effects, and their role, if any, in the production of human disease remains a matter of disagreement and debate.
Because natural estrogens have undesirable as well as desirable effects (for example, they preserve bone in osteoporosis but can cause uterine and breast cancer), there has been an active search for “tailor-made” estrogens that have selective effects in humans. Two compounds, tamoxifen and raloxifene, show promise in this regard. Neither combats the symptoms of menopause, but both have the bone-preserving effects of estradiol. In addition, tamoxifen does not stimulate the breast, and raloxifene does not stimulate the breast or uterus. The way the effects of these selective estrogen receptor modulators (SERMs) are brought about is related to the complexity of the estrogen receptors and hence to differences in the way that the receptor–ligand complexes they form bind to DNA.
Chemistry, Biosynthesis, & Metabolism of Progesterone
Progesterone is a C21 steroid (Figure 22–18) secreted by the corpus luteum, the placenta, and (in small amounts) the follicle. It is an important intermediate in steroid biosynthesis in all tissues that secrete steroid hormones, and small amounts apparently enter the circulation from the testes and adrenal cortex. About 2% of the circulating progesterone is free whereas 80% is bound to albumin and 18% is bound to corticosteroid-binding globulin. Progesterone has a short half-life and is converted in the liver to pregnanediol, which is conjugated to glucuronic acid and excreted in the urine.
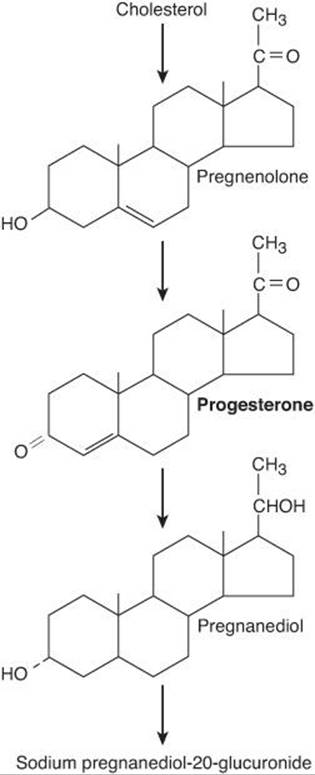
FIGURE 22–18 Biosynthesis of progesterone and major pathway for its metabolism. Other metabolites are also formed.
Secretion
In men, the plasma progesterone level is approximately 0.3 ng/mL (1 nmol/L). In women, the level is approximately 0.9 ng/mL (3 nmol/L) during the follicular phase of the menstrual cycle (Figure 22–15). The difference is due to secretion of small amounts of progesterone by cells in the ovarian follicles; theca cells provide pregnenolone to the granulosa cells, which convert it to progesterone. Late in the follicular phase, progesterone secretion begins to increase. During the luteal phase, the corpus luteum produces large quantities of progesterone (Table 22–3) and plasma progesterone is markedly increased to a peak value of approximately 18 ng/mL (60 nmol/L).
The stimulating effect of LH on progesterone secretion by the corpus luteum is due to activation of adenylyl cyclase and involves a subsequent step that is dependent on protein synthesis.
Actions
The principal target organs of progesterone are the uterus, the breasts, and the brain. Progesterone is responsible for the progestational changes in the endometrium and the cyclical changes in the cervix and vagina described above. It has an antiestrogenic effect on the myometrial cells, decreasing their excitability, their sensitivity to oxytocin, and their spontaneous electrical activity while increasing their membrane potential. It also decreases the number of estrogen receptors in the endometrium and increases the rate of conversion of 17β-estradiol to less active estrogens.
In the breast, progesterone stimulates the development of lobules and alveoli. It induces differentiation of estrogen-prepared ductal tissue and supports the secretory function of the breast during lactation.
The feedback effects of progesterone are complex and are exerted at both the hypothalamic and pituitary levels. Large doses of progesterone inhibit LH secretion and potentiate the inhibitory effect of estrogens, preventing ovulation.
Progesterone is thermogenic and is probably responsible for the rise in basal body temperature at the time of ovulation. It stimulates respiration, and the alveolar PCO2 (see Chapter 34) in women during the luteal phase of the menstrual cycle is lower than that in men. In pregnancy, the PCO2 falls as progesterone secretion rises. However, the physiologic significance of this respiratory response is unknown.
Large doses of progesterone produce natriuresis, probably by blocking the action of aldosterone on the kidney. The hormone does not have a significant anabolic effect.
Mechanism of Action
The effects of progesterone, like those of other steroids, are brought about by an action on DNA to initiate synthesis of new mRNA. The progesterone receptor is bound to a heat shock protein in the absence of the steroid, and progesterone binding releases the heat shock protein, exposing the DNA-binding domain of the receptor. The synthetic steroid mifepristone (RU 486) binds to the receptor but does not release the heat shock protein, and it blocks the binding of progesterone. Because the maintenance of early pregnancy depends on the stimulatory effect of progesterone on endometrial growth and its inhibition of uterine contractility, mifepristone combined with a prostaglandin can be used to produce elective abortions.
There are two isoforms of the progesterone receptor—PRA and PRB—that are produced by differential processing from a single gene. PRA is a truncated form, but it is likely that both isoforms mediate unique subsets of progesterone action.
Substances that mimic the action of progesterone are sometimes called progestational agents, gestagens, or progestins. They are used along with synthetic estrogens as oral contraceptive agents.
Relaxin
Relaxin is a polypeptide hormone that is produced in the corpus luteum, uterus, placenta, and mammary glands in women and in the prostate gland in men. During pregnancy, it relaxes the pubic symphysis and other pelvic joints and softens and dilates the uterine cervix. Thus, it facilitates delivery. It also inhibits uterine contractions and may play a role in the development of the mammary glands. In nonpregnant women, relaxin is found in the corpus luteum and the endometrium during the secretory but not the proliferative phase of the menstrual cycle. Its function in nonpregnant women is unknown. In men, it is found in semen, where it may help maintain sperm motility and aid in sperm penetration of the ovum.
In most species there is only one relaxin gene, but in humans there are two genes on chromosome 9 that code for two structurally different polypeptides that both have relaxin activity. However, only one of these genes is active in the ovary and the prostate. The structure of the polypeptide produced in these two tissues is shown in Figure 22–19.
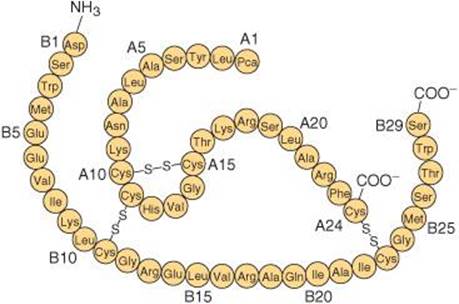
FIGURE 22–19 Structure of human luteal and seminal relaxin. Pca, pyroglutamic acid. (Modified and reproduced with permission from Winslow JW, et al: Human seminal relaxin is a product of the same gene as human luteal relaxin. Endocrinology 1992;130:2660. Copyright © 1992 by The Endocrine Society.)
CONTROL OF OVARIAN FUNCTION
FSH from the pituitary is responsible for the early maturation of the ovarian follicles, and FSH and LH together are responsible for their final maturation. A burst of LH secretion (Figure 22–15) is responsible for ovulation and the initial formation of the corpus luteum. A smaller midcycle burst of FSH secretion also occurs, the significance of which is uncertain. LH stimulates the secretion of estrogen and progesterone from the corpus luteum.
Hypothalamic Components
The hypothalamus occupies a key position in the control of gonadotropin secretion. Hypothalamic control is exerted by GnRH secreted into the portal hypophysial vessels. GnRH stimulates the secretion of FSH as well as LH.
GnRH is normally secreted in episodic bursts, and these bursts produce the circhoral peaks of LH secretion. They are essential for normal secretion of gonadotropins. If GnRH is administered by constant infusion, the GnRH receptors in the anterior pituitary down-regulate and LH secretion declines to zero. However, if GnRH is administered episodically at a rate of one pulse per hour, LH secretion is stimulated. This is true even when endogenous GnRH secretion has been prevented by a lesion of the ventral hypothalamus.
It is now clear not only that episodic secretion of GnRH is a general phenomenon but also that fluctuations in the frequency and amplitude of the GnRH bursts are important in generating the other hormonal changes that are responsible for the menstrual cycle. Frequency is increased by estrogens and decreased by progesterone and testosterone. The frequency increases late in the follicular phase of the cycle, culminating in the LH surge. During the secretory phase, the frequency decreases as a result of the action of progesterone (Figure 22–20), but when estrogen and progesterone secretion decrease at the end of the cycle, the frequency once again increases.
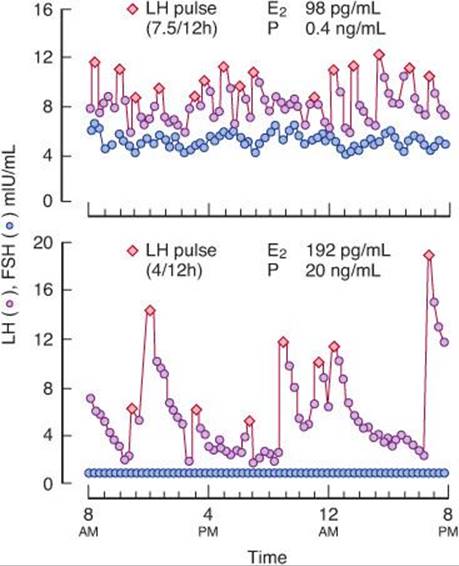
FIGURE 22–20 Episodic secretion of LH (s) and FSH (d) during the follicular stage (top) and the luteal stage (bottom) of the menstrual cycle. The numbers above each graph indicate the numbers of LH pulses per 12 hours and the plasma estradiol (E2) and progesterone (P) concentrations at these two times of the cycle. (Reproduced with permission from Marshall JC, Kelch RO: Gonadotropin-releasing hormone: Role of pulsatile secretion in the regulation of reproduction. N Engl J Med 1986;315:1459.)
At the time of the midcycle LH surge, the sensitivity of the gonadotropes to GnRH is greatly increased because of their exposure to GnRH pulses at a specific frequency. This self-priming effect of GnRH is important in producing a maximum LH response.
The nature and the exact location of the GnRH pulse generator in the hypothalamus are still unsettled. However, it is known in a general way that norepinephrine and possibly epinephrine in the hypothalamus increase GnRH pulse frequencies. Conversely, opioid peptides such as the enkephalins and β-endorphin reduce the frequency of GnRH pulses.
The down-regulation of pituitary receptors and the consequent decrease in LH secretion produced by constantly elevated levels of GnRH has led to the use of long-acting GnRH analogs to inhibit LH secretion in precocious puberty and in cancer of the prostate.
Feedback Effects
Changes in plasma LH, FSH, sex steroids, and inhibin during the menstrual cycle are shown in Figure 22–15, and their feedback relations are diagrammed in Figure 22–21. During the early part of the follicular phase, inhibin B is low and FSH is modestly elevated, fostering follicular growth. LH secretion is held in check by the negative feedback effect of the rising plasma estrogen level. At 36–48 h before ovulation, the estrogen feedback effect becomes positive, and this initiates the burst of LH secretion (LH surge) that produces ovulation. Ovulation occurs about 9 h after the LH peak. FSH secretion also peaks, despite a small rise in inhibin, probably because of the strong stimulation of gonadotropes by GnRH. During the luteal phase, the secretion of LH and FSH is low because of the elevated levels of estrogen, progesterone, and inhibin.
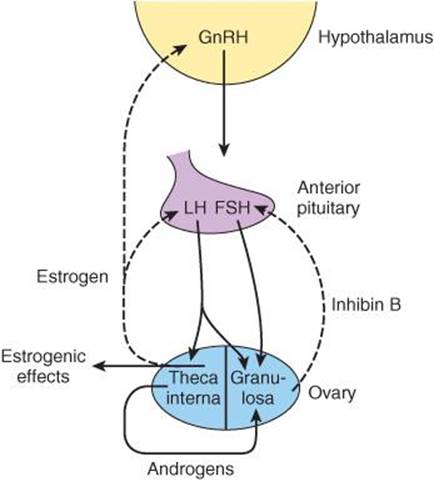
FIGURE 22–21 Feedback regulation of ovarian function. The cells of the theca interna provide androgens to the granulosa cells, and theca cells also produce the circulating estrogens that inhibit the secretion of GnRH, LH, and FSH. Inhibin from the granulosa cells inhibits FSH secretion. LH regulates the thecal cells, whereas the granulosa cells are regulated by both LH and FSH. The dashed arrows indicate inhibitory effects and the solid arrows stimulatory effects.
It should be emphasized that a moderate, constant level of circulating estrogen exerts a negative feedback effect on LH secretion, whereas during the cycle, an elevated estrogen level exerts a positive feedback effect and stimulates LH secretion. In monkeys, it has been demonstrated that estrogens must also be elevated for a minimum time to produce positive feedback. When circulating estrogen was increased about 300% for 24 h, only negative feedback was seen; but when it was increased about 300% for 36 h or more, a brief decline in secretion was followed by a burst of LH secretion that resembled the midcycle surge. When circulating levels of progesterone were high, the positive feedback effect of estrogen was inhibited. In primates there is evidence that both the negative and the positive feedback effects of estrogen are exerted in the mediobasal hypothalamus, but exactly how negative feedback is switched to positive feedback and then back to negative feedback in the luteal phase remains unknown.
Control of the Cycle
In an important sense, regression of the corpus luteum (luteolysis) starting 3–4 days before menses is the key to the menstrual cycle. PGF2α appears to be a physiologic luteolysin, but this prostaglandin is only active when endothelial cells producing ET-1 (see Chapter 32) are present. Therefore, it appears that at least in some species luteolysis is produced by the combined action of PGF2α and ET-1. In some domestic animals, oxytocin secreted by the corpus luteum appears to exert a local luteolytic effect, possibly by causing the release of prostaglandins. Once luteolysis begins, the estrogen and progesterone levels fall and the secretion of FSH and LH increases. A new crop of follicles develops, and then a single dominant follicle matures as a result of the action of FSH and LH. Near midcycle, estrogen secretion from the follicle rises. This rise augments the responsiveness of the pituitary to GnRH and triggers a burst of LH secretion. The resulting ovulation is followed by formation of a corpus luteum. Estrogen secretion drops, but progesterone and estrogen levels then rise together, along with inhibin B. The elevated levels inhibit FSH and LH secretion for a while, but luteolysis again occurs and a new cycle starts.
Reflex Ovulation
Female cats, rabbits, mink, and some other animals have long periods of estrus, during which they ovulate only after copulation. Such reflex ovulation is brought about by afferent impulses from the genitalia and the eyes, ears, and nose that converge on the ventral hypothalamus and provoke an ovulation-inducing release of LH from the pituitary. In species such as rats, monkeys, and humans, ovulation is a spontaneous periodic phenomenon, but neural mechanisms are also involved. Ovulation can be delayed 24 h in rats by administering pentobarbital or various other neurally active drugs 12 h before the expected time of follicle rupture.
Contraception
Methods commonly used to prevent conception are listed in Table 22–4, along with their failure rates. Once conception has occurred, abortion can be produced by progesterone antagonists such as mifepristone.
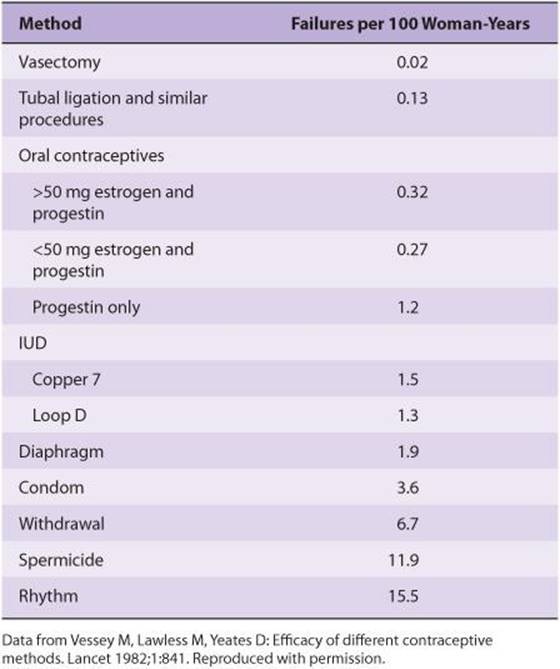
TABLE 22–4 Relative effectiveness of frequently used contraceptive methods.
Implantation of foreign bodies in the uterus causes changes in the duration of the sexual cycle in a number of mammalian species. In humans, such foreign bodies do not alter the menstrual cycle, but they act as effective contraceptive devices. Intrauterine implantation of pieces of metal or plastic (intrauterine devices, IUDs) has been used in programs aimed at controlling population growth. Although the mechanism of action of IUDs is still unsettled, they seem in general to prevent sperm from fertilizing ova. Those containing copper appear to exert a spermatocidal effect. IUDs that slowly release progesterone or synthetic progestins have the additional effect of thickening cervical mucus so that entry of sperm into the uterus is impeded. IUDs can cause intrauterine infections, but these usually occur in the first month after insertion and in women exposed to sexually transmitted diseases.
Women undergoing long-term treatment with relatively large doses of estrogen do not ovulate, probably because they have depressed FSH levels and multiple irregular bursts of LH secretion rather than a single midcycle peak. Women treated with similar doses of estrogen plus a progestational agent do not ovulate because the secretion of both gonadotropins is suppressed. In addition, the progestin makes the cervical mucus thick and unfavorable to sperm migration, and it may also interfere with implantation. For contraception, an orally active estrogen such as ethinyl estradiol is often combined with a synthetic progestin such as norethindrone. The pills are administered for 21 days, then withdrawn for 5–7 days to permit menstrual flow, and started again. Like ethinyl estradiol, norethindrone has an ethinyl group on position 17 of the steroid nucleus, so it is resistant to hepatic metabolism and consequently is effective by mouth. In addition to being a progestin, it is partly metabolized to ethinyl estradiol, and for this reason it also has estrogenic activity. Small as well as large doses of estrogen are effective (Table 22–4).
Implants made up primarily of progestins such as levonorgestrel are now seeing increased use in some parts of the world. These are inserted under the skin and can prevent pregnancy for up to 5 years. They often produce amenorrhea, but otherwise they appear to be effective and well tolerated.
ABNORMALITIES OF OVARIAN FUNCTION
Menstrual Abnormalities
Some women who are infertile have anovulatory cycles; they fail to ovulate but have menstrual periods at fairly regular intervals. As noted above, anovulatory cycles are the rule for the first 1–2 years after menarche and again before the menopause. Amenorrhea is the absence of menstrual periods. If menstrual bleeding has never occurred, the condition is called primary amenorrhea. Some women with primary amenorrhea have small breasts and other signs of failure to mature sexually. Cessation of cycles in a woman with previously normal periods is called secondary amenorrhea. The most common cause of secondary amenorrhea is pregnancy, and the old clinical maxim that “secondary amenorrhea should be considered to be due to pregnancy until proved otherwise” has considerable merit. Other causes of amenorrhea include emotional stimuli and changes in the environment, hypothalamic diseases, pituitary disorders, primary ovarian disorders, and various systemic diseases. Evidence suggests that in some women with hypothalamic amenorrhea, the frequency of GnRH pulses is slowed as a result of excess opioid activity in the hypothalamus. In encouraging preliminary studies, the frequency of GnRH pulses was increased by administration of the orally active opioid blocker naltrexone.
The terms hypomenorrhea and menorrhagia refer to scanty and abnormally profuse flow, respectively, during regular periods. Metrorrhagia is bleeding from the uterus between periods, and oligomenorrhea is reduced frequency of periods. Dysmenorrhea is painful menstruation. The severe menstrual cramps that are common in young women quite often disappear after the first pregnancy. Most of the symptoms of dysmenorrhea are due to accumulation of prostaglandins in the uterus, and symptomatic relief has been obtained by treatment with inhibitors of prostaglandin synthesis.
Some women develop symptoms such as irritability, bloating, edema, decreased ability to concentrate, depression, headache, and constipation during the last 7–10 days of their menstrual cycles. These symptoms of the premenstrual syndrome (PMS) have been attributed to salt and water retention. However, it seems unlikely that this or any of the other hormonal alterations that occur in the late luteal phase are responsible because the time course and severity of the symptoms are not modified if the luteal phase is terminated early and menstruation produced by administration of mifepristone. The antidepressant fluoxetine (Prozac), which is a serotonin reuptake inhibitor, and the benzodiazepine alprazolam (Xanax) produce symptomatic relief, and so do GnRH-releasing agonists in doses that suppress the pituitary–ovarian axis. How these diverse clinical observations fit together to produce a picture of the pathophysiology of PMS is still unknown (see Clinical Box 22–4).
CLINICAL BOX 22–4
Genetic Defects Causing Reproductive Abnormalities
A number of single-gene mutations cause reproductive abnormalities when they occur in women. Examples include (1) Kallmann syndrome, which causes hypogonadotropic hypogonadism; (2) GnRH resistance, FSH resistance, and LH resistance, which are due to defects in the GnRH, FSH, or LH receptors, respectively; and (3) aromatase deficiency, which prevents the formation of estrogens. These are all caused by loss-of-function mutations. An interesting gain-of-function mutation causes the McCune–Albright syndrome, in which Gsα becomes constitutively active in certain cells but not others (mosaicism) because a somatic mutation after initial cell division has occurred in the embryo. It is associated with multiple endocrine abnormalities, including precocious puberty and amenorrhea with galactorrhea.
PREGNANCY
Fertilization & Implantation
In humans, fertilization of the ovum by the sperm (see Chapter 23) usually occurs in the ampulla of the uterine tube. Fertilization involves (1) chemoattraction of the sperm to the ovum by substances produced by the ovum; (2) adherence to the zona pellucida, the membranous structure surrounding the ovum; (3) penetration of the zona pellucida and the acrosome reaction; and (4) adherence of the sperm head to the cell membrane of the ovum, with breakdown of the area of fusion and release of the sperm nucleus into the cytoplasm of the ovum (Figure 22–22). Millions of sperm are deposited in the vagina during intercourse. Eventually, 50–100 sperm reach the ovum, and many of them contact the zona pellucida. Sperm bind to a receptor in the zona, and this is followed by the acrosomal reaction, that is, the breakdown of the acrosome, the lysosome-like organelle on the head of the sperm (Figure 23–4). Various enzymes are released, including the trypsin-like protease acrosin. Acrosin facilitates but is not required for the penetration of the sperm through the zona pellucida. When one sperm reaches the membrane of the ovum, fusion to the ovum membrane is mediated by fertilin, a protein on the surface of the sperm head that resembles the viral fusion proteins that permit some viruses to attack cells. The fusion provides the signal that initiates development. In addition, the fusion sets off a reduction in the membrane potential of the ovum that prevents polyspermy, the fertilization of the ovum by more than one sperm. This transient potential change is followed by a structural change in the zona pellucida that provides protection against polyspermy on a more long-term basis.
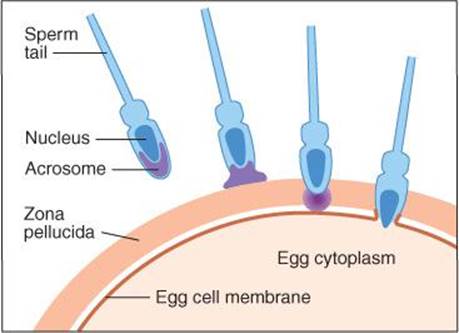
FIGURE 22–22 Sequential events in fertilization in mammals. Sperm are attracted to the ovum, bind to the zona pellucida, release acrosomal enzymes, penetrate the zona pellucida, and fuse with the membrane of the ovum, releasing the sperm nucleus into its cytoplasm. Current evidence indicates that the side, rather than the tip, of the sperm head fuses with the egg cell membrane. (Modified from Vacquier VD: Evolution of gamete recognition proteins. Science 1998;281:1995.)
The developing embryo, now called a blastocyst, moves down the tube into the uterus. This journey takes about 3 days, during which the blastocyst reaches the 8- or 16-cell stage. Once in contact with the endometrium, the blastocyst becomes surrounded by an outer layer of syncytiotrophoblast, a multi-nucleate mass with no discernible cell boundaries, and an inner layer of cytotrophoblast made up of individual cells. The syncytiotrophoblast erodes the endometrium, and the blastocyst burrows into it (implantation). The implantation site is usually on the dorsal wall of the uterus. A placenta then develops, and the trophoblast remains associated with it.
Failure to Reject the “Fetal Graft”
It should be noted that the fetus and the mother are two genetically distinct individuals, and the fetus is in effect a transplant of foreign tissue in the mother. However, the transplant is tolerated, and the rejection reaction that is characteristically produced when other foreign tissues are transplanted (see Chapter 3) fails to occur. The way the “fetal graft” is protected is unknown. However, one explanation may be that the placental trophoblast, which separates maternal and fetal tissues, does not express the polymorphic class I and class II MHC genes and instead expresses HLA-G, a nonpolymorphic gene. Therefore, antibodies against the fetal proteins do not develop. In addition, there is Fas ligand on the surface of the placenta, and this binds to T cells, causing them to undergo apoptosis (see Chapter 3).
Infertility
The vexing clinical problem of infertility often requires extensive investigation before a cause is found. In 30% of cases the problem is in the man; in 45%, the problem is in the woman; in 20%, both partners have a problem; and in 5% no cause can be found. In vitro fertilization, that is, removing mature ova, fertilizing them with sperm, and implanting one or more of them in the uterus at the four-cell stage is of some value in these cases. It has a 5–10% chance of producing a live birth.
Endocrine Changes
In all mammals, the corpus luteum in the ovary at the time of fertilization fails to regress and instead enlarges in response to stimulation by gonadotropic hormones secreted by the placenta. The placental gonadotropin in humans is called human chorionic gonadotropin (hCG). The enlarged corpus luteum of pregnancy secretes estrogens, progesterone, and relaxin. Progesterone and relaxin help maintain pregnancy by inhibiting myometrial contractions; progesterone prevents prostaglandin production by the uterus, which stops contractions from occurring. In humans, the placenta produces sufficient estrogen and progesterone from maternal and fetal precursors to take over the function of the corpus luteum after the 6th week of pregnancy. Ovariectomy before the 6th week thus leads to abortion, but ovariectomy thereafter has no effect on the pregnancy. The function of the corpus luteum begins to decline after 8 weeks of pregnancy, but it persists throughout pregnancy. hCG secretion decreases after an initial marked rise, but estrogen and progesterone secretion increase until just before parturition (Table 22–5).
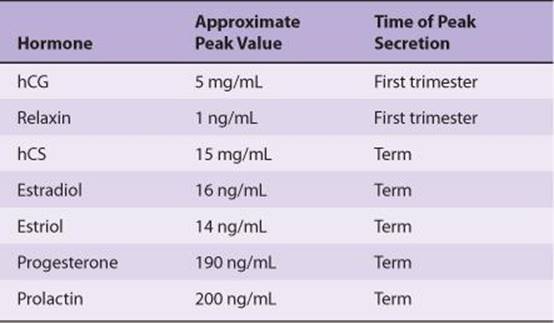
TABLE 22–5 Hormone levels in human maternal blood during normal pregnancy.
Human Chorionic Gonadotropin
hCG is a glycoprotein that contains galactose and hexosamine. It is produced by the syncytiotrophoblast. Like the pituitary glycoprotein hormones, it is made up of α and β subunits. hCG-α is identical to the α subunit of LH, FSH, and TSH. The molecular weight of hCG-α is 18,000, and that of hCG-β is 28,000. hCG is primarily luteinizing and luteotropic and has little FSH activity. It can be measured by radioimmunoassay and detected in the blood as early as 6 days after conception. Its presence in the urine in early pregnancy is the basis of the various laboratory tests for pregnancy, and it can sometimes be detected in the urine as early as 14 days after conception. It appears to act on the same receptor as LH. hCG is not absolutely specific for pregnancy. Small amounts are secreted by a variety of gastrointestinal and other tumors in both sexes, and hCG has been measured in individuals with suspected tumors as a “tumor marker.” It also appears that the fetal liver and kidney normally produce small amounts of hCG.
Human Chorionic Somatomammotropin
The syncytiotrophoblast also secretes large amounts of a protein hormone that is lactogenic and has a small amount of growth-stimulating activity. This hormone has been called chorionic growth hormone-prolactin (CGP) and human placental lactogen (hPL), but it is now generally called human chorionic somatomammotropin (hCS). The structure of hCS is very similar to that of human growth hormone (see Chapter 18), and it appears that these two hormones and prolactin evolved from a common progenitor hormone. Large quantities of hCS are found in maternal blood, but very little reaches the fetus. Secretion of growth hormone from the maternal pituitary is not increased during pregnancy and may actually be decreased by hCS. However, hCS has most of the actions of growth hormone and apparently functions as a “maternal growth hormone of pregnancy” to bring about the nitrogen, potassium, and calcium retention, lipolysis, and decreased glucose utilization seen in this state. These latter two actions divert glucose to the fetus. The amount of hCS secreted is proportional to the size of the placenta, which normally weighs about one-sixth as much as the fetus. Low hCS levels are a sign of placental insufficiency.
Other Placental Hormones
In addition to hCG, hCS, progesterone, and estrogens, the placenta secretes other hormones. Human placental fragments probably produce proopiomelanocortin (POMC). In culture, they release corticotropin-releasing hormone (CRH), β-endorphin, α-melanocyte-stimulating hormone (MSH), and dynorphin A, all of which appear to be identical to their hypothalamic counterparts. They also secrete GnRH and inhibin, and since GnRH stimulates and inhibin inhibits hCG secretion, locally produced GnRH and inhibin may act in a paracrine fashion to regulate hCG secretion. The trophoblast cells and amnion cells also secrete leptin, and moderate amounts of this satiety hormone enter the maternal circulation. Some also enters the amniotic fluid. Its function in pregnancy is unknown. The placenta also secretes prolactin in a number of forms.
Finally, the placenta secretes the α subunits of hCG, and the plasma concentration of free α subunits rises throughout pregnancy. These α subunits acquire a carbohydrate composition that makes them unable to combine with β subunits, and their prominence suggests that they have a function of their own. It is interesting in this regard that the secretion of the prolactin produced by the endometrium also appears to increase throughout pregnancy, and it may be that the circulating α subunits stimulate endometrial prolactin secretion.
The cytotrophoblast of the human chorion contains prorenin (see Chapter 38). A large amount of prorenin is also present in amniotic fluid, but its function in this location is unknown.
Fetoplacental Unit
The fetus and the placenta interact in the formation of steroid hormones. The placenta synthesizes pregnenolone and progesterone from cholesterol. Some of the progesterone enters the fetal circulation and provides the substrate for the formation of cortisol and corticosterone in the fetal adrenal glands (Figure 22–23). Some of the pregnenolone enters the fetus and, along with pregnenolone synthesized in the fetal liver, is the substrate for the formation of dehydroepiandrosterone sulfate (DHEAS) and 16-hydroxydehydroepiandrosterone sulfate (16-OHDHEAS) in the fetal adrenal. Some 16-hydroxylation also occurs in the fetal liver. DHEAS and 16-OHDHEAS are transported back to the placenta, where DHEAS forms estradiol and 16-OHDHEAS forms estriol. The principal estrogen formed is estriol, and since fetal 16-OHDHEAS is the principal substrate for the estrogens, the urinary estriol excretion of the mother can be monitored as an index of the state of the fetus.
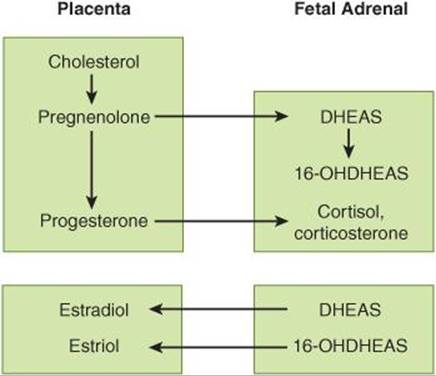
FIGURE 22–23 Interactions between the placenta and the fetal adrenal cortex in the production of steroids.
Parturition
The duration of pregnancy in humans averages 270 days from fertilization (284 days from the first day of the menstrual period preceding conception). Irregular uterine contractions increase in frequency in the last month of pregnancy.
The difference between the body of the uterus and the cervix becomes evident at the time of delivery. The cervix, which is firm in the nonpregnant state and throughout pregnancy until near the time of delivery, softens and dilates, while the body of the uterus contracts and expels the fetus.
There is still considerable uncertainty about the mechanisms responsible for the onset of labor. One factor is the increase in circulating estrogens produced by increased circulating DHEAS. This makes the uterus more excitable, increases the number of gap junctions between myometrial cells, and causes production of more prostaglandins, which in turn cause uterine contractions. In humans, CRH secretion by the fetal hypothalamus increases and is supplemented by increased placental production of CRH. This increases circulating adrenocorticotropic hormone (ACTH) in the fetus, and the resulting increase in cortisol hastens the maturation of the respiratory system. Thus, in a sense, the fetus picks the time to be born by increasing CRH secretion.
The number of oxytocin receptors in the myometrium and the decidua (the endometrium of pregnancy) increases more than 100-fold during pregnancy and reaches a peak during early labor. Estrogens increase the number of oxytocin receptors, and uterine distention late in pregnancy may also increase their formation. In early labor, the oxytocin concentration in maternal plasma is not elevated from the prelabor value of about 25 pg/mL. It is possible that the marked increase in oxytocin receptors causes the uterus to respond to normal plasma oxytocin concentrations. However, at least in rats, the amount of oxytocin mRNA in the uterus increases, reaching a peak at term; this suggests that locally produced oxytocin also participates in the process.
Premature onset of labor is a problem because premature infants have a high mortality rate and often require intensive, expensive care. Intramuscular 17α-hydroxyprogesterone causes a significant decrease in the incidence of premature labor. The mechanism by which it exerts its effect is uncertain, but it may be that the steroid provides a stable level of circulating progesterone. Progesterone relaxes uterine smooth muscle, inhibits the action of oxytocin on the muscle, and reduces the formation of gap junctions between the muscle fibers. All these actions would be expected to inhibit the onset of labor.
Once labor is started, the uterine contractions dilate the cervix, and this dilation in turn sets up signals in afferent nerves that increase oxytocin secretion (Figure 22–24). The plasma oxytocin level rises and more oxytocin becomes available to act on the uterus. Thus, a positive feedback loop is established that aids delivery and terminates on expulsion of the products of conception. Oxytocin increases uterine contractions in two ways: (1) It acts directly on uterine smooth muscle cells to make them contract and (2) it stimulates the formation of prostaglandins in the decidua. The prostaglandins enhance the oxytocin-induced contractions.
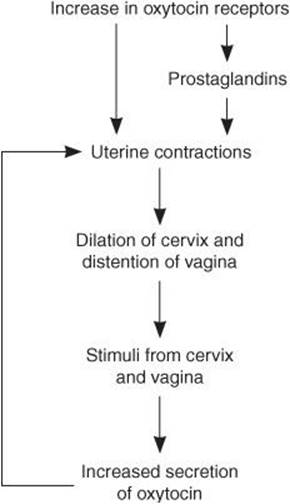
FIGURE 22–24 Role of oxytocin in parturition.
During labor, spinal reflexes and voluntary contractions of the abdominal muscles (“bearing down”) also aid in delivery. However, delivery can occur without bearing down and without a reflex increase in secretion of oxytocin from the posterior pituitary gland, since paraplegic women can go into labor and deliver.
LACTATION
Development of the Breasts
Many hormones are necessary for full mammary development. In general, estrogens are primarily responsible for proliferation of the mammary ducts and progesterone for the development of the lobules. In rats, some prolactin is also needed for development of the glands at puberty, but it is not known if prolactin is necessary in humans. During pregnancy, prolactin levels increase steadily until term, and levels of estrogens and progesterone are elevated as well, producing full lobuloalveolar development.
Secretion & Ejection of Milk
The composition of human and cows’ milk is shown in Table 22–6. In estrogen- and progesterone-primed rodents, injections of prolactin cause the formation of milk droplets and their secretion into the ducts. Oxytocin causes contraction of the myoepithelial cells lining the duct walls, with consequent ejection of the milk through the nipple.
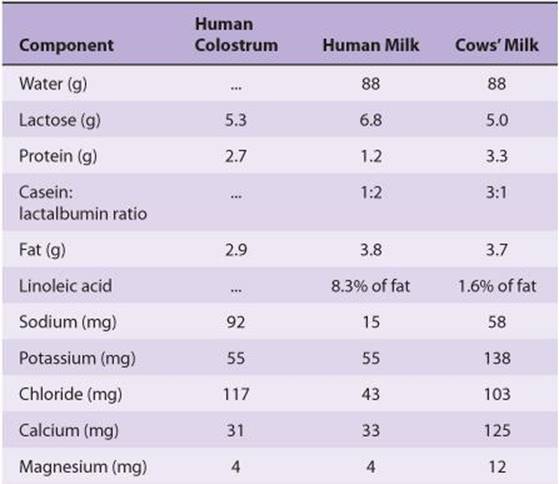
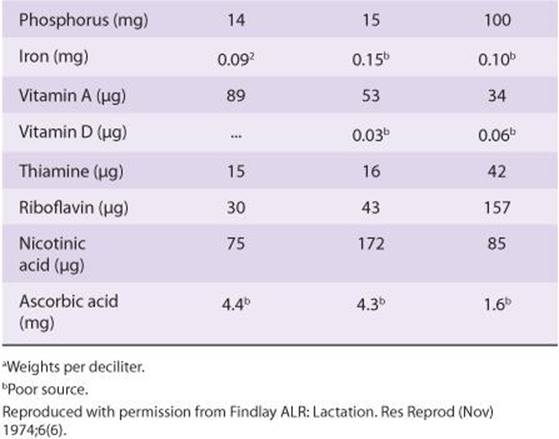
TABLE 22–6 Composition of colostrum and milk.a
Initiation of Lactation after Delivery
The breasts enlarge during pregnancy in response to high circulating levels of estrogens, progesterone, prolactin, and possibly hCG. Some milk is secreted into the ducts as early as the 5th month, but the amounts are small compared with the surge of milk secretion that follows delivery. In most animals, milk is secreted within an hour after delivery, but in women it takes 1–3 days for the milk to “come in.”
After expulsion of the placenta at parturition, the levels of circulating estrogens and progesterone abruptly decline. The drop in circulating estrogen initiates lactation. Prolactin and estrogen synergize in producing breast growth, but estrogen antagonizes the milk-producing effect of prolactin on the breast. Indeed, in women who do not wish to nurse their babies, estrogens may be administered to stop lactation.
Suckling not only evokes reflex oxytocin release and milk ejection, it also maintains and augments the secretion of milk because of the stimulation of prolactin secretion it produces.
Effect of Lactation on Menstrual Cycles
Women who do not nurse their infants usually have their first menstrual period 6 weeks after delivery. However, women who nurse regularly have amenorrhea for 25–30 weeks. Nursing stimulates prolactin secretion, and evidence suggests that prolactin inhibits GnRH secretion, inhibits the action of GnRH on the pituitary, and antagonizes the action of gonadotropins on the ovaries. Ovulation is inhibited, and the ovaries are inactive, so estrogen and progesterone output falls to low levels. Consequently, only 5–10% of women become pregnant again during the suckling period, and nursing has long been known to be an important, if only partly effective, method of birth control. Furthermore, almost 50% of the cycles in the first 6 months after resumption of menses are anovulatory (see Clinical Box 22–5).
CLINICAL BOX 22–5
Chiari–Frommel Syndrome
An interesting, although rare, condition is persistence of lactation (galactorrhea) and amenorrhea in women who do not nurse after delivery. This condition, called the Chiari–Frommel syndrome, may be associated with some genital atrophy and is due to persistent prolactin secretion without the secretion of the FSH and LH necessary to produce maturation of new follicles and ovulation. A similar pattern of galactorrhea and amenorrhea with high circulating prolactin levels is seen in nonpregnant women with chromophobe pituitary tumors and in women in whom the pituitary stalk has been sectioned during treatment of cancer.
Gynecomastia
Breast development in the male is called gynecomastia. It may be unilateral but is more commonly bilateral. It is common in newborns because of transplacental passage of maternal estrogens (occurring in about 75%). It also occurs in a mild, transient form in 70% of normal boys at the time of puberty and in many men over the age of 50. It occurs in androgen resistance. It is a complication of estrogen therapy and is seen in patients with estrogen-secreting tumors. It is found in a wide variety of seemingly unrelated conditions, including eunuchoidism, hyperthyroidism, and cirrhosis of the liver. Digitalis can produce it, apparently because cardiac glycosides are weakly estrogenic. It can also be caused by many other drugs. It has been seen in malnourished prisoners of war, but only after they were liberated and eating an adequate diet. A feature common to many and perhaps all cases of gynecomastia is an increase in the plasma estrogen:androgen ratio due to either increased circulating estrogens or decreased circulating androgens.
HORMONES & CANCER
About 35% of carcinomas of the breast in women of child-bearing age are estrogen-dependent; their continued growth depends on the presence of estrogens in the circulation. The tumors are not cured by decreasing estrogen secretion, but symptoms are dramatically relieved, and the tumor regresses for months or years before recurring (see Chapter 16). Women with estrogen-dependent tumors often have a remission when their ovaries are removed. Inhibition of the action of estrogens with tamoxifen also produces remissions, and inhibition of estrogen formation with drugs that inhibit aromatase (Figure 22–16) is even more effective.
CHAPTER SUMMARY
![]() Differences between males and females depend primarily on a single chromosome (the Y chromosome) and a single pair of endocrine structures (the gonads); testes in the male and ovaries in the female.
Differences between males and females depend primarily on a single chromosome (the Y chromosome) and a single pair of endocrine structures (the gonads); testes in the male and ovaries in the female.
![]() The gonads have a dual function: the production of germ cells (gametogenesis) and the secretion of sex hormones. The testes secrete large amounts of androgens, principally testosterone, but they also secrete small amounts of estrogens. The ovaries secrete large amounts of estrogens and small amounts of androgens.
The gonads have a dual function: the production of germ cells (gametogenesis) and the secretion of sex hormones. The testes secrete large amounts of androgens, principally testosterone, but they also secrete small amounts of estrogens. The ovaries secrete large amounts of estrogens and small amounts of androgens.
![]() The reproductive system of women has regular cyclical changes that can be thought of as periodic preparations for fertilization and pregnancy. In humans and other primates, the cycle is a menstrual cycle, and features the periodic vaginal bleeding that occurs with the shedding of the uterine mucosa (menstruation).
The reproductive system of women has regular cyclical changes that can be thought of as periodic preparations for fertilization and pregnancy. In humans and other primates, the cycle is a menstrual cycle, and features the periodic vaginal bleeding that occurs with the shedding of the uterine mucosa (menstruation).
![]() Ovaries also secrete progesterone, a steroid that has special functions in preparing the uterus for pregnancy. During pregnancy the ovaries secrete relaxin, which facilitates the delivery of the fetus. In both sexes, the gonads secrete other polypeptides, including inhibin B, a polypeptide that inhibits FSH secretion.
Ovaries also secrete progesterone, a steroid that has special functions in preparing the uterus for pregnancy. During pregnancy the ovaries secrete relaxin, which facilitates the delivery of the fetus. In both sexes, the gonads secrete other polypeptides, including inhibin B, a polypeptide that inhibits FSH secretion.
![]() In women, a period called perimenopause precedes menopause, and can last up to 10 years; during this time the menstrual cycles become irregular and the level of inhibins decrease.
In women, a period called perimenopause precedes menopause, and can last up to 10 years; during this time the menstrual cycles become irregular and the level of inhibins decrease.
![]() Once in menopause, the ovaries no longer secrete progesterone and 17β-estradiol and estrogen is formed only in small amounts by aromatization of androstenedione in peripheral tissues.
Once in menopause, the ovaries no longer secrete progesterone and 17β-estradiol and estrogen is formed only in small amounts by aromatization of androstenedione in peripheral tissues.
![]() The naturally occurring estrogens are 17β estradiol, estrone, and estriol. They are secreted primarily by the granulosa cells of the ovarian follicles, the corpus luteum, and the placenta. Their biosynthesis depends on the enzyme aromatase (CYP19), which converts testosterone to estradiol and androstenedione to estrone. The latter reaction also occurs in fat, liver, muscle, and the brain.
The naturally occurring estrogens are 17β estradiol, estrone, and estriol. They are secreted primarily by the granulosa cells of the ovarian follicles, the corpus luteum, and the placenta. Their biosynthesis depends on the enzyme aromatase (CYP19), which converts testosterone to estradiol and androstenedione to estrone. The latter reaction also occurs in fat, liver, muscle, and the brain.
MULTIPLE-CHOICE QUESTIONS
For all questions, select the single best answer unless otherwise directed.
1. If a young woman has high plasma levels of T3, cortisol, and renin activity but her blood pressure is only slightly elevated and she has no symptoms or signs of thyrotoxicosis or Cushing syndrome, the most likely explanation is that
A. she has been treated with TSH and ACTH.
B. she has been treated with T3 and cortisol.
C. she is in the third trimester of pregnancy.
D. she has an adrenocortical tumor.
E. she has been subjected to chronic stress.
2. In humans, fertilization usually occurs in the
A. vagina.
B. cervix.
C. uterine cavity.
D. uterine tubes.
E. abdominal cavity.
3. Which of the following is not a steroid?
A. 17α-hydroxyprogesterone
B. Estrone
C. Relaxin
D. Pregnenolone
E. Etiocholanolone
4. Which of the following probably triggers the onset of labor?
A. ACTH in the fetus
B. ACTH in the mother
C. Prostaglandins
D. Oxytocin
E. Placental renin
CHAPTER RESOURCES
Bole-Feysot C, Goffin V, Edery M et al: Prolactin (PRL) and its receptor: Actions, signal transduction pathways, and phenotypes observed in PRL receptor knockout mice. Endocrinol Rev 1998;19:225.
Mather JP, Moore A, Li R-H: Activins, inhibins, and follistatins: Further thoughts on a growing family of regulators. Proc Soc Exper Biol Med 1997;215:209.
Matthews J, Gustafson J-A: Estrogen signaling: A subtle balance between ERα and ERβ. Mol Interv 2003;3:281.
McLaughlin DT, Donahoe PR: Sex determination and differentiation. N Engl J Med 2004;350:367.
Naz RK (editor): Endocrine Disruptors. CRC Press, 1998.
Norwitz ER, Robinson JN, Challis JRG: The control of labor. N Engl J Med 1999;341:660.
Primakoff P, Nyles DG: Penetration, adhesion, and fusion in mammalian sperm–egg interaction. Science 2002;296:2183.
Simpson ER, Clyne C, Rubin G, et al. Aromatase—A brief overview. Annu Rev Physiol. 2002;64:93-127.
Yen SSC, Jaffe RB, Barbieri RL: Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management, 4th ed. Saunders, 1999.