Goran Augustin1, 2
(1)
Department of Surgery Division of Gastrointestinal Surgery, University Hospital Center Zagreb, Zagreb, Croatia
(2)
School of Medicine University of Zagreb, Zagreb, Croatia
4.1 Perforated Peptic Ulcers
4.1.1 Peptic Ulcer in Pregnancy with General Considerations
I have never seen undue activity of a peptic ulcer during pregnancy, but I am very familiar with the opposite state of affairs where ulcer symptoms disappear during pregnancy. Grey Turner
4.1.1.1 History
The first known peptic ulcer was found recently in China in a corpse 2,200 years ago [1] with increasing frequency since then. But there is this gap of 2,000 years since the Greeks started Western medicine and conceived that abdominal pain could be due to an ulcer inside the stomach lining akin to ulcers they were familiar with on the rest of the body. The testing of this hypothesis could, of course, come only from necropsies from about the fifteenth century, when ulcers, first gastric, then in the eighteenth century duodenal, were recorded and became more common and, then later, less frequent in most age groups [2].
4.1.1.2 Incidence
There are approximately 500,000 new cases and 4.5 million people suffering from these diseases each year in the United States [3].
Lower Incidence in Women
It has long been observed that the ratio between men and women who develop duodenal ulcer is 1.9:1 in the United States, whereas in Europe and Asia, this ratio is 2.2:1 [4–7] and 3.1:1 [8], respectively. Incidence in pregnancy is fortunately extremely low due to several factors.
Declining Incidence
With time, there has been a dramatic fall in the prevalence of peptic ulcer disease (PUD) in developed countries. There is an approximately 30–40 % fall in hospitalizations for PUD complications between 1993 and 2006 with a larger reduction in duodenal ulcers (−37.2 %) than gastric ulcers (−19.6 %) [9]. Similar percentage is found in other studies from other countries over the past three decades [9–11]. Duodenal ulcer is more common than gastric ulcer, although the largest decreases in ulcer incidence have been seen in duodenal ulcer [12]. Despite a declining incidence overall of PUD, the incidence of PUD complicated by either bleeding or perforation has remained constant or in fact even increased. Although the data are inconsistent in different countries, data from Finland and the Netherlands suggest that the rate of ulcer complications and the need for emergent ulcer surgery may have increased slightly over the past 30 years [10, 11].
Lower Fertility Rate in Women with Peptic Ulcer
One of the causes of rarity of the disease in pregnancy is that patients with duodenal ulcer, regardless of sex, have a 25 % lower fertility rate compared to the general population (at least in the era before methods of assisted reproduction) [13]. Lower reproduction rate is associated with peptic ulcers of all types. The results revealed that peptic ulcer reduces the reproductive ability of the individual in the sense that the number of children born to affected probands as well as affected parents is smaller than to unaffected individuals. The finding was supported by the observation that the number of children of patients with peptic ulcer was not influenced (i.e., further reduced) by a positive family history of peptic ulcer. By contrast, detailed analysis revealed that childlessness was more frequent in affected probands with a positive family history of peptic ulcer than in affected probands with a negative family history: 26 % compared to 16 %, respectively. A positive family history has thus been shown to participate in the higher rate of childless marriages for subjects suffering from peptic ulcer. At the same time, it has no bearing on the number of children who are born. The number is, however, reduced compared to the average for the general population, as a result of the probands disease.
Incidence in Pregnancy
Cappell and Sidhom reported that of 29,317 pregnant patients, 56 pregnant women who were hospitalized (0.19 %) were found to have severe upper gastrointestinal complaints [14]. Only 2 of 20 of the women undergoing esophagogastroduodenoscopy (EGD) were identified as having PUD (specifically for duodenal ulcers). Tests to evaluate suspected PUD (e.g., upper gastrointestinal series or EGD) that are routine in the general population have been conservatively performed on pregnant women [15, 16]. At the Central Middlesex Hospital, London, during the 11-year period (1951–1961), there were 22,994 confinements; there were duodenal ulcer in two, gastric ulcer in two, and peptic ulceration and hemorrhage in two (with additional dyspepsia in three and gastritis in three) patients [17]. In England and Wales [18], for the years 1951–1960, of 1,193 deaths associated with pregnancy but not due to it, 0.58 % were due to peptic ulceration; while of 8,429 deaths from all causes in women aged 20–49, 0.3 % were due to PUD [19]. Duodenal ulcers in early pregnancy are extremely rare (see Sect. 4.1.1.3). In a 15-year period, there were five cases published [20, 21]. On the contrary, there is higher incidence of maternal dyspepsia during pregnancy in comparison to general population. Dyspepsia is among the most common gastrointestinal diagnoses and is estimated to occur in 14–20 % of adults [22, 23]. Dyspepsia is a very common symptom in pregnancy, particularly in the second part, when 21 % of pregnant women complain of heartburn daily, 52 % at least once a month, and as many as 80 % in the third trimester [24, 25].
4.1.1.3 Pathophysiology
Dyspeptic symptoms usually disappear about the end of the 3rd month of pregnancy, but they may persist till term. The estrogen level and the greatly elevated histaminase concentration afford part of the explanation why symptoms, and especially complications, from peptic ulcer are so rare during pregnancy. Occasionally, more severe indigestion occurs with considerable resemblance to ulcer. Sandweiss et al. in 1939 reported 52 pregnancies in 25 women who were known to have peptic ulcer. In all but one case, the ulcer symptoms disappeared during pregnancy [26]. Clark in 1953 investigated dyspeptic symptoms during 313 pregnancies in 118 women diagnosed as suffering from peptic ulcer before pregnancy. He found that there was a remission of ulcer symptoms in 88 % of the pregnancies. More than half of these women claimed to have been completely symptom-free during the whole pregnancy; the remainder had minor symptoms which they regarded as unconnected with the ulcer. In the remaining 12 %, symptoms persisted which were indistinguishable from those of ulcer, and 1/3 of these were admitted to hospital for treatment of “indigestion.” In no case did hemorrhage or perforation occur during the pregnancy [27].
The benefits derived from pregnancy in women with PUD are apparently short-lived. In Clark’s series, there was recurrence in almost every case within 2 years postpartum [27].
Gastric Position Changes
Hurst and Stewart in 1929 stated that there was no doubt that pregnancy exerts a favorable influence on the symptoms of an ulcer and in some cases appears to lead to actual healing apart from any specific treatment. This they attributed to the mechanical effects of support of the stomach by the rising uterus. This is supposed to relieve the strain on the lesser curvature and improve the local circulation, which promotes healing of any ulcer [28]. Both in James’s case [29] as well as Mulsow and Brown’s case [30], the major accidents took place at a time when the stomach could not have been lifted much higher in the later weeks of pregnancy. Therefore, the mechanical theory by Hurst and Stewart is questionable.
Hypochlorhydria
Balint in 1927 [31] first suggested a general tendency toward increased alkalinity in tissue fluids during pregnancy, and other observers have confirmed that with increased alkalinity, there is found a hypo- or even achlorhydria, especially in the first 6 months of pregnancy; thereafter, the acid values began to rise toward normality and might even reach supernormal figures in the puerperium in certain cases [32–37]. The earliest observations on gastric acidity in pregnancy were made in 1925 by Nakai, who showed that there was a striking diminution in both the free and the total acid content of gastric juice in response to a test meal [32]. This was confirmed by Artz [36], who drew attention to the fact that the lowest secretion of free acid coincides with the period of pregnancy when nausea and vomiting are common. Murray et al. noted with the maximal histamine test that maximal secretion was decreased in the first 30 weeks of pregnancy [38]. This decreased secretion could be due to several factors. Plasma diamine oxidase (histaminase) levels are markedly increased in pregnancy [39], and there is evidence from the 1960s that this substance is related to gastric secretion and may inhibit it [40, 41]. Another important observation is that regurgitation of duodenal contents especially bile is present in only 3 % of pregnant patients despite common nausea and vomiting during (early) pregnancy [33, 42]. Authors share opinion that duodenal regurgitation is not the cause of hypochlorhydria.
Hormonal Influence
Crohn (1927) and others noted that peptic ulcers tend to break down in the puerperium. Winkelstein (1940) thought that the agent responsible for the breakdown might possibly be prolactin, the lactogenic hormone of the anterior pituitary. During gestation, the formation of prolactin is inhibited by the high blood levels of ovarian and placental hormones. He made experimental studies on animals with chemically produced peptic ulcers by treating them with the ovarian hormone theelin. The response was good and the ulcers healed within 10 days. Abrahamson et al. in 1942 treated peptic ulcers in human beings with theelin and, while getting a slightly better immediate response as compared with a number of controls treated on routine lines, found the long-term results no better [43].
One study confirmed previous observation that following ovariectomy, the gastroduodenal mucosa is less sensitive to ulcerogenic stimuli [44]. The reduction by ovariectomy of cysteamine- and indomethacin-induced ulcers of the stomach and the duodenum might relate to the decrease of plasma 17a-estradiol levels, since mucosal damage induced by cysteamine was increased by exogenous administration of the hormone into intact female rats. In contrast, administration of progesterone protected the gastroduodenal mucosa against ulcerogenic treatment with cysteamine or indomethacin. This last finding is in agreement with recent data showing that an increase of endogenous progesterone levels by early pregnancy or the administration of exogenous progesterone decreases the vulnerability of gastroduodenal mucosa to cysteamine [45]. Interestingly, progesterone acts as a protective factor also in male rats.
The maximal levels of chorionic gonadotropins also correspond to the period of decreased gastric secretion. The increased level of estrogen may be a factor, for Truelove has shown that stilbestrol does have a beneficial effect on duodenal ulcers [46]. Others confirmed these results [47, 48]. The equal sex incidence of peptic ulceration in children, the decreased incidence in women during the childbearing years, and the marked increase in incidence at the time of menopause [49] all suggest that the female sex hormones have some relationship to peptic ulceration and that the alterations in the hormones during pregnancy may give rise to an increased resistance to peptic ulceration. Duodenal ulceration and its complications in the presence of high blood levels of both estrogens and progestagens must be due to factors other than changes in acid output. Interestingly enough, Kahlson et al. have shown protection against gastric ulceration during pregnancy in rats in the presence of raised acid output [50]. The resistance against digestion is provided by many factors, most of which are still poorly understood, including mucus, rapid epithelial turnover and migration, secretion of proteolytic ferments in the inactive form in the basal part of the gastric glands, and gastric urease, and it may be that estrogens exert a beneficial influence on duodenal ulceration by altering the secretion of mucus.
Izak [51] and Gryboski [52] noted that plasma pepsinogen rises in the last trimester of pregnancy, reaching a maximum on the first postpartum day. Murray et al. [38] examined the gastric secretion of pregnant women, both in the basal state and after the administration of 0.04 mg of histamine acid phosphate per kilogram of body weight. He noted decreased secretory response during pregnancy, mainly during the first 30 weeks. Two possible explanations for diminished hydrochloric acid secretion have been offered. The first is the antisecretory effect of plasma histaminase, which increases in pregnancy, sometimes as much as 1,000-fold [53]. Barnes [39] showed that plasma histaminase begins to rise about 7 weeks after the last normal menstrual period and that the peak is reached in the 26th–28th weeks of gestation. Preparations of histaminase administered to dogs with Heidenhain pouches were shown to diminish histamine-stimulated secretion [54]. Furthermore, the administration of histaminase inhibitors appears to augment both basal and gastric secretory response to a meal [40].
Way in 1945 attempted to explain the rarity of peptic ulcer and complications in pregnancy by correlating the hypochlorhydria found in these patients with the increased secretion of the anterior-pituitary-like hormones in the urine. He concluded that the greater the secretion of these latter, the more marked the hypochlorhydria. This endocrine explanation appears to be the most likely reason for the rarity of peptic ulcer activity during pregnancy [42]. Same theory was postulated by Horwich in 1958 [55]. Hormonal changes characterized by significant increases in levels of 17-hydroxysteroids and 17-ketosteroids have also been implicated as a possible factor in peptic ulcer in late pregnancy [56]. These and other observations suggest that estrogens may protect against peptic ulceration. This concept is supported back in 1960 by the beneficial effect, demonstrated in when stilbestrol was used in the treatment of men with duodenal ulcer [46].
It has also been suggested that female gestational hormones (particularly progesterone) decrease the rate of ulcer formation by increasing gastric mucus synthesis. An increase in plasma histamine in pregnancy (caused by placental histaminase synthesis) increases metabolism of maternal histamine, thereby reducing gastric acid secretion during pregnancy [39].
Changes in Nutritional and Lifestyle Habits
Avoidance of ulcerogenic factors such as cigarette smoking, alcohol, and drugs including NSAIDs (nonsteroidal anti-inflammatory drugs) all probably contribute to the reduced incidence of PUD in pregnancy.
4.1.1.4 Risk Factors
All known risk factors for peptic ulcers in general population are also risk factors in the pregnant population.
Helicobacter pylori Infection
H. pylori infection and NSAID use account for most cases of PUD. The rate of H. pylori infection for duodenal ulcers in the United States is less than 75 % for patients who do not use NSAIDs. Excluding patients who used NSAIDs, 61 % of duodenal ulcers and 63 % of gastric ulcers were positive for H. pylori in one study. These rates were lower in whites than in nonwhites. Prevalence of H. pylori infection in complicated ulcers (i.e., bleeding, perforation) is significantly lower than that found in uncomplicated ulcer disease. Several studies reported that H. pylori infection is not associated with an increase in dyspepsia, hyperemesis gravidarum, or maternal or neonatal morbidity [57–60].
Medications
NSAID use is a common cause of PUD. These drugs disrupt the mucosal permeability barrier, rendering the mucosa vulnerable to injury. Around 30 % of adults taking NSAIDs have adverse GI effects. Factors associated with an increased risk of duodenal ulcers in the setting of NSAID use include history of previous PUD, advanced age, female sex, high doses or combinations of NSAIDs, long-term NSAID use, concomitant use of anticoagulants, and severe comorbid illnesses. Although the idea was initially controversial, most evidence now supports the assertion that H. pylori and NSAIDs are synergistic with respect to the development of PUD. A meta-analysis found that H. pylorieradication in NSAID-naive users before the initiation of NSAIDs was associated with a decrease in PUD [61].
Corticosteroids alone do not increase the risk for PUD; however, they can potentiate ulcer risk in patients who use NSAIDs concurrently.
The risk of upper GI tract bleeding may be increased in users of the diuretic spironolactone [62] or serotonin reuptake inhibitors with moderate to high affinity for serotonin transporter [63].
Lifestyle Factors
Evidence that tobacco use is a risk factor for duodenal ulcers is not conclusive. Support for a pathogenic role for smoking comes from the finding that smoking may accelerate gastric emptying and decrease pancreatic bicarbonate production. However, studies have produced contradictory findings. In one prospective study of more than 47,000 men with duodenal ulcers, smoking did not emerge as a risk factor [64]. However, smoking in the setting of H. pyloriinfection may increase the risk of relapse of PUD [65]. Smoking is harmful to the gastroduodenal mucosa, and H. pylori infiltration is denser in the gastric antrum of smokers [66].
Ethanol is known to cause gastric mucosal irritation and nonspecific gastritis. Evidence that consumption of alcohol is a risk factor for duodenal ulcer is inconclusive. A prospective study of more than 47,000 men with duodenal ulcer did not find an association between alcohol intake and duodenal ulcer [64].
Little evidence suggests that caffeine intake is associated with an increased risk of duodenal ulcers.
Severe Physiological Stress
Stressful conditions that may cause PUD include burns, CNS trauma, surgery, and severe medical illness. Serious systemic illness, sepsis, hypotension, respiratory failure, and multiple traumatic injuries increase the risk for secondary (stress) ulceration. Cushing ulcers are associated with a brain tumor or injury and typically are single, deep ulcers that are prone to perforation. They are associated with high gastric acid output and are located in the duodenum or stomach. Extensive burns are associated with Curling ulcers. Severe illness and a decreased gastric pH are related to an increased risk of gastric ulceration and hemorrhage.
Hypersecretory States (Uncommon)
The following are among hypersecretory states that may, uncommonly, cause PUD:
· Gastrinoma (Zollinger-Ellison syndrome) or multiple endocrine neoplasia type I
· Antral G-cell hyperplasia
· Systemic mastocytosis
· Basophilic leukemias
· Cystic fibrosis
· Short bowel syndrome
· Hyperparathyroidism
Physiological Factors
In up to one-third of patients with duodenal ulcers, basal acid output (BAO) and maximal acid output (MAO) are increased. In one study, increased BAO was associated with an odds ratio [OR] of up to 3.5, and increased MAO was associated with an OR of up to 7 for the development of duodenal ulcers. Individuals at especially high risk are those with a BAO >15 mEq/h. The increased BAO may reflect the fact that in a significant proportion of patients with duodenal ulcers, the parietal cell mass is increased to nearly twice that of the reference range [67].
In addition to the increased gastric and duodenal acidity observed in some patients with duodenal ulcers, accelerated gastric emptying is often present. This acceleration leads to a high acid load delivered to the first part of the duodenum, where 95 % of all duodenal ulcers are located. Acidification of the duodenum leads to gastric metaplasia, which indicates replacement of duodenal villous cells with cells that share morphological and secretory characteristics of the gastric epithelium. Gastric metaplasia may create an environment that is well suited to colonization by H. pylori.
Genetics
More than 20 % of patients have a family history of duodenal ulcers, compared with only 5–10 % in the control groups. In addition, weak associations have been observed between duodenal ulcers and blood type O. Furthermore, patients who do not secrete ABO antigens in their saliva and gastric juices are known to be at higher risk. The reason for these apparent genetic associations is unclear.
A rare genetic association exists between familial hyperpepsinogenemia type I (a genetic phenotype leading to enhanced secretion of pepsin) and duodenal ulcers. However, H. pylori can increase pepsin secretion, and a retrospective analysis of the sera of one family studied before the discovery of H. pylori revealed that their high pepsin levels were more likely related to H. pylori infection.
Fasting (In General Population)
Most of the studies showed that the frequency of PUD is increased during Ramadan [68–71]. Donderici et al. reported that peptic ulcer complications are more frequent during Ramadan compared to periods before and after Ramadan [72]. There are no studies in the pregnant population. Of three studies, two reported an increase (only in patients with predisposing factors especially dyspepsia) [72, 73], and one reported no change [74] in the frequency of duodenal ulcer perforation during Ramadan in general population. It is interesting that during Ramadan fasting, incidence of male dominance of duodenal ulcer perforation significantly decreases. This observation is found in two studies [72, 73]. Up to date, there are no such studies in pregnant population.
Additional Risk Factors
Other risk factors may be associated with PUD and are listed in Table 4.1.
Table 4.1
Some of the less common causes of peptic ulcer disease in general population
|
Hepatic cirrhosis |
|
Chronic obstructive pulmonary disease |
|
Allergic gastritis and eosinophilic gastritis |
|
Cytomegalovirus infection |
|
Graft versus host disease |
|
Uremic gastropathy |
|
Henoch-Schönlein gastritis |
|
Corrosive gastropathy |
|
Celiac disease |
|
Bile gastropathy |
|
Autoimmune disease |
|
Crohn’s disease |
|
Other granulomatous gastritides (e.g., sarcoidosis, histiocytosis X, tuberculosis) |
|
Phlegmonous gastritis and emphysematous gastritis |
|
Other infections (Epstein-Barr virus, HIV, Helicobacter heilmannii, herpes simplex, influenza, syphilis, Candida albicans, histoplasmosis, mucormycosis, and anisakiasis) |
|
Chemotherapeutic agents, such as 5-fluorouracil (5-FU), methotrexate (MTX), and cyclophosphamide |
|
Local radiation resulting in mucosal damage, which may lead to the development of duodenal ulcers |
|
Use of crack cocaine, which causes localized vasoconstriction, resulting in reduced blood flow and possibly leading to mucosal damage |
4.1.1.5 Clinical Presentation
Peptic ulcer is rare and difficult to diagnose during pregnancy. Obstetric patients as a rule are not questioned closely with respect to past gastrointestinal symptoms. Epigastric distress, heartburn, nausea, and vomiting are frequent complaints during normal pregnancy and, therefore, often overlooked. These symptoms are also associated with hyperemesis gravidarum and hiatal hernia, both more prevalent than peptic ulcer in pregnancy. On the contrary to peptic ulcer itself, dyspepsia is among the most common gastrointestinal diagnoses and is estimated to occur in 14–20 % of adults [22, 23]. Dyspepsia is a very common symptom in pregnancy, particularly in the second part, when 21 % of pregnant women complain of heartburn daily, 52 % at least once a month, and as many as 80 % in the third trimester [24, 25].
Cardinal symptoms of PUD are upper abdominal pain, nausea, and vomiting. The pain is often epigastric and worse at night. In the presence of a gravid uterus (and especially when labor ensues), it can be quite difficult for patients to localize pain. Unlike gastroesophageal reflux disease, the pain is not exacerbated by recumbence or associated with regurgitation. Although nausea and vomiting occurs in 50–80 % of normal pregnancies, it is uncommon for these symptoms to persist beyond 20-week gestation. Nausea and vomiting of pregnancy is classically most intense in the morning while PUD symptoms are worse nocturnally and postprandially during the day. PUD symptoms also get worse with increasing gestation and are therefore usually most severe in the third trimester. Occasionally, PUD may present with hematemesis. Uncomplicated PUD produces minimal physical signs.
The symptoms of peptic ulceration are improved during pregnancy in many women. Relief occurs early in pregnancy, but unfortunately, the symptoms frequently recur following delivery [28, 29].
4.1.1.6 Diagnosis
Diagnostic modalities are the same for pregnant and general population. The most common diagnostic tool of nonemergent presentation is esophagogastroduodenoscopy because it can obtain samples for histopathological examination as well as H. pylori presence. The procedure is safe in pregnancy if no sedative medications are used which can lead to fetal hypoxia [75, 76]. American Society for Gastrointestinal Endoscopy (ASGE) guidelines state two indications for EGD:
· Significant or continued GI bleeding
· Severe or refractory nausea and vomiting or abdominal pain
Therefore, if only uncomplicated ulcer is suspected, there is no need for endoscopy during pregnancy or it should be postponed to the second trimester [77].
4.1.1.7 Therapy
Pharmacological treatment is the same in pregnant and general population (see Sect. 4.1.2.5). All classes of medications are safe for the fetus, and no increase in incidence of fetal anomalies was found on large samples [78]. No severe side effects were observed in any of the mothers or their newborns. No malfunctions or malformations were observed in the newborns. Follow-up of the children between 2 and 12 years showed normal development in all children [79]. Recent studies confirmed that higher rate of congenital anomalies was not found in the offspring of mothers with PUD [78]. One study showed that severe chronic dyspepsia in early pregnancy and drug treatment for this was not associated with a higher risk of congenital malformations except possibly isolated rectal/anal atresia/stenosis [80].
4.1.1.8 Prognosis
Perforated gastroduodenal ulcers in pregnancy, as in nonpregnant condition, should be divided into benign peptic ulcers, malignant ulcers/perforated carcinomas, and specific forms such as Zollinger-Ellison syndrome. The division is necessary because therapeutic principles and prognosis between these groups are different.
Nationwide, population-based study revealed that maternal PUD was independently associated with a 1.18-, 1.20-, and 1.25-fold increased risk of having babies with low birth weight, preterm delivery, and small for gestational age, respectively, after adjusting for family income and maternal, paternal, and infant characteristics. With the comparison of the PUD women without treatment with the unaffected mothers, gestational PUD was found to have an adverse impact on pregnancy outcomes. However, in further examining women with treated PUD, authors were unable to identify improved effects of PUD medication on the risks of adverse neonate outcomes [81]. It remains unclear what factors elevate the risk of adverse birth outcomes among patients with PUD. The possible role of diet and nutrient absorption deserve more examination. In animal models, maternal starvation decreased the extent of metabolic substrate produced by the mother and provided to the fetus, retarding fetal intrauterine growth [82]. Glucose, transmitted from the mother to fetus, is the main energy substrate for intrauterine growth [83].
Whereas glucose is produced by maternal metabolism, dietary restriction or maternal hypoglycemia decreases availability of metabolic fuel and consequently slows fetal growth [84, 85]. Likewise, low micronutrient intake during pregnancy is associated with adverse neonatal outcomes such as preterm delivery [82]. In response to symptoms of anorexia, abdominal distention, epigastric pain, and postprandial vomiting, mothers with PUD during pregnancy may restrict their dietary intake to avoid the discomfort. The risk of constrained fetal growth and adverse birth outcomes might be elevated accordingly. Stress might also contribute to the link between gestational PUD and adverse pregnancy outcomes. Stress is strongly associated with PUD because threats to homeostasis prompt an adaptive or allostatic response [86]. Maternal vasoconstriction, resulting from the release of catecholamines in exposure to stress, might also obstruct the transmission of oxygen and vital nutrients to the fetus [87]. Fetal central nervous system and particularly glucocorticoid brain receptor development might subsequently be affected [88, 89]. Previous literature indeed demonstrated a significant relationship between maternal prenatal stress and infants with low birth weights and decreased gestational age at birth [89]. Thus, women with PUD might be those who perceive or experience more stressful circumstances. The further exposure of their fetuses to stress and elevated levels of adrenal hormones might consequently elevate the risk of negative birth outcomes. Furthermore, Chen et al. identified increased risk of adverse pregnancy outcomes among mothers with PUD who took no medication for it during pregnancy [81]. Meanwhile, no significant difference in outcomes was observed for those who did take medication during pregnancy. PUD medications, such as H2 blockers or proton pump inhibitors [90–92], are probably safe during pregnancy according to current clinical data but with the possibility that the lack of insignificant difference is due to the relatively small sample size. The trend toward slightly increased though insignificant risk of low birth weight and preterm birth might reflect more severe PUD symptoms among women who were prescribed PUD medication.
4.1.1.9 Specific Considerations
Zollinger-Ellison Syndrome
Zollinger-Ellison syndrome (ZES), described in 1955, is an ulcerative disease of the upper gastrointestinal tract that includes high levels of gastrin and gastric acid. There is little information on the management of pregnancy in patients with pancreatic endocrine tumors such as ZES. This has occurred because the syndromes are uncommon (i.e., ten cases/million population/year); until last decades, these patients frequently died soon after the diagnosis, which was often established only late in the disease course and the hormonal syndrome often caused severe metabolic or nutritional deficiencies that may have interfered with pregnancy [93–95]. However, at present, because of earlier diagnosis and the increased ability to medically control the hormonal symptoms, especially in patients with ZES with potent gastric acid antisecretory drugs, these patients are living longer [93, 95–97] and women with the disorder more frequently become pregnant. The tendency of the tumor to grow slowly enables the physician to focus on symptomatic treatment. Gastrin levels do not change significantly during pregnancy and thus are useful for the diagnosis and follow-up of this syndrome [98]. There is a controversy whether pregnancy offers protection against ZES. Some have reported the absence of symptoms of ZES during pregnancy [99, 100], while Ezeh et al. [101] reported a case of exacerbation during pregnancy that required i.v. omeprazole treatment. The patient by Mayer et al. had been treated operatively and had low gastrin levels requiring high doses of omeprazole. This fact might strengthen the theory that pregnancy does not offer protection against ZES [102].
The management of pregnant patients with an asymptomatic pancreatic endocrine tumor syndrome such as ZES presents a number of unique problems. ZES is the most common symptomatic malignant pancreatic endocrine tumor [93]. Similar to the other pancreatic endocrine tumors, these patients have two different treatment problems [93]. First, symptoms caused by the ectopic hormonal release must be controlled, and, second, treatment must be directed against the tumor, which in all the syndromes, except insulinoma, is malignant in 30–90 % of cases [93]. In ZES the ectopically released gastrin causes gastric acid hypersecretion that, if untreated, results in severe ulcer disease, malabsorption, and frequently severe gastroesophageal reflux disease [93–95]. The gastrinoma is malignant in 60–90 % of cases [93–95], and 34 % of patients have liver metastases [93]; however, in most patients the tumor grows relatively slowly [97]. Because of the slow rate of progression of most gastrinomas, the primary problem during pregnancy in patients with ZES is controlling the severe gastric acid secretion. This problem is complicated by the large volume of gastric acid secretion, necessitating daily gastric acid antisecretory drug treatment [93, 96]; the requirement for high doses of these drugs in many patients [96]; and the unknown safety profiles of any of the gastric antisecretory drugs during pregnancy, especially in high doses.
It is possible for patients with ZES to have pregnancies that are not complicated by gastric acid hypersecretion. If the ZES is diagnosed before pregnancy, curative resection with parietal cell vagotomy may obviate the need for gastric antisecretory drugs. If metastases are present or the diagnosis of ZES is made after conception, ranitidine in the lowest possible dose should be used to control acid secretion. If acid secretion in uncontrolled, the dose may be increased or omeprazole may be used [103].
Antacids are generally ineffective in the management of ZES and thus are not a realistic option. The histamine H2 receptor antagonists and H+-K+ adenosine triphosphatase inhibitors can control gastric hypersecretion in all patients with ZES [96]; however, high doses of these drugs are frequently required [93, 96]. In various studies of patients with ZES, the mean dose of cimetidine required was 3.6 g, for ranitidine it was 1.2 g, and for famotidine it was 0.25 g, all of which were more than four times the doses required for the treatment of idiopathic PUD [93, 96]. Similarly, the median dose of omeprazole or lansoprazole required is 60 mg, which is also higher than the 20 or 30 mg, respectively, used in routine idiopathic PUD [96]. The safety of these drugs in pregnancy is the central issue in trying to decide the proper approach to the management of the acid hypersecretion in these patients during pregnancy. Studies have shown that the high doses used in ZES cimetidine can cause antiandrogen side effects in some patients [104]. Ranitidine, however, has not been shown to possess these antiandrogenic effects in pregnant rats or in patients with ZES even at high doses [105]. There are case reports describing the safe use of cimetidine and ranitidine in pregnant patients with gastroesophageal reflux disease, hyperemesis gravidarum, Mallory-Weiss tears, and active PUD [106–108]. Detailed strategy of treating patients with ZES prior to and during pregnancy could be found in the article by Stewart et al. [103].
Helicobacter pylori
H. pylori infects the human stomach, causing gastritis, peptic ulcer, and gastric cancer. H. pylori infection has also been related to extra-gastric disorders. During pregnancy, preferential induction of Th2-type cytokines downregulates Th1-type responses, allowing fetal survival. The results suggest that H. pylori infection can induce activation of resident uterine immune cells and/or recruitment of cells at the endometrial level. It can be hypothesized that the local Th1-type response induced by H. pylori infection could alter the systemic Th1-/Th2-type cytokine balance at sites under particular physiopathological conditions of active tissue and/or vascular formation, such as pregnancy. This is the first evidence in an animal model of the possible influence of H. pylori infection on pregnancy. Further work is required on its mechanism and its relevance for humans [109]. Transmission of H. pylori infection from the mother to infant was not detected by culture in animal study, suggesting that decreased baby weight may be due to decreased milk supply or altered nutrition from the mother [110].
Physiological and epidemiological evidence suggests that H. pylori may interfere with iron metabolism, lowering it [111–114]. In the study by Weyermann et al., the reduction of hemoglobin levels during pregnancy in the presence of H. pylori infection seemed to be slightly higher among women with iron therapy during pregnancy compared with women without [115]. Even though the difference between both groups was not statistically significant, this pattern would be consistent with the hypothesis of a possible increase in bacterial density by iron therapy, which might in turn reduce the benefit from iron therapy, because microbiologic and ferrokinetic studies suggested that outer membrane receptors of H. pylori in vitro are able to capture iron from human lactoferrin and use it for growth [116]. However, this hypothesis must be confirmed.
Women who were infected with H. pylori were generally shorter than women who were not infected. Moreover, women who gave birth to babies with intrauterine growth retardation were also shorter than women who gave birth to normal-sized babies. Many studies have shown that close contact and overcrowding among family members promotes the transmission of H. pylori infection [117–119]. Therefore, the possibility exists that an infected mother may more often transmit H. pylori to her infant and thereby continues a vicious cycle of growth restriction. The possible mechanisms by which H. pylori may affect fetal growth are speculative. However, it is conceivable that H. pylorimay be linked with an increase in symptoms including dyspepsia [120], nausea [121], or vomiting [122, 123], because of underlying undiagnosed PUD, which in turn may affect maternal appetite and therefore restrict the growth of the fetus, although this was not determined in this study. Another possible mechanism linking intrauterine growth retardation with H. pylori infection may be the effect of chronic H. pylori infection upon the vascular system. Acute atherosclerotic changes have been noted in placental and uterine spiral arteries in cases with intrauterine growth retardation [124]. Previous studies have suggested that H. pylori infection may increase platelet aggregation and fibrinogen, as well as having an effect on lipid peroxidase [125–128]. Therefore, chronic H. pylori infection might induce vascular disease, which in turn may affect the placenta and thereby cause intrauterine growth retardation. Therefore, direct link between perforated peptic ulcer and abnormal pregnancy and/or fetal consequences could not be proved because acute/chronic H. pylori infection and other potential confounders could have the same or even more influence on negative pregnancy outcomes.
It has been shown in mice that H. pylori-infected mice show a decrease in implantation rates and their offspring are of low birth weight [109]. Infection with H. pylori cytotoxin-associated gene (CagA)-positive strains has been shown to cause a severe inflammatory response and significant neutrophil infiltration in the gastric mucosa [129]. There is statistically significant relationship between CagA-positive strains of H. pylori and early pregnancy loss (EPL) which might be explicable on the basis of general inflammatory reaction to infection. Concentrations of IL-1β, IL-8, and TNF-α were all significantly higher in H. pylori-positive gastric mucosa samples [130]. These cytokines may cause systemic inflammation that could affect the integrity of the fetoplacental unit and threaten the welfare of the fetus [131]. It was shown that poor oral hygiene is associated with a history of miscarriage [131], possibly due to systemic inflammatory response to oral bacterial infection. It may be assumed that a parallel mechanism underpins the ELL in women infected with CagE-positive H. pylori strains.
In infertile human males, H. pylori infection was shown to be associated with low sperm quality compared to uninfected patients [132]. The pathogenicity of an H. pylori isolate depends on strain-specific factors [133]. The Cag pathogenicity island, for which CagA is the marker, has been associated with both duodenal ulcer and gastric cancer [134], and infection with CagA-positive strain is generally associated with a higher level of inflammatory mediators compared to CagA-negative strains. In CagA-positive male patients, a significant reduction in sperm motility was observed along with increased apoptosis and necrosis [132] with two hypotheses explaining this finding: inflammatory reaction to infection and the immune reaction between H. pylori and the sperm antigen [135].
Peptic Ulcer Disease Complicated by Gastric Outlet Obstruction
Several such cases are described [136, 137]. Ideally, the operation during pregnancy should be avoided due to surgical stress and possible postoperative nutritional deficiencies to the mother and fetus. Gastric outlet obstruction should be treated with endoscopic balloon dilatation with additional procedures such as endoscopic needle-knife radial incisions [138]. Duration of the therapeutic effect depends on the underlying cause of the gastric outlet obstruction, but most studies report therapeutic effect in months which is enough to postpone the definitive treatment by operation after delivery [139]. If malignancy is confirmed, surgery is indicated by oncologic principles in pregnancy.
4.1.2 Perforated Peptic Ulcer
I cannot remember a perforated gastric or duodenal ulcer during pregnancy. Sir Gordon-Taylor
Every doctor, faced with a perforated duodenal ulcer of the stomach or intestine, must consider opening the abdomen, sewing up the hole, and averting a possible or actual inflammation by careful cleansing of the abdominal cavity. Johann von Mikulicz-Radecki, 1884
4.1.2.1 History
For thousands of years, healthy people have had acute abdominal pain, nausea, vomiting, and diarrhea followed by death in a few hours or days. Often these symptoms were contributed to poisoning, and people have been sent to prison for this [140]. King Charles I’s daughter, Henriette Anne, died suddenly in 1670 (at age 26) after a day of abdominal pain and tenderness. Since poisoning was suspected, autopsy was performed revealing peritonitis and a small hole in the anterior wall of the stomach. However, the doctors had never heard of a perforated peptic ulcer (PPU) and attributed the hole in the stomach to the knife of the dissector [141]. Necropsies were first allowed since 1500 and became more common between 1600 and 1800 [141, 142]. As a consequence, more often perforation of the stomach was observed. Johann Mikulicz-Radecki (1850–1905), often referred to as the first surgeon who closed a perforated peptic ulcer (PPU) by simple closure in 1884, said: “Every doctor, faced with a perforated duodenal ulcer of the stomach or intestine, must consider opening the abdomen, sewing up the hole, and averting a possible or actual inflammation by careful cleansing of the abdominal cavity” [143]. Robert Daniel Mussey (Fig. 4.1) was one of the first, in 1927, who reported two cases of peptic ulceration in 370 operations during pregnancy at the Mayo Clinic in a period of 10 years [145]. It is not known whether these two operations were made in elective or emergent settings.

Fig. 4.1
Robert Daniel Mussey (1884–1958) is a physician in a family of six generations of physicians (cropped picture) [144]. He guided the development of an obstetrics/gynecology department at the Mayo Clinic and was Professor of Obstetrics and Gynecology there until he retired in 1950
4.1.2.2 Considerations in General Population
Remarkable changes have occurred in the sex and age incidence of PUD in North-West Europe. The fluctuations over the previous 150 years were studied by Jennings in 1940 [146]. He examined the incidence of perforations, which provide perhaps the most uniform index of the incidence of ulcers for the total period. His interpretation suggested that during this period, there had been three observable syndromes: perforations of acute gastric ulcers in young women, perforations of duodenal ulcers in young and middle-aged men, and perforations of gastric ulcers in older men [146].
Perforations began to be noted with increasing frequency at the beginning of the nineteenth century. Half of all perforations were then in young women in their twenties, and these reached a peak in the latter half of the century. They seemed to be acute gastric ulcers, which caused death from perforations near the cardia or from hemorrhage [146, 147]. By the end of the century, this condition had begun to disappear. But even in 1905, the Registrar General was able to write: Gastric ulcer does not appear frequently as a cause of death until the attainment of the reproductive period, when the female rate greatly exceeds the male, while at later ages the male rate is in excess [148].
The common perforations of today made an appearance only at the beginning of the twentieth century; these are juxtapyloric ulcers occurring mainly in young and middle-aged men [149]. Studies up to 1955 show a continuing trend of increase in perforations of peptic ulcers in men [150]. The incidence of perforation during the 1940s in the two sexes was much greater in men, varying from 25:1 [43, 151–155].
In the 1950s, however, there were signs that the volume of peptic ulcer had at last reached a peak and was beginning to fall. A halt in mortality from gastric ulcer was noted in the early 1950s, and it then seemed possible to ascribe this to better treatment [156]. Subsequently the death rate has continued to fall, and sickness statistics show the same trends. The decline is found in sickness rates reported from general practice, from the Army, and from insurance certificates [157–159].
Trends for duodenal ulcer are similar but follow about 5 years behind. In the mid-1950s, death rates reached a plateau and then began to fall. This fall can also be seen from the census of clinically diagnosed peptic ulcers in York and from the duration and the number of spells of sickness absence [160]. As yet it does not appear in statistics of the last decade from general practice and from the Army, both of which showed stable rates [157–159]. All these trends together suggest that we are observing a recession of the PUD. This has affected the age groups unequally. Since the war, mortality from gastric and duodenal ulcers has declined in young men and women, although up to 1962, it was still rising at ages over 65 (Fig. 4.2a–d). One possible explanation is that the fluctuations in peptic ulcer rates represent a cohort phenomenon and that each generation has carried its own particular risk of bearing ulcers throughout adult life. In order to examine this hypothesis, the experience of each generation or cohort must be followed separately through its life cycle.
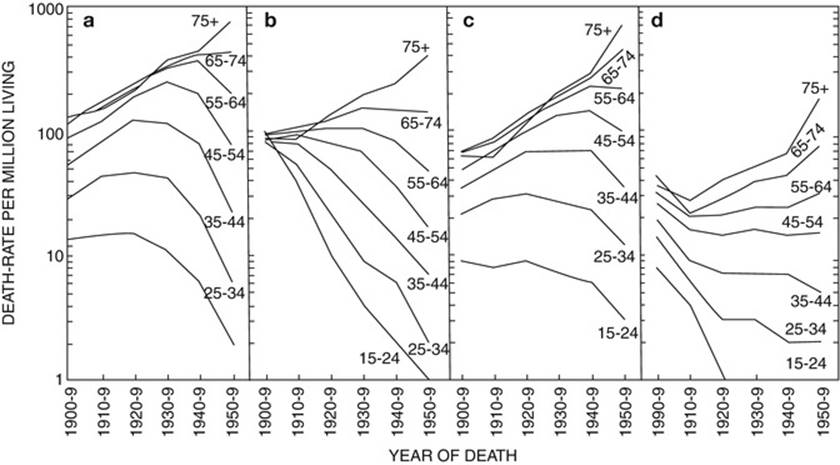
Fig. 4.2
Deaths from peptic ulcer by age and sex and year of death. (a) Gastric ulcer: males. (b) Gastric ulcer: females. (c) Duodenal ulcer: males. (d) Duodenal ulcer: females; mean rates for 10-year periods were calculated from the Annual Reviews of the Registrar General. Populations include non-civilians. Correction factors for the pre-1940 data to allow for the change in death certification (males 1.034, females 1.042) have not been used. Log graphs [161]
Because of the success of medical therapy in the management of PUD, surgery has a very limited role, and elective peptic ulcer surgery has been virtually abandoned. The number of elective operations for PUD dropped more than 70 % in the 1980s; 80 % of these procedures were emergent operations [162]. The lifetime prevalence of perforated peptic ulcer (PPU) has been estimated at 5 % [163]. Currently, mortality and morbidity following PPU are substantial, and mortality rates as high as 25–30 % have been reported [164–167]. Several prognostic factors and scoring systems for PPU have been examined [166, 168–172]. The mortality incidence doubles for every 6-h period from the time of perforation to the time of surgery; after 24 h the mortality rate is maintained at the high rate of over 60 %. Sepsis is frequent and a leading cause of death in patients with PPU, and some of the reported prognostic factors are associated with the sepsis syndrome [173, 174]. The authors of the first surgical procedures for PPU were as follows:
· 1892 resection: Heusner
· 1894 oversaw: Dean
· 1937 omental patch: Graham
· 1990 laparoscopy: Mouret
4.1.2.3 Perforated Peptic Ulcer in Pregnant Population
History
In pregnant population, Chabannes [175] in 1903 first drew attention to this subject, followed by Szenes [176]. This point is further buttressed by the seminal work of Hooker in 1933, in which only one case of duodenal ulcer was recorded following 1,564 puerperal deaths from 348,310 pregnancies [177]. Sandweiss et al. have subsequently reviewed the topic and found nine PPUs [178]. Howkins in 1950 quoted Professor Grey Turner’s statement that he has never seen undue activity of a peptic ulcer during pregnancy, but is very familiar with the opposite state of affairs where ulcer symptoms disappear during pregnancy; also Sir Gordon-Taylor’s statement that he cannot remember a perforated gastric or duodenal ulcer during pregnancy [179] and it must be extremely rare to meet with this complication. Scott in 1945, discussing the differential diagnosis of acute abdominal lesions in pregnancy, does not even mention ulcer perforation as a possibility [180].
Incidence
Sandweiss et al. found only one case of perforated duodenal ulcer in 70,310 pregnancies in Detroit in the period 1928–1937 and also one case of perforated gastric ulcer in 348,310 pregnancies over a period of 3 years in New York. Both patients died [178]. The low incidence of peptic ulceration in pregnancy has been demonstrated in a number of series from 1939 to 1955; a compilation of four of these has shown that among 233,650 deliveries, only 11 patients had peptic ulcers [28, 181–183], and among 1,564 maternal deaths in 348,310 pregnancies, only one death was due to peptic ulceration [184]. In early reports perforation was more frequent than bleeding during pregnancy [178]. Reports have found 13 cases of PPUs (nine duodenal and four gastric) during pregnancy and the first week after delivery [185]. Nine of the 13 mothers died, and the four cases in which the mother survived were reported from this country up to 1961 by James [29], Horwich [55], Ross [186], and Burkitt [187]. Only 24 cases of PPUs have been described up to 1966 [19, 29, 55, 154, 178, 186–193]. Up to 1971, 31 perforations (and 32 cases of hemorrhage) proved from peptic ulcer which occurred during pregnancy have been reported [194]. In the last 20 years, there are several more cases published [195, 196].
Risk Factors
Risk factors for PPU are the same as for the peptic ulcer itself. Fasting can be a risk factor [197]. Even a case of perforated gastric ulcer was described after adjustable gastric banding. The case does not define localization, macroscopic appearance, and whether the ulcer was peptic or related to silicone ring and local ischemia (marginal ulcer) [198].
Ulcer Type
Summary of case reports show that most cases during pregnancy are located in the first part of the duodenum on the anterior surface which is a common presentation in young nonpregnant population (Table 4.2).
Table 4.2
Important data of published studies of perforated peptic ulcers during pregnancy (without puerperium)
|
Study |
Age |
Pregnancy (weeks) |
Ulcer type |
Duration (hours) |
Operation |
Mother/birth |
Child |
|
James, 1948 [29] |
24 |
36 |
Duodenum, anterior |
10 |
Live, vaginal |
After 4 days, live |
|
|
Burkitt, 1961 [187] |
38 |
31 |
Duodenum |
10 |
Partial gastrectomy |
Live, vaginal |
Less than 24 h, one twin alive |
|
Horwich, [55] |
30 |
31 |
Duodenum, anterior |
60 |
Sutures |
Before operation, dead |
|
|
Lindell and Tera, 1962 [188] |
26 |
9 months |
Pylorus, greater curvature, 1 cm |
Live, vaginal |
Less than 24 h, live |
||
|
Winchester and Bancroft, 1966 [193] |
34 |
Duodenum |
Roscoe Graham |
Live, vaginal |
37th week, live |
||
|
Gali et al., 2011 [197] |
16 |
28 |
Duodenum, anterior |
Roscoe Graham |
Live, vaginal |
After 3 days, died |
|
|
Goh and Sidhu, 1995 [195] |
Duodenum |
||||||
|
Hsu et al., 2011 [196] |
23 |
20 |
96 |
Live, vaginal |
Live |
||
|
Segal, 1959 [199] |
29 |
6 |
Pylorus, anterior |
18 |
Sutures |
Live, lost for follow-up after 24 weeks of pregnancy |
|
|
Essilfie et al., 2011 [200] |
27 |
38 |
Duodenum, anterior |
Roscoe Graham |
Live, vaginal |
38th week, live |
Clinical Presentation
Clinical presentation is similar to nonpregnant population: acute, severe abdominal pain, and sometimes with vomiting. It is difficult to see abdominal distension in advanced pregnancy.
Perforated Peptic Ulcer in the Puerperium
PPU rarely occurs in the puerperium. Anderson first described such a case in 1942, when a 29-year-old woman developed abdominal pain a few hours after a normal delivery and died in septic shock due to perforated duodenal ulcer [154]. The relative rarity of perforated duodenal ulcer in pregnancy and puerperium often causes delay in both diagnosis and surgical intervention [201]; this is made worse considering that the usual signs of perforation may be diminished or subtle in the puerperium [186, 202]. The symptoms may commonly be attributed to obstetric-related causes, and therefore, a high index of suspicion is necessary. However, earlier diagnosis may be enabled with the conventional plain abdominal X-rays and ultrasound scan [203].
In the last 40 years, there are only several cases published. There is approximately equal number of these perforations developed after Cesarean section and vaginal delivery. The important figure is that after Cesarean section, these perforations occur during the first several days of puerperium [177, 204–207]. In the immediate postoperative period, abdominal symptoms may be interpreted as constitutional symptoms emanating from pregnancy or surgery [202]. Often a presumptive diagnosis of paralytic ileus is made and in some instances that of puerperal sepsis, which could result in a relaxed approach in dealing with such symptoms.
After vaginal delivery, there are also several cases with half of patients being older (41 and 42 years old [201, 208]) and two were younger (28 and 29 years) [154, 186]. In this group perforated ulcer also developed during first days after delivery.
There are two reports of gastric perforation [209, 210] and one perforation of duodenal ulcer in the puerperium, but most of the medical data were not available (Table 4.3) [211].
Table 4.3
Published studies of perforated peptic ulcers during puerperium
|
Study |
Age |
Days after delivery |
Ulcer type |
Duration (hours) |
Operation |
Mother/birth |
Child |
|
Anderson, 1942 [154] |
29 |
4 h |
Duodenum |
Died, vaginal |
Live |
||
|
Ross, 1958 [186] |
28 |
1 |
Duodenum, anterior |
60 |
Live, vaginal |
Live |
|
|
McGarvey et al., 1952 [208] |
41 |
2 |
Duodenum |
||||
|
Parry, 1974 [211] |
Duodenum |
||||||
|
Munro and Jones, 1975 [201] |
42 |
4 |
Prepyloric |
70 |
Sutures |
Vaginal |
|
|
Kaczmarek, 1970 [205] |
C-section |
||||||
|
Opitz, 1971 [209] |
Gastric |
||||||
|
Gaĭstruk et al., 1980 [210] |
Gastric |
||||||
|
Uchikova et al., 2004 [204] |
Duodenum |
C-section |
|||||
|
Engemise et al., 2009 [177] |
29 |
Duodenum, anterior |
50 |
Omental patch |
Live/C-section |
Live |
|
|
Alabi-Isama et al., 2009 [206] |
|||||||
|
Sule and Omo-Aghoja, 2010 [207] |
25 |
3 |
Duodenum, anterior |
7 days |
Omental patch |
Live/C-section |
Live |
There are several diagnostic problems in puerperium. Nonspecific abdominal pain is experienced by 98 and 92 % of primiparous and multiparous women, respectively, in the puerperium [212]. Another fact is that about 60 % of all post-laparotomy patients will have evidence of pneumoperitoneum and this will take 1–24 days to be absorbed [213]. This is important for patients with abdominal pain after Cesarean section making the diagnosis more difficult. In such cases water-soluble contrast swallow will show a free peritoneal leak.
4.1.2.4 Diagnosis
The only role radiology would have in the pregnant patient with PUD is confirmation of perforation. The usual approach to the diagnosis of pneumoperitoneum is to perform an abdominal series, but this would involve irradiation of the fetus in the pregnant patient. In a series of 100 patients with known pneumoperitoneum, Woodring and Heiser showed that the upright lateral chest radiograph confirmed pneumoperitoneum in 98 % of the cases. This was more sensitive than the upright posteroanterior chest radiograph, which showed the pneumoperitoneum in only 80 % of the cases [214]. The performance of a lateral chest radiograph excludes the fetus from the direct beam; if negative for the presence of free intraperitoneal air, this would support more conservative management. In the presence of strong clinical suspicion for intra-abdominal disease, the decision to perform further imaging, such as abdominal CT, versus surgical exploration will have to be made on an individual basis.
4.1.2.5 Treatment
The treatment of PPU consists of surgical intervention and perioperative pharmacological gastric acid suppression.
Surgical Treatment
In the first half of the twentieth century, there were cases of PPU in pregnancy treated conservatively. Only 24 cases of PPUs have been described up to 1966 [19, 29, 55, 154, 178, 186–192]. In that series 16 patients were treated medically (nasogastric suction, nil by mouth, and antibiotics) with 16 maternal and 11 infant deaths. As in nonpregnant population, conservative therapy of PPU is not an acceptable option. Omental patch repair with H. pylorieradication (if present) is the standard of care for sealing duodenal perforations and preventing reperforations. Postoperative complications such as intra-abdominal abscess [207] should be drained as soon as possible. If the adjustable gastric band is the cause of marginal or peptic ulcer, it should be removed during emergency operation [198].
Perioperative Gastric Acid Suppression
Histamine2 Receptor Antagonists (H2RA)
The H2RAs are the most commonly used and safest medications for the pregnant woman with heartburn not responding to lifestyle modification and nonabsorbable medication. All four drugs (cimetidine, ranitidine, famotidine, and nizatidine) are FDA (Food and Drug Administration)-approved category B drugs for pregnancy.
Cimetidine and ranitidine. Cimetidine and ranitidine have had considerable use in pregnancy over the last 30 years with an excellent safety profile. Only ranitidine’s efficacy has been specifically studied during pregnancy for heartburn [215]. No adverse pregnancy outcomes or drug reactions were noted. Cimetidine has a weak antiandrogenic effect in animals, as evidenced by a reduction of the size of testes, prostate glands, and seminal vesicles [216]. Ranitidine has no antiandrogenic activity in animals [105]. Neither H2RA has reports of human sexual defects in infants. To date, the safety of cimetidine and ranitidine has been assessed in over 2,000 pregnancies in database studies not sponsored by the manufacturers. In the surveillance study of 229,101 pregnancies in the Michigan Medicaid recipients between 1985 and 1992, similar rate of major birth defects was detected (4.3 % with cimetidine, 4.5 % with ranitidine, and 4.3 % in women taking no medications during their pregnancies) [217]. In a 1996 prospective cohort study, 178 women exposed during pregnancy to H2RAs were matched with 178 women with no exposure with similar maternal age, smoking, and alcohol history [91]. Among these subjects, 71 % took ranitidine, 16 % cimetidine, 8 % famotidine, and 5 % nizatidine. The outcomes of both groups were similar in terms of live births, spontaneous or elective abortions, gestational age at delivery, birth weight, or major malformation. The latter rate was 2.1 % in subjects exposed to H2RAs versus 3.0 % in the nonexposed cohorts. The Swedish Medical Birth Registry in 1998 reported on 553 babies delivered by 547 women using various acid-suppressing medications in early pregnancy [218]. Seventeen infants had congenital defects (3.1 %) compared with the expected rate of 3.9 % in the Registry among women not taking any medications. Of the 17 infants, ten had been exposed to PPIs, six to H2RAs, and one to both classes of drugs. Two birth defects (5.7 %) in 35 infants exposed to cimetidine and six defects (3.8 %) in 156 infants exposed to ranitidine were reported. Overall, the odds ratio for malformations after H2RAs was 0.46 in contrast to 0.91 for infants exposed to PPIs, early during pregnancy. Finally, two databases, one from England and another from Italy, were combined in a study published in 1999, which compared the incidence of congenital malformations in infants and women receiving cimetidine, ranitidine, or omeprazole during the first trimester of pregnancy with unexposed control women [92]. The relative risk of malformation (adjusted for maternal age and prematurity) was similar among all three drugs: cimetidine 1.3, ranitidine 1.5, and omeprazole 0.9. In summary, cimetidine and ranitidine have not been associated with an increased risk of congenital malformations. Ranitidine is the only H2RA with documented efficacy in pregnancy. Some authorities have recommended that cimetidine not be used during pregnancy because of possible feminization as observed in some animals and nonpregnant humans [219].
Famotidine and nizatidine. There are much less reported safety data with these latter H2RAs than cimetidine and ranitidine. Animal studies with famotidine revealed no fetal toxicity or teratogenicity [220]. However, pregnant rabbits with the equivalent of 300 times the recommended human dose of nizatidine encountered abortions, low fetal weights, and fewer live fetuses [221]. On the contrary, rat studies found no adverse effects on the fetal pups [222]. In the Michigan Medicaid Surveillance Study, 6.1 % of fetuses exposed to famotidine during the first trimester of pregnancy developed major birth defects compared with the expected prevalence of one. The small size was too small to draw firm conclusions, however. With nizatidine there is only a single case report of a woman delivering a healthy baby after taking the drug during 14–16 weeks of gestation [217]. Although few reports are available, famotidine appears safe during pregnancy. Although nizatidine was previously classified as category C, the FDA recently reclassified it as a category B drug. However, the conflicting animal data are troublesome and suggest that other H2RAs may be safer during pregnancy. Proton pump inhibitors are the most effective drug therapy for symptom control and healing of esophagitis. The PPIs have not been as extensively used in pregnancy as the H2RAs, or is their efficacy proven in pregnancy, and the data about total safety are more limited. Omeprazole is categorized as a class C drug by the FDA because of fetal toxicity. The other PPIs are categorized as class B drugs. However, unlike the nonpregnant heartburn patient, PPIs should only be used during pregnancy in women with well-defined complicated GERD, not responding to lifestyle changes, antacids, and H2RAs.
Proton Pump Inhibitors (PPIs)
Omeprazole. Omeprazole, the first of the PPIs, is classified as a class C drug in pregnancy because at doses similar to those used in humans, omeprazole produced dose-related embryonic and fetal mortality in pregnant rats and rabbits [223]. No teratogenicity was observed. The FDA has received reports of at least 12 birth defects in pregnant women exposed to omeprazole, including anencephaly and hydroencephaly [217]. However, other case reports and small case series have found no infant congenital malformations in mothers taking 20–60 mg omeprazole/day, even in the first trimester of pregnancy [79, 224]. A meta-analysis from 2002 assessed the risks of congenital fetal malformations in women using PPIs in the first trimester of pregnancy [225]. Five studies met the inclusion criteria, all were cohort studies ascertaining pregnancy outcomes with either registry linkage [92, 218, 226] or by direct interview with the mother [225, 227]. A total of 593 infants were exposed to PPIs, most (534) received omeprazole. The summary relative risk for all major malformations among any PPI exposure was 1.18, a nonsignificant relative risk. For the four studies where data for only omeprazole could be extracted (Fig. 4.3), the summary relative risk was 1.05, also indicating a nonsignificant relative risk for malformations. Although the weight of evidence suggests omeprazole is safe in pregnancy, the FDA has not changed its class C rating. With the advent of newer PPIs, especially esomeprazole, omeprazole is currently infrequently prescribed. However, the drug is now over the counter at a 20 mg dose and cheaper than prescription PPIs.
Lansoprazole. Animal studies using doses of lansoprazole up to 40 times the recommended human dose have found no evidence of impaired fertility or fetal toxicity [229].
Human data on the safety of lansoprazole in pregnancy are more limited. In one nonobservational cohort study [224], six pregnant patients taking lansoprazole during the first trimester delivered seven healthy newborns. Lansoprazole was the only acid-suppressing drug exposed in 13 infants reported to the Swedish Medical Birth Registry [218]. Two birth defects were observed: one atrial septal defect and one undescended testes. In a Danish study published in 1999, 38 patients had taken PPIs during the first trimester of pregnancy (35 omeprazole, 3 lansoprazole) [226]. The prevalence of major birth defects, low birth weight, and prematurity were no different than in pregnant controls not receiving any medications. In a study published this year, 295 pregnancies exposed to omeprazole, 62 to lansoprazole, and 53 to pantoprazole were compared with 868 pregnant controls for the development of congenital abnormalities [230]. As with other studies, the rate of congenital abnormalities did not differ between the exposed and control groups: omeprazole 3.6 %, lansoprazole 3.9 %, and pantoprazole 2.1 % versus controls 3.8 %. No differences were found when exposure was limited to the first trimester. The lack of teratogenicity in animals is reassuring, accounting for the FDA class C risk category for lansoprazole use during pregnancy. However, the data on safety in human pregnancies are limited, and avoidance of this PPI and all PPIs, especially during the first trimester, is the safest course. If lansoprazole is required or if inadvertent exposure occurs early in gestation, the fetal risk seems to be low. Based on product information from the individual manufacturers, the newer PPIs (rabeprazole, pantoprazole, and esomeprazole) have been shown safe in various animal studies. No reports describing the use of these newer PPIs during human pregnancies are available [217].
Gastric Acid Suppression During Lactation
All systemic antireflux medications are excreted in breast milk and could harm the infant. Therapeutic options must be explained and discussed with women who require treatment but who want to breast-feed. Drug safety during lactation has been assessed in animal studies and human case reports (Table 4.4).
Table 4.4
Safety of antiulcer/GERD medications during lactation
|
Medications |
Safety |
Comments |
|
Antacids |
Yes |
Not concentrated in breast milk |
|
Sucralfate |
Yes |
Minimal, if any, excretion in breast milk |
|
Cimetidine |
Yes |
Compatible with breastfeeding (American Academy of Pediatrics) |
|
Ranitidine |
Yes |
Excreted in breast milk in concentrations similar to cimetidine |
|
Famotidine |
Yes |
Lowest concentrations in breast milk of all H2RAs |
|
Nizatidine |
No |
Growth depression in pups of lactating rats |
|
PPIs |
No |
Growth depression in pups of lactating rats |
GERD gastroesophageal reflux disease, H2 RA histamine2 receptor antagonist, PPI proton pump inhibitor
Antacids
Aluminum and magnesium hydroxide antacids are not concentrated in breast milk and, thus, are safe during lactation. Neither Gaviscon nor sucralfate has been studied during lactation but is presumed safe because of limited maternal absorption.
Histamine2 Receptor Antagonists
All H2RAs are excreted in human breast milk. Cimetidine and ranitidine reach concentrations in breast milk 4–7 times the doses present in maternal serum [231]. In contrast, famotidine only reaches a mean milk to plasma concentration of 1.78, 6 h after ingestions [232]. Small amounts of nizatidine are excreted into human breast milk [233]. In the only animal studies assessing H2RA safety during lactation, pups reared by lactating rats ingesting nizatidine experienced growth retardation [234]. The effects of H2RAs in breast milk on the nursing human infant are unknown. In 1994, the American Academy of Pediatricsclassified cimetidine as compatible with breastfeeding [235]. Others also suggest that ranitidine and famotidine are safe and the latter H2RA may be preferred because of the lower concentration in human breast milk. Nizatidine should be avoided in the breastfeeding mother because of the single animal study [234].
Proton Pump Inhibitors
Little is known about PPI excretion in breast milk or infant safety in lactating women. PPIs probably are excreted in human milk, because of their relatively low molecular weight. This was confirmed in the only report of PPI use during breastfeeding [236]. During the day, the patient fed her infant son just before taking omeprazole at 8:00 am, refraining from nursing for 4 h, and then expressed and discarded her breast milk at noon. At 3 weeks postpartum, blood and milk samples were obtained at 8:00 am and then every 30 min for 4 h. Breast milk levels of omeprazole began to rise at 9:30 am and peaked at 11:00 am at 58 mm, considerably lower value than simultaneous maternal level of 950 mm. The infant was doing well at 1 year. However, rats administered with omeprazole at 35–345 times and rabeprazole at a dose of 195 times the recommended human dose during late pregnancy and lactation had decreased body weight gain of their pups [223]. Therefore, PPIs are not recommended for use by lactating mothers. Women can either take PPIs and discontinue nursing or use medications (i.e., H2RA) from another class.
4.1.2.6 Prognosis
The diagnosis is often made late in pregnancy with quite devastating consequences. In the series of 24 cases described up to 1966, 16 patients were treated medically with 16 maternal (maternal mortality 100 %) and 11 infant deaths (fetal mortality of 69 %), while 8 patients received surgical treatment (seven simple closures and one partial gastrectomy) without maternal and two infant deaths (of the two infants who died, one was a twin; the other twin survived), making fetal mortality 29 % [19, 29, 55, 154, 178, 186–193]. It is questionable how Paul et al. in 1976 found only six (including their case) cases of maternal survival following perforation of a peptic ulcer and, of these, only four [237] (including their case) were associated with survival of both the mother (maternal mortality 33 %) and infant [238]. Early surgical diagnosis and treatment followed by vaginal delivery of the fetus offer the best hope for survival of the mother and child.
Table 4.2 shows ten cases during pregnancy (without puerperium) with maternal data of eight mothers. All survived and the survival rate today is approaching 100 %. Table 4.3 shows 12 cases of PPU during puerperium, but the data about maternal and fetal outcome are lacking; therefore, conclusions about prognosis cannot be made but probably are the same as during pregnancy. Clinicians are not reluctant to indicate necessary imaging methods during puerperium as in general population because there is no fear of radiation exposure to the fetus.
4.2 Perforated Malignant Ulcer/Carcinoma
Perforated gastric carcinoma is an extremely rare condition due to the rarity of the gastric cancer in pregnant population. The characteristics of gastric cancer in young (pregnant) women are discussed for easier understanding and diagnosis of such condition during pregnancy.
4.2.1 Gastric Cancer in Pregnancy
4.2.1.1 Incidence
Whereas gastric cancer is prevalent in the elderly, the incidence of gastric cancer associated with pregnancy is comparatively low, 0.026–0.1 % of all pregnancies [239–242]. There are few reports of pregnancy-associated gastric cancer from countries other than Japan. It was first reported by Fujimura and Fukunda in 1916 [243]. Jaspers et al. reviewed a total of 31 cases of pregnancy-associated gastric cancer in reports that were published in academic journals from 1969 to 1999 [244]. Theirs was the only major study in Western countries, and subsequent reports have been sporadic [245–252]. On the other hand, owing in part to the relatively high incidence of gastric cancer in Japan, more than 100 cases have been reported in this country up to 1987 [240]. The largest study from Japan accumulated 137 patients adding to Ueo et al. [240] another 37 cases of pregnancy-associated gastric cancer that had been newly reported in Japan from 1988 to 2007: these consisted of two cases in 1968–1977, six cases in 1978–1987, and 29 cases in 1987–2007 [253–271].
Krukenberg (Metastatic) Tumor
The association of Krukenberg tumor and pregnancy is extremely rare. For over a century and its first description in 1896 by Krukenberg [272], few cases have been reported in world literature [273]. Yaushiji on a series of 112 Krukenberg tumor reported only three cases during pregnancy, so an incidence of 2.6 % [274]. The rarity of this disease is due to the rarity of gastric cancer in young women. Only 0.4–0.5 % of gastric cancers occurs in women aged less than 30 years [275]. Incidence in future decades cannot be estimated. On one hand, with increasing fertility of women over 30 years, one could expect an increased incidence of this disease over the next decades, but on the other, the incidence of (advanced) gastric cancer is declining.
4.2.1.2 Pathology
Pathology according to the largest review on the topic shows that diffuse type is more common (86.9 %) than the intestinal type (13.1 %) [276]. While in older patients the majority of carcinomas are of the intestinal, usually well-differentiated type, the tumors in young patients are mainly poorly differentiated carcinomas of the diffuse type with signet ring cells and peritoneal metastasis.
4.2.1.3 Pathophysiology
Gastric adenocarcinoma occurs infrequently in patients under 40 years of age. The literature on gastric cancer in the young adults has described almost similar findings: the female dominance with a male to female ratio of 1:1.5 [277], more aggressive histological features, the advanced disease stage at presentation, and the poorer prognosis [278]. These characteristics were even more pronounced in the pregnancy-associated cases [242, 279]. Being more common in females, the association of gastric cancer and pregnancy could be purely a natural coincidence, but on the other hand, it has been postulated that the immunosuppression during pregnancy is conducive for tumor growth and the biological and hormonal circumstances further enhances tumor progression [279, 280]. Furukawa et al. demonstrated experimentally a suppressive effect of sex hormones on spreading of stomach cancer in rat models [280]. Placenta secretes histaminase which degrades histamine function; hence, the patient shows no deterioration of symptoms caused by the cancerous ulcer. As it is known, blood circulation increases during pregnancy; pregnant women are particularly susceptible to the rapid growth and spread of cancer.
4.2.1.4 Clinical Presentation
Krukenberg Tumor
A maternal and fetal virilization can be observed [281]. This virilization, nonspecific to Krukenberg, is due to luteinized ovarian stroma reaction, stimulated by the placental production of steroids and human chorionic gonadotropin. The pelvic mass was found in 49.3 % of cases in the series of Yaushiji [274]. Its management during pregnancy is difficult. Indeed, the incidence of malignant tumors is only about 1–6 % of adnexal masses associated with the pregnancy. The differential diagnosis with luteomas or other benign adnexal pathology, where the management is radically different, is not always easy.
4.2.1.5 Diagnosis
Hormonal and immunosuppressive effects of pregnancy could explain why most cases of gastric cancer associated with pregnancy are usually advanced by the time that they are diagnosed. Misdiagnosis is another contributing factor as the symptoms are frequently masked by factors related to the normal pregnancy. In one case initial symptoms of gastritis were mingled and masked by the hyperemesis gravidarum. Even on admission, the acute abdomen was thought to be pregnancy related. Similar to other reported cases, symptoms were attributed to the pregnancy and not evaluated further until delivery or complications developed [242, 279]. Detection can be further delayed as therapeutic approaches will usually be restricted by the physical and psychological clinical events surrounding the pregnancy.
Diagnostic modality for definitive diagnosis as in nonpregnant patients is esophagogastroduodenoscopy (EGD). Indications for the repeated EGD are the same as in nonpregnant patients. It is confirmed by the fact that a patient with an exacerbation of peptic ulcer presented with gastric carcinoma during pregnancy [282].
In pregnant patient MRI is preferred to CT scan due to the ionizing radiation. Although not specific, the presence of solid components showing hypo-intensity on T2-weighted images in an ovarian mass appears to be a characteristic finding of Krukenberg tumors (Figs. 4.3 and 4.4), especially if the tumors are bilateral, have sharp margin, thin-walled, and have an oval configuration [283, 284]. Except primary tumor, the metastatic form can be found, which can sometimes, as when Krukenberg tumor is present, mislead the clinician to the diagnosis of primary ovarian tumor during pregnancy. Therefore, the definitive diagnosis is histological, marked by areas of mucoid degeneration and by the presence of signet ring cells.
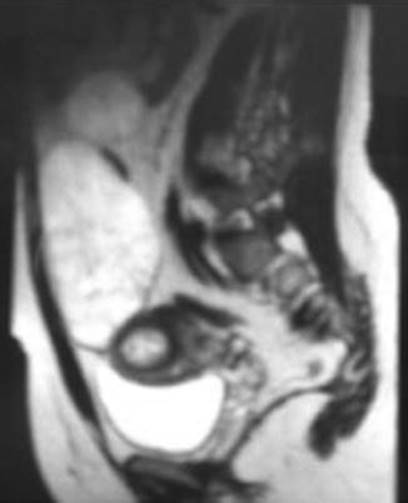
Fig. 4.3
Sagittal T2-weighted MR image revealing a gravid uterus with two ovarian masses [228]

Fig. 4.4
Axial T2-weighted MR image revealing bilateral Krukenberg tumors. Both are well encapsulated and have oval form [228]
4.2.1.6 Treatment
Primary Gastric Tumor
Because of this as well as the fact that the peritoneal cavity will already be contaminated by cancer cells, surgery should be as palliative as possible. In view of the poor outcome, a simple closure of the perforation or omentopexy is the usual procedure.
Metastatic Tumor
Indication for the palliative or curative surgery is the same as in general population. Concerning Krukenberg tumor, aggressive surgery can improve the prognosis; but its management depends essentially on the finding at laparotomy [285–287]. If no other metastatic disease except involvement of both ovaries is found (Fig. 4.5), bilateral oophorectomy with or without hysterectomy can be performed. The decision on the termination of pregnancy depends on the trimester of pregnancy and patient’s decision about current pregnancy. If the diagnosis of primary gastric carcinoma is known before the operation, definitive operation can be done in the same act. If primary tumor is not known, the diagnostic workup should be done and the indications for the operation made according the stage of the primary gastric carcinoma.

Fig. 4.5
Bilateral Krukenberg tumor at 10-week pregnancy without other metastatic disease found at laparotomy [228]
Cesarean Section
With regard to the fetus, an induced delivery or early Cesarean section will simplify management of the mother provided the fetus has reached viability. Otherwise an abortion is not known to be therapeutic, and an early pregnancy can be left undisturbed unless irradiation or chemotherapy is planned.
Hormonal Therapy
The effect of estrogen and the results of antiestrogen treatment in clinical trials are controversial. Jaspers et al. [244] reported that the features and prognosis in gastric cancer associated with pregnancy were the same as in other young patients.
4.2.1.7 Prognosis
Pregnancy-associated gastric cancer is found in the advanced stage in 95.5 % of the patients. In one of the largest studies by Ueo et al., only 44 % of the patients underwent surgical resection and the prognosis was extremely poor, i.e., 1-year survival in 14.5 % and 2-year survival in 10.6 % [240]. In another study patient survival was analyzed based on the data obtained from the 85 patients whose prognostic data were available. The prognosis was very poor: the 1- and 2-year survival rates were 18 and 15 %, respectively, and only five patients survived for more than 3 years with no recurrence [276]. Fazeny and Marosi conducted a 30-year review of the world’s medical literature. Among 100 reports of pregnancy-associated gastric cancer, only one survivor was detected. Maternal survival of 9–19 months after diagnosis in pregnancy was observed for all other cases [288]. Even in regard to the 27 patients diagnosed in the most recent 20 years, the 1- and 2-year survival rates were 37 and 32 %, respectively [276]. In conclusion, the prognosis of patients with pregnancy-associated gastric cancer remains poor, although it seems to be somewhat improved compared with that in the report of Ueo et al. [240].
4.2.2 Perforated Gastric Cancer in Pregnancy
4.2.2.1 Incidence
There are four cases of perforated gastric cancer during pregnancy published with extremely poor prognosis. First is a 29-year-old woman from Turkey [289] and three others from Japan, one during Cesarean section [261], another during pregnancy during observation of ovarian tumor [254], and the third during delivery with misdiagnosed abruption of placenta [271]. There is only one case of perforated malignant ulcer in 43-year-old 17th gravid patient, who developed a perforation of a carcinomatous ulcer of the stomach on the 8th day of puerperium [290]. There are no more details about the case.
4.2.2.2 Treatment
Primary Gastric Tumor
The difference between benign and malignant ulcer or carcinoma is the necessity of oncologic curative or palliative surgery. If perforated carcinoma is found during Cesarean section, definitive oncologic surgery could be made or just suturing as the therapy for the perforation and another exploration is made for definitive surgery. If perforation is found during pregnancy, further therapy depends on the stage of pregnancy as in other malignant tumors during pregnancy. In early pregnancy termination of pregnancy with oncologic surgery is made. In advanced pregnancy oncologic surgery can be postponed after delivery, or if pregnancy is around 27th week, then corticosteroids are used for fetal lung maturation and Cesarean section with definitive surgery is made.
Because of this as well as the fact that the peritoneal cavity will already be contaminated by cancer cells, surgery should be as palliative as possible. In view of the poor outcome, a simple closure of the perforation or omentopexy is the usual procedure.
4.2.2.3 Prognosis
One patient died 6 months after initial diagnosis of gastric cancer despite surgical therapy and adjuvant chemotherapy [289]. Unfortunately, the data for three Japanese cases [254, 261, 271], as well as for perforated malignant ulcer [290], were not available.
4.3 Non-peptic Ulcer Nontraumatic Gastric Perforations/Ruptures
4.3.1 Spontaneous Gastric Rupture
4.3.1.1 History and Incidence
Spontaneous rupture of the stomach in general population was the subject of medical speculation as long ago as 1819, but Carson’s report in 1845 offered the first proof of its occurrence in human [291]. Glassman in 1929 collected 14 cases of nontraumatic rupture of the stomach from the literature and noted that there was but one survival [292]. Miller has made the first report of spontaneous rupture of the stomach during labor or the postpartum period [293]. It is an extremely rare condition with less than ten cases published [44, 199, 293–296].
4.3.1.2 Etiopathogenesis
Spontaneous gastric rupture is rare because the stomach is anatomically protected in the upper abdomen by the liver and ribs and because the stomach has mobile distensible walls and two valves, gastroesophageal and pyloric, to decrease intragastric pressure [297].
It is apparent from the reports of spontaneous rupture of the stomach or intestine that distention of the viscera invariably precedes rupture. Acute gastric dilatation is a recognized complication of the postpartum period which is most frequently of functional origin. Pylorospasm, “dropping” of the stomach and intestines to their antepartum position, hypotonicity of the bowel, and “nutritional edema” of the pylorus have also been suggested as etiological factors in acute postpartum gastric dilatation [298]. Harkins has noted that gastric dilatation and intestinal ileus are prone to occur after abdominal operations and especially when peritonitis is present [299]. Carlson and Ortiz in 1960 attributed ileus and gastric dilatation to the exhaustion phase of the stress reaction and have treated their patients with ACTH [300]. Whatever the cause of the dilatation, sustained distention of the stomach may lead to an ischemic necrosis of the mucosa with disruption of this layer and subsequent extension through the remainder of the stomach wall [293, 301]. Nontraumatic rupture of the dilated stomach occurs most frequently near the lesser curvature and explains this predilection by the external fixation of the lesser curvature and the reduced “elastic coefficient” of the “magenstrasse” [301, 302]. These authors describe a symptomatic triad of:
· Tympanitic distention of the abdomen
· Subcutaneous emphysema
· Shock as distinguishing features of spontaneous rupture of the stomach
The first factor leading to increased intragastric pressure is dilatation of its walls following sudden consumption of large quantities of food. Historical studies on cadavers by Revilliod in 1885 indicate that the stomach has enormous capacity. Gastric rupture due to overfilling could occur only after a rapid filling of a stomach with 4 l of fluid and that the rents occurred in mid-stomach, both anterior and posterior walls [303]. Key Aberg in 1897 made the experiment in sitting position and found that filling with 4 l made ruptures on the lesser curvature.
Vomiting is a significant contributing factor in Mallory-Weiss syndrome, causing longitudinal cracks in the gastric mucosa near the cardia. The above-mentioned cracks may penetrate into the muscular layer. Sometimes vomiting may lead to the rupture of the distal esophagus (Boerhaave syndrome). The difference is that the esophageal rupture occurs during vomiting with gastric contents, while gastric rupture occurs during nausea and vomiting reflexes. Pathogenesis of gastric rupture is believed to involve arterial ischemia of the gastric wall despite its excellent blood supply. Inflammation of the gastric mucosa which often is not noticed by the patients is also a significant factor here. Trauma, e.g., indirect cardiac massage or chest thump, is the last of the factors leading to gastric rupture [304].
High position of the diaphragm intensified activity of the valve closing the gastric cardia. Compression of the stomach by the uterine fundus increased intragastric pressure and impaired gastric emptying. The probable inflammation of the gastric mucosa decreased the resistance of its walls.
Spontaneous gastric rupture can be caused by increased intra-abdominal pressure [305]. The pathologically dilated stomach becomes susceptible to rupture during forceful emesis when an abrupt increase in intra-abdominal pressure occurs [306]. Once the stomach becomes critically dilated, the lower esophageal sphincter functionally becomes a one-way valve, allowing contents to only enter into the stomach. Such gastric ruptures typically occur on the lesser curvature where the stomach is less elastic.
All authors have been impressed by the rapidity of onset and depth of the shock and note that these patients die in the first 9–10 h without alleviation of the state of shock by vigorous, supportive treatment. Numerous explanations of the mechanism of this type of shock have been advanced, all pertinent, but none of which are conclusive. Christoph and Pinkhamew in 1961 believed that the pathogenesis of the gastric rupture in the presented case followed a definite sequence [294]. Because of the stress from perforation of the appendix and peritonitis, which may have spread following involution of the uterus, and spontaneous delivery, the basis for acute gastric dilatation was present [299, 300]. The distention was sufficient to cause ischemic necrosis of the gastric mucosa [293, 301] with a subsequent tearing of the outer layers of the stomach wall by the trauma of persistent emesis. Because of the surgical vent in the right lower quadrant, this case did not demonstrate the tympany and subcutaneous emphysema described by others [301]. The depth of shock, however, was disheartening to physician and surgeon alike. In view of the facts that postpartum gastric dilatation and postoperative abdominal distention are frequent complications without causing “unexpected rupture” of a viscus, an additional factor must have had a vital role in the present case. Christoph and Pinkhamew in 1961 believed that stress and chemical imbalance from her several difficulties may have produced changes in the gastric mucosa similar to those produced in major burns [294]. It seems probable that the subtly damaged gastric wall was thus more susceptible to ischemic necrosis and subsequent rupture than the normal stomach.
Some authors believe that the term “spontaneous rupture” of the stomach is a misnomer and that “unexpected rupture” is a more descriptive phrase [294, 307]. In reviewing the available reports of so-called spontaneous rupture of the stomach, a pathologic basis, whether it was ulcer, carcinoma, or gastric dilatation of undetermined cause, was demonstrated at operation or at postmortem examination in all cases.
It should be noted that both cases of gastric rupture in pregnancy were located on the greater curvature [293, 295].
4.3.1.3 Prognosis
In general population during 1930s, in a small number of patients with nontraumatic gastric rupture the survival was almost impossible (1 of 14 patients) [292]. Previous literature indicates high maternal and newborn mortality [44, 199, 304]. There is one case with maternal survival but fetal death in 2002 [296]. The key for maternal survival was early suspicion and diagnosis, early aggressive resuscitation, and emergency laparotomy.
4.3.2 Postoperative Gastric Perforation/Rupture
4.3.2.1 Gastric Ulcer Perforation After Gastric Banding
Laparoscopic placing of an inflating silicon band around the stomach and reducing its orifice, also known as gastric banding, is a surgical procedure that reduces maternal obesity. This procedure is associated with increased unplanned pregnancies. The most common effect reported during pregnancy is repeated/intractable nausea and vomiting, resolving with deflating of the silicon band. This complication imposes a diagnostic dilemma as to whether bowel obstruction or other intra-abdominal pathologies are involved.
Marginal ulcer is a known complication of bariatric surgery and is a result of tissue ischemia caused by reduced blood supply to the stomach because of the inflated ring [308]. Therefore, when the patient deteriorates under conservative management and a laparotomy is performed, removal of the ring is necessary to resume appropriate gastric blood supply, which is important for a proper gastric healing. Weiss et al. reviewed the results of seven pregnancies, five of which had progressed to delivery [309]. All bands were decompressed because of nausea and vomiting, and two patients had serious complications: one had intragastric migration of the band and the other a balloon defect. Both had to be operated on to remove the band. Laparoscopic gastric banding is considered an efficient and relatively safe procedure for the treatment of maternal obesity. The severely obese pregnant patients with previous gastrointestinal surgery demonstrate one of the unique management dilemmas when presenting with intractable vomiting. This case is even more complicated because a combination of other clinical symptoms suggesting preeclampsia and fetal distress, on top of obesity and vomiting, made the diagnosis even more difficult [198].
4.3.2.2 Gastric Rupture Caused by Diaphragmatic Hernia
This entity is described in Chap. 6.
References
1.
Wu Z. Study of the ancient corpse of the Western Han dynasty unearthed from tomb no. 168 on Phoenix Hill at Jiangling County. Med Bull Wuhan Med Coll. 1980;1:1–12.
2.
Baron JH. Peptic ulcer. Mount Sinai J Med. 2000;67:58–62.
3.
Valle JD, Chey WD, Scheiman JM. Acid peptic disorders. In: Yamada T, editor. Textbook of gastroenterology. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2003. p. 1322–76.
4.
Kurata JH, Honda GD, Frankl H. The incidence of duodenal and gastric ulcers in a large health maintenance organization. Am J Public Health. 1985;75:625–9.PubMed
5.
Rosenstock SJ, Jorgensen T. Prevalence and incidence of peptic ulcer disease in a Danish County – a prospective cohort study. Gut. 1995;36:819–24.PubMed
6.
Ostensen H, Gudmundsen TE, Bolz KD, et al. The incidence of gastric ulcer and duodenal ulcer in north Norway. A prospective epidemiological study. Scand J Gastroenterol. 1985;20:189–92.PubMed
7.
Bonnevie O. The incidence in Copenhagen County of gastric and duodenal ulcers in the same patient. Scand J Gastroenterol. 1975;10:529–36.PubMed
8.
Wu HC, Tuo BG, Wu WM, et al. Prevalence of peptic ulcer in dyspeptic patients and the influence of age, sex, and Helicobacter pylori infection. Dig Dis Sci. 2008;53:2650–6.PubMed
9.
Wang YR, Richter JE, Dempsey DT. Trends and outcomes of hospitalizations for peptic ulcer disease in the United States, 1993 to 2006. Ann Surg. 2010;251:51–8.PubMed
10.
Paimela H, Paimela L, Myllykangas-Luosujarvi R, et al. Current features of peptic ulcer disease in Finland: incidence of surgery, hospital admissions and mortality for the disease during the past twenty-five years. Scand J Gastroenterol. 2002;37:399–403.PubMed
11.
Groenen MJ, Kuipers EJ, Hansen BE, et al. Incidence of duodenal ulcers and gastric ulcers in a Western population: back to where it started. Can J Gastroenterol. 2009;23:604–8.PubMed
12.
Ahsberg K, Ye W, Lu Y, et al. Hospitalisation of and mortality from bleeding peptic ulcer in Sweden: a nationwide time-trend analysis. Aliment Pharmacol Ther. 2011;33:578–84.PubMed
13.
Kubícková Z, Veselý KT. Fertility and reproduction in patients with duodenal ulcer. J Reprod Fertil. 1974;36:311–7.PubMed
14.
Cappell MS, Sidhom O. A multicenter, multiyear study of the safety and clinical utility of esophagogastroduodenoscopy in 20 consecutive pregnant females with follow-up of fetal outcome. Am J Gastroenterol. 1993;88:1900–5.PubMed
15.
Cappell MS. Gastrointestinal endoscopy in high-risk patients. Dig Dis. 1996;14:228–44.PubMed
16.
Krueger KJ, Hoffman BJ. Radiation exposure during gastroenterologic fluoroscopy: risk assessment for pregnant workers. Am J Gastroenterol. 1992;87:429–31.PubMed
17.
Baird RM. Peptic ulceration in pregnancy: report of a case with perforation. Can Med Assoc J. 1966;94:861–2.PubMed
18.
Great Britain. General Register Office: statistical review for England and Wales. Part III, Commentary. Table; deaths of women not classed to pregnancy or childbearing but certified as associated therewith, England and Wales. London: Her Majesty’s Stationery Office; 1951–1960.
19.
Great Britain. General Register Office: Statistical review of England and Wales, for the year 1961. Part I, table 17. London: Her Majesty’s Stationery Office; 1963. p. 122.
20.
Vasicka A, Lin TJ, Bright RH. Peptic ulcer in pregnancy; review of hormonal relationships and a report of one case of massive gastrointestinal hemorrhage. Obstet Gynecol Surv. 1957;12:1–13.PubMed
21.
Rachlin B. Duodenal ulcer in early pregnancy; report of two cases. Obstet Gynecol. 1957;10:684–6.PubMed
22.
Heading RC. Prevalence of upper gastrointestinal symptoms in the general population: a systematic review. Scand J Gastroenterol Suppl. 1999;231:3–8.PubMed
23.
Camilleri M, Dubois D, Coulie B, et al. Prevalence and socioeconomic impact of functional gastroenterological disorders in the United States: results from the US Upper Gastrointestinal Study. Clin Gastroenterol Hepatol. 2005;3:543–52.PubMed
24.
Nagler R, Spiro HM. Heartburn in late pregnancy: manometric studies of esophageal motor function. J Clin Invest. 1961;40:954–70.PubMed
25.
Olans LB, Wolf JL. Gastroesophageal reflux in pregnancy. Gastrointest Endosc Clin North Am. 1975;82:699–703.
26.
Sandweiss DJ, Saltzstein HC, Farbman AA. The relation of sex hormones to peptic ulcer. Am J Diges Dis. 1939;6:6–12.
27.
Clark DH. Peptic ulcer in women. Br Med J. 1953;1:1254–7.PubMed
28.
Hurst AF, Stewart MJ. Gastric and duodenal ulcer. Oxford: Oxford University Press; 1929. p. 153.
29.
James DW. Peptic ulcer during pregnancy with a report of a case of perforation. Br Med J. 1948;2:74–5.PubMed
30.
Mulsow FW, Brown WE. Am J Obstet Gynecol. 1936;31:1041.
31.
Balint R. Ulcusproblem und Säurebasengleichgewicht. Berlin: S. Karger; 1927.
32.
Nakai T. On the gastric juice of the pregnant women. Tokyo J Biochem. 1925;5:465-77.
33.
Strauss MB, Castle WB. Studies of anemia in pregnancy; gastric secretion in pregnancy and puerperium. Am J Med Sci. 1932;184:655–62.
34.
Bloomfiled AL, Keefer CS. Clinical physiology of the stomach: simultaneous quantitative observations on gastric secretory volume, acidity and motility. Arch Intern Med (Chicago). 1926;38:145–57.
35.
Clark DH, Tankel HI. Gastric acid and plasma-histaminase during pregnancy. Lancet. 1954;2:886–9.
36.
Artz F. Further observations on the gastric juice in pregnancy. Am J Obstet Gynecol. 1930;20:382–5.
37.
Labate JS. The effect of pregnancy on gastric secretion. Am J Obstet Gynecol. 1939;38:650–3.
38.
Murray FA, Erskine JP, Fielding J. Gastric secretion in pregnancy. J Obstet Gynec Br Emp. 1957;64:373–81.
39.
Barnes LW. Serum histaminase during pregnancy. Obstet Gynecol. 1957;9:730–2.PubMed
40.
Liepins KW, Ivy AC, Suzuki R. Effect of certain histaminase inhibitors on gastric secretion. Am J Physiol. 1958;195:209–15.PubMed
41.
Peter ET, Walder AI, Madsen AJ, Wangensteen OH. Production of gastric secretory inhibition by diamine oxidase (histaminase). Surg Forum. 1963;14:336–8.PubMed
42.
Way S. Relation between gastric acidity and the anterior-pituitary-like hormone content of urine in pregnant women. Br Med J. 1945;2:182–4.PubMed
43.
Abrahamson RH, Church R, Hinton JW. Hormone effects on gastroduodenal mucosa. Am J Med Sci. 1942;204:809–23.
44.
Laszlo F, Amani E, Varga CS, Laszlo FA. Influence of sex hormones on ethanol-induced gastric haemorrhagic erosions in rats. Acta Physiol Hung. 1992;80:289–92.
45.
Montoneri C, Drago F. Effects of pregnancy in rats on cysteamine-induced peptic ulcers: role of progesterone. Dig Dis Sci. 1997;42:2572–5.PubMed
46.
Truelove SC. Stilboestrol, phenobarbitone, and diet in chronic duodenal ulcer. A factorial therapeutic trial. Br Med J. 1960;2:559–66.PubMed
47.
Doll R, Hill ID, Hutton CF. Treatment of gastric ulcer with carbenoxolone sodium and oestrogens. Gut. 1965;6:19–24.PubMed
48.
Parbhoo SP, Johnston IDA. Effects ofoestrogens and progestogens on gastric secretion in patients with duodenal ulcer. Gut. 1966;7:612–8.PubMed
49.
Borri A. Ober magengeschwure im Klimakterium. Zbl Inn Med. 1904;25:689–96.
50.
Kahlson G, Lilja B, Svensson SE. Physiological protection against gastric ulceration during pregnancy and lactation in the rat. Lancet. 1964;2:1269–72.PubMed
51.
Izak G, Rachmilewitz M, Stein Y, et al. Vitamin B12 and iron deficiencies in anemia of pregnancy and puerperium. Arch Intern Med. 1957;99:346–55.
52.
Gryboski WA, Spiro HM. The effect of pregnancy on gastric secretion. New Engl J Med. 1956;255:1131–4.PubMed
53.
Ahimark A. Significance of blood histaminase in pregnancy. Lancet. 1944;2:406–7.
54.
Rostorfer HH, Laskowski M. Action of histaminase preparations in the heidenhain dog. Am J Dig Dis. 1945;12:337–9.
55.
Horwich M. Perforated duodenal ulcer during pregnancy. Br Med J. 1958;2:145.PubMed
56.
Gemzell CA. Blood levels of 17-hydroxysteroids in normal pregnancy. J Clin Endocrinol. 1953;13:898–902.PubMed
57.
Wu CY, Tseng JJ, Chou MM, et al. Correlation between Helicobacter pylori and gastrointestinal symptom in pregnancy. Adv Ther. 2000;17:152–8.PubMed
58.
Erdem A, Arslan M, Erdem M, et al. Detection of Helicobacter pylori seropositivity in hyperemesis gravidarum and correlation with symptoms. Am J Perinatol. 2002;19:87–92.PubMed
59.
McKenna D, Watson P, Dornan J. Helicobacter pylori infection and dyspepsia in pregnancy. Obstet Gynecol. 2003;102:845–9.PubMed
60.
Fukui O, Shimoya K, Shimizu TT, et al. Helicobacter pylori infection and platelet counts during pregnancy. Int J Gynecol Obstet. 2005;89:26–30.
61.
Vergara M, Catalán M, Gisbert JP, Calvet X. Meta-analysis: role of Helicobacter pylori eradication in the prevention of peptic ulcer in NSAID users. Aliment Pharmacol Ther. 2005;21:1411–8.PubMed
62.
Gulmez SE, Lassen AT, Aalykke C, et al. Spironolactone use and the risk of upper gastrointestinal bleeding: a population-based case-control study. Br J Clin Pharmacol. 2008;66:294–9.PubMed
63.
Lewis JD, Strom BL, Localio AR, et al. Moderate and high affinity serotonin reuptake inhibitors increase the risk of upper gastrointestinal toxicity. Pharmacoepidemiol Drug Saf. 2008;17:328–35.PubMed
64.
Aldoori WH, Giovannucci EL, Stampfer MJ, et al. A prospective study of alcohol, smoking, caffeine, and the risk of duodenal ulcer in men. Epidemiology. 1997;8:420–4.PubMed
65.
Sonnenberg A, Müller-Lissner SA, Vogel E, et al. Predictors of duodenal ulcer healing and relapse. Gastroenterology. 1981;81:1061–7.PubMed
66.
Koivisto TT, Voutilainen ME, Färkkilä MA. Effect of smoking on gastric histology in Helicobacter pylori-positive gastritis. Scand J Gastroenterol. 2008;43:1177–83.PubMed
67.
Schubert ML, Peura DA. Control of gastric acid secretion in health and disease. Gastroenterology. 2008;134:1842–60.PubMed
68.
Gocmen E, Koc M, Tez M, et al. Effect of Ramadan on surgical emergencies. Ann Emerg Med. 2004;44:283–5.PubMed
69.
Bener A, Derbala MF, Al-Kaabi S, et al. Frequency of peptic ulcer disease during and after Ramadan in a United Arab Emirates hospital. East Mediterr Health J. 2006;12:105–11.PubMed
70.
Torab FC, Amer M, Abu-Zidan FM, Branicki FJ. Perforated peptic ulcer: different ethnic, climatic and fasting risk factors for morbidity in Al-ain medical district, United Arab Emirates. Asian J Surg. 2009;32:95–101.PubMed
71.
Elnagib E, Mahadi S, Mohamed E, Ahmed M. Perforated peptic ulcer in Khartoum. Khartoum Med J. 2008;1:62–4.
72.
Donderici O, Temizhan A, Kucukbas T, Eskioglu E. Effect of Ramadan on peptic ulcer complications. Scand J Gastroenterol. 1994;29:603–6.PubMed
73.
Kucuk H, Censur Z, Kurt N, et al. The effect of Ramadan fasting on duodenal ulcer perforation: a retrospective analysis. Indian J Surg. 2005;67:195–8.
74.
Jastaniah S, Al Naami MY, Malatani TM. Perforated duodenal ulcer in Asir central hospital. Saudi J Gastroenterol. 1997;3:90–3.PubMed
75.
O’Mahony S. Endoscopy in pregnancy. Best Pract Res Clin Gastroenterol. 2007;21:893–9.PubMed
76.
Cappell MS. Risks versus benefits of gastrointestinal endoscopy during pregnancy. Nat Rev Gastroenterol Hepatol. 2011;8:610–34.PubMed
77.
ASGE Standard of Practice Committee, Shergill AK, Ben-Menachem T, Chandrasekhara V, et al. Guidelines for endoscopy in pregnant and lactating women. Gastrointest Endosc. 2012;76:18–24.PubMed
78.
Bánhidy F, Dakhlaoui A, Puhó EH, Czeizel AE. Peptic ulcer disease with related drug treatment in pregnant women and congenital abnormalities in their offspring. Congenit Anom (Kyoto). 2011;51:26–33.
79.
Brunner G, Meyer H, Athmann C. Omeprazole for peptic ulcer disease in pregnancy. Digestion. 1998;59:651–4.PubMed
80.
Acs N, Bánhidy F, Puhó EH, Czeizel AE. A possible association between maternal dyspepsia and congenital rectal/anal atresia/stenosis in their children: a population-based case-control study. Acta Obstet Gynecol Scand. 2009;88:1017–23.PubMed
81.
Chen YH, Lin HC, Lou HY. Increased risk of low birthweight, infants small for gestational age, and preterm delivery for women with peptic ulcer. Am J Obstet Gynecol. 2010;202:164.e1–8.
82.
Institute of Medicine. Subcommittee on nutritional status and weight gain during pregnancy. Nutrition during pregnancy. Washington, DC: National Academy Press; 1990.
83.
Knopp RH. Hormone-mediated changes in nutrient metabolism in pregnancy: a physiological basis for normal fetal development. Ann N Y Acad Sci. 1997;817:251–71.PubMed
84.
Caruso A, Paradisi G, Ferrazzani S, et al. Effect of maternal carbohydrate metabolism on fetal growth. Obstet Gynecol. 1998;92:8–12.PubMed
85.
Scholl TO, Sowers M, Chen X, Lenders C. Maternal glucose concentration influences fetal growth, gestation, and pregnancy complications. Am J Epidemiol. 2001;154:514–20.PubMed
86.
Choung RS, Talley NJ. Epidemiology and clinical presentation of stress-related peptic damage and chronic peptic ulcer. Curr Mol Med. 2008;8:253–7.PubMed
87.
Copper RL, Goldenberg RL, Das A, et al. The preterm prediction study: maternal stress is associated with spontaneous preterm birth at less than thirty-five weeks’ gestation. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Am J Obstet Gynecol. 1996;175:1286–92.PubMed
88.
Monk C, Fifer WP, Myers MM, et al. Maternal stress responses and anxiety during pregnancy: effects on fetal heart rate. Dev Psychobiol. 2000;36:67–77.PubMed
89.
Wadhwa PD, Sandman CA, Porto M, et al. The association between prenatal stress and infant birth weight and gestational age at birth: a prospective investigation. Am J Obstet Gynecol. 1993;169:858–65.PubMed
90.
Kallen B. Delivery outcome after the use of acid-suppressing drugs in early pregnancy with special reference to omeprazole. Br J Obstet Gynaecol. 1998;105:877–81.PubMed
91.
Magee LA, Inocencion G, Kamboj L, et al. Safety of first trimester exposure to histamine H2 blockers. A prospective cohort study. Dig Dis Sci. 1996;41:1145–9.PubMed
92.
Ruigomez A, Garcia Rodriguez LA, Cattaruzzi C, et al. Use of cimetidine, omeprazole, and ranitidine in pregnant women and pregnancy outcomes. Am J Epidemiol. 1999;150:476–81.PubMed
93.
Jensen RT, Gardner JD. Gastrinoma. In: Go VLW, DiMagno EP, Gardner JD, et al., editors. The pancreas: biology, pathobiology and disease. New York: Raven; 1993. p. 931–78.
94.
Ellison EH, Wilson SD. The Zollinger-Ellison syndrome: re-appraisal and evaluation of 260 registered cases. Ann Surg. 1964;160:512–30.PubMed
95.
Jensen RT, Norton JA. Endocrine tumors of the pancreas. In: Yamada T, Alpers BH, Owyang C, Powell DW, Silverstein FE, editors. Textbook of gastroenterology. 2nd ed. Philadelphia: Lippincott; 1995. p. 2131–66.
96.
Metz DC, Jensen RT. Advances in gastric antisecretory therapy in Zollinger-Ellison syndrome. In: Mignon M, Jensen RT, editors. Endocrine tumors of the pancreas: recent advances in research and management, Frontiers of gastrointestinal research, vol. 23. Basel: Karger; 1995. p. 240–57.
97.
Weber HC, Venzon DJ, Lin JT, et al. Determinants of metastatic rate and survival in patients with Zollinger-Ellison syndrome: a prospective long-term study. Gastroenterology. 1995;108:1637–49.PubMed
98.
Frick G, Bremme K, Sjogren C, et al. Plasma levels of cholecystokinin and gastrin during the menstrual cycle and pregnancy. Acta Obstet Gynecol Scand. 1990;69:317–20.PubMed
99.
Waddell WR, Leonsins AS, Zuidema GD. Gastric secretory and other laboratory studies on two patients with Zollinger–Ellison syndrome. New Eng J Med. 1959;260:56–62.PubMed
100.
Mentagen CN, Moeller MD, Klotz AP. Protection by pregnancy. Zollinger–Ellison syndrome. J Kans Med Soc. 1974;75:37–9.
101.
Ezeh UO, Narayan H. Pregnancy does not offer protection against Zollinger–Ellison syndrome. Acta Obstet Gynecol Scand. 1996;75:302–4.PubMed
102.
Mayer A, Sheiner E, Holcberg G. Zollinger Ellison syndrome, treated with lansoprazole, during pregnancy. Arch Gynecol Obstet. 2007;276:171–3.PubMed
103.
Stewart CA, Termanini B, Sutliff VE, et al. Management of the Zollinger-Ellison syndrome in pregnancy. Am J Obstet Gynecol. 1997;176(1 Pt 1):224–33.PubMed
104.
Jensen RT, Collen MJ, Allende HD, et al. Cimetidine induced impotence and breast changes in patients with gastric hypersecretory states. New Engl J Med. 1983;308:883–7.PubMed
105.
Parker S, Udani M, Gavaler JS, Van Thiel DH. Pre- and neonatal exposure to cimetidine but not ranitidine adversely affects adult sexual functioning of male rats. Neurobehav Toxicot Teratol. 1984;6:313–8.
106.
Baron TH, Richter JE. Gastroesophageal reflux disease in pregnancy. Gastroenterol Clin North Am. 1992;21:777–91.PubMed
107.
Armentano G, Bracco PL, DiSilverio C. Ranitidine in the treatment of reflux oesophagitis in pregnancy. Clin Exp Obstet Gynecol. 1996;16:130–3.
108.
Harper MA, McVeigh JE, Thompson W, et al. Successful pregnancy in association with Zollinger-Ellison syndrome. Am J Obstet Gynecol. 1995;173:863–4.PubMed
109.
Rossi G, Romagnoli S, Lauretti L, et al. Helicobacter pylori infection negatively influences pregnancy outcome in a mouse model. Helicobacter. 2004;9:152–7.PubMed
110.
Gøbel R, Symonds EL, Butler RN, Tran CD. Association between Helicobacter pylori infection in mothers and birth weight. Dig Dis Sci. 2007;52:3049–53.PubMed
111.
Yip R, Limburg PJ, Ahlquist DA, et al. Pervasive occult gastrointestinal bleeding in an Alaska native population with prevalent iron deficiency: role of Helicobacter pylori gastritis. J Am Med Assoc. 1997;277:1135–9.
112.
Peach HG, Bath NE, Farish SJ. Helicobacter pylori infection: an added stressor on iron status of women in the community. Med J Aust. 1998;169:188–90.PubMed
113.
Choe YH, Kwon YS, Jung MK, et al. Helicobacter pylori – associated iron deficiency anemia in adolescent female athletes. J Pediatr. 2001;139:100–4.PubMed
114.
Milman N, Rosenstock S, Andersen L, et al. Serum ferritin, hemoglobin, and Helicobacter pylori infection: a seroepidemiologic survey comprising 2794 Danish adults. Gastroenterology. 1998;115:268–74.PubMed
115.
Weyermann M, Rothenbacher D, Gayer L, et al. Role of Helicobacter pylori infection in iron deficiency during pregnancy. Am J Obstet Gynecol. 2005;192:548–53.PubMed
116.
Barabino A. Helicobacter pylori-related iron deficiency anemia: a review. Helicobacter. 2002;7:71–5.PubMed
117.
Singh V, Trikha B, Vaiphel K, et al. Helicobacter pylori: evidence for spouse-to-spouse transmission. J Gastroenterol Hepatol. 1999;14:519–22.PubMed
118.
Schutze K, Hentschel E, Dragosics B, et al. Helicobacter pylori reinfection with identical organisms: transmission by the parents’ spouses. Gut. 1995;36:831–3.PubMed
119.
Bamford KB, Bickley J, Collins JSA, et al. Helicobacter pylori: comparison of DNA fingerprints provides evidence for intrafamilial infection. Gut. 1993;34:1348–50.PubMed
120.
Bolin TD, Korman MG, Hansky J, Stanton R. Heartburn: community perceptions. J Gastroenterol Hepatol. 2000;15:1–2.
121.
Agréus L, Eslick GD, Engstrand L, et al. Is Helicobacter pylori infection associated with nausea? J Gastroenterol Hepatol. 1997;12(Suppl):A81.
122.
Kocak I, Akcan Y, Ustun C, et al. Helicobacter pylori seropositivity in patients with hyperemesis gravidarum. Int J Gynaecol Obstet. 1999;66:251–4.PubMed
123.
Jacoby EB, Porter KB. Helicobacter pylori infection and persistent hyperemesis gravidarum. Am J Perinatol. 1999;16:85–8.PubMed
124.
Gurski MR, Gonzalez E, Brown EG. Immunochemical localization of platelet-derived growth factor in placenta and its possible role in pre-eclampsia. J Invest Med. 1999;47:128–33.
125.
Murray L, Bamford K, O’Reilly PJ, et al. Helicobacter pylori infection: relation with cardiovascular risk factors, ischaemic heart disease, and social class. Br Heart J. 1995;74:497–501.PubMed
126.
Mendall MA, Goggin PM, Strachan D, et al. Relation of Helicobacter pylori infection and coronary heart disease. Br Heart J. 1994;71:437–9.PubMed
127.
Miragliotta G, Del-Prete R, Mosca A. Helicobacter pylori infection and coronary heart disease. Lancet. 1994;344:751.PubMed
128.
Patel P, Mendall MA, Carrington D, et al. Fibrinogen: a link between chronic infection and coronary heart disease. Lancet. 1994;343:1634–5.PubMed
129.
Segal ED, Cha J, Lo J, et al. Altered states: involvement of phosphorylated CagA in the induction of host cellular growth changes by Helicobacter pylori. Proc Natl Acad Sci U S A. 1999;96:14559–64.PubMed
130.
Guiraldes E, Duarte I, Pena A, et al. Proinflammatory cytokine expression in gastric tissue from children with Helicobacter pylori-associated gastritis. J Pediatr Gastroenterol Nutr. 2001;33:127–32.PubMed
131.
Heimonen A, Janket SJ, Meurman JH, et al. Oral health care patterns and the history of miscarriage. Oral Dis. 2008;14:734–40.PubMed
132.
Collodel G, Moretti E, Campagna MS, et al. Infection by CagA-positive Helicobacter pylori strains may contribute to alter the sperm quality of men with fertility disorders and increase the systemic levels of TNF-alpha. Dig Dis Sci. 2010;55:94–100.PubMed
133.
Yamaoka Y, Kodama T, Gutierrez O, et al. Relationship between Helicobacter pylori iceA, cagA, and vacA status and clinical outcome: studies in four different countries. J Clin Microbiol. 1999;37:2274–9.PubMed
134.
Graham DY, Yamaoka Y. H. pylori and cagA: relationships with gastric cancer, duodenal ulcer, and reflux esophagitis and its complications. Helicobacter. 1998;3:145–51.PubMed
135.
Hajishafiha M, Ghasemi-Rad M, Memari A, et al. Effect of Helicobacter pylori infection on pregnancy rates and early pregnancy loss after intracytoplasmic sperm injection. Int J Womens Health. 2011;3:329–35.PubMed
136.
Goh JT, Flynn MB, Florin TH. Active chronic peptic ulcer disease complicated by gastric outlet obstruction in pregnancy. Aust N Z J Obstet Gynaecol. 1993;33:89–90.PubMed
137.
Curran D, Lorenz R, Czako P. Gastric outlet obstruction at 30 weeks’ gestation. Obstet Gynecol. 1999;93(5 Pt 2):851.PubMed
138.
Kochhar R, Dutta U, Sethy PK, et al. Endoscopic balloon dilation in caustic-induced chronic gastric outlet obstruction. Gastrointest Endosc. 2009;69:800–5.PubMed
139.
Kochhar R, Kochhar S. Endoscopic balloon dilation for benign gastric outlet obstruction in adults. World J Gastrointest Endosc. 2010;2:29–35.PubMed
140.
Böhm B, Ablassmaier B, Müller JM. Laparoskopische Chirurgie am oberen gastrointestinaltrakt. Chirurg. 2001;72:349–61.PubMed
141.
Cellan-Jones CJ. A rapid method of treatment in perforated duodenal ulcer. Br Med J. 1929;36:1076–7.
142.
Graham RR. The treatment of perforated duodenal ulcers. Surg Gynecol Obstet. 1937;64:235–8.
143.
Fisher JE. Mastery of surgery. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2007.
144.
http://www.flickr.com/photos/trebore/2044146244/meta/.
145.
Mussey RD. Operations of necessity during pregnancy. Proc Mayo Clin. 1927;2:156.
146.
Jennings D. Perforated peptic ulcer; changes in age incidence and sex- distribution in the last 150 years. Lancet. 1940;1(395–8):444–7.
147.
Jones FA. Haematemesis and melaena, with special reference to bleeding peptic ulcer. Br Med J. 1947;2:441–6.PubMed
148.
Registrar General. Statistical Reviews of England and Wales for the years 1900–59.
149.
Bager B. Beitrag zur kenntnis über vorkommen, klinik und behandlung von perforierten magenund duodenal gesch wuren nebst einer untersuchung über die spatresultate nach verschiedenen operations methoden. Acta Chir Scand. 1929;(suppl 11):5–320.
150.
Illingworth CFW, Scott LDW, Jamieson RA. Acute perforated peptic ulcer in the west of Scotland. Br Med J. 1944;2:617–20.
151.
Weir RD. Perforated peptic ulcer in North-East Scotland. Scot Med J. 1960;5:257–64.PubMed
152.
Bockus HL. Gastroenterology. Philadelphia: Saunders; 1943.
153.
Adams C. Die Behandlung des Magen und Zwölffingerdarmgeschwürs mit Keimdriisenhormonen. Gastroenterologia. 1942;66:343–9.
154.
Anderson GW. Pregnancy complicated by acute perforated peptic ulcer. Am J Obstet Gynecol. 1942;43:883.
155.
Atkinson AJ, Ivy AC. Further attempts to produce achlorhydria. Am J Dig Dis. 1938;5:30–5.
156.
Doll R. Peptic ulcer: epidemiology. In: Avery Jones F, editor. Modern trends in gastroenterology. London: Butterworth; 1958. p. 361–79.
157.
Logan WPD. General practitioners’ records. General Register Office: Subjects no. 7. HM Stationery Office. 1953.
158.
Logan WPD, Cushion AA. Morbidity statistics from general practice, vol. I, General. General Register Office: Subjects no. 14. HM Stationery Office. 1958.
159.
Rosenbaum S. Cross-sectional review of morbidity among young soldiers. Br J Prev Soc Med. 1959;13:103–27.PubMed
160.
Pulvertaft CN. Peptic ulcer in town and country. Br J Prev Soc Med. 1959;13:131–8.PubMed
161.
Susser M, Stein Z. Civilization and peptic ulcer. 1962. Int J Epidemiol. 2002;31:13–7.PubMed
162.
McConnell DB, Baba GC, Deveney CW. Changes in surgical treatment of peptic ulcer disease within a veterans hospital in the 1970s and the 1980s. Arch Surg. 1989;124:1164–7.PubMed
163.
Vaira D, Menegatti M, Miglioli M. What is the role of Helicobacter pylori in complicated ulcer disease? Gastroenterology. 1997;113(Suppl):S78–84.PubMed
164.
Irvin TT. Mortality and perforated peptic ulcer: a case for risk stratification in elderly patients. Br J Surg. 1989;76:215–8.PubMed
165.
Blomgren LG. Perforated peptic ulcer: long-term results after simple closure in the elderly. World J Surg. 1997;21:412–4.PubMed
166.
Thomsen RW, Riis A, Christensen S, et al. Diabetes and 30-day mortality from peptic ulcer bleeding and perforation: a Danish population-based cohort study. Diabetes Care. 2006;29:805–10.PubMed
167.
Møller MH, Adamsen S, Wøjdemann M, Møller AM. Perforated peptic ulcer: how to improve outcome? Scand J Gastroenterol. 2009;44:15–22.PubMed
168.
Hermansson M, Staël von Holstein C, Zilling T. Surgical approach and prognostic factors after peptic ulcer perforation. Eur J Surg. 1999;165:566–72.PubMed
169.
Møller MH, Adamsen S, Thomsen RW, Møller AM. Preoperative prognostic factors for mortality in peptic ulcer perforation – a systematic review. Scand J Gastroenterol. 2010;45:785–805.PubMed
170.
Svanes C, Salvesen H, Espehaug B, et al. A multifactorial analysis of factors related to lethality after treatment of perforated gastroduodenal ulcer. 1935–1985. Ann Surg. 1989;209:418–23.PubMed
171.
Egberts JH, Summa B, Schulz U, et al. Impact of preoperative physiological risk profile on postoperative morbidity and mortality after emergency operation of complicated peptic ulcer disease. World J Surg. 2007;31:1449–57.PubMed
172.
Koç M, Yoldaş O, Kiliç YA, et al. Comparison and validation of scoring systems in a cohort of patients treated for perforated peptic ulcer. Langenbecks Arch Surg. 2007;392:581–5.PubMed
173.
Boey J, Wong J, Ong GB. Bacteria and septic complications in patients with perforated duodenal ulcers. Am J Surg. 1982;143:635–9.PubMed
174.
Fong IW. Septic complications of perforated peptic ulcer. Can J Surg. 1983;26:370–2.PubMed
175.
Chabannes. Lyon Med. 1903;101:529.
176.
Szenes A. Über den Einfluss der Schwangerschaft, der Menstruation, und des Klimakterium auf das Magen- und Duodenalgeschwür. Mitt Grenzgeb Med Chir. 1924;37:652–91.
177.
Engemise S, Oshowo A, Kyei-Mensah A. Perforated duodenal ulcer in the puerperium. Arch Gynecol Obstet. 2009;279:407–10.PubMed
178.
Sandweiss DJ, Podolsky MB, Saltzstein HC, Farbman AA. Deaths from perforation and hemorrhage of gastroduodenal ulcer during pregnancy and puerperium. Am J Obstet Gynecol. 1943;45:131–6.
179.
Howkins J. Br Surg Pract. 1950;7:116.
180.
Scott WA. Surgical complications during pregnancy and labour. Am J Obstet Gynecol. 1945;49:494.
181.
Durst JB, Klieger JA. A report of a fatal hemorrhage due to peptic ulcer in pregnancy. Am J Obstet Gynecol. 1955;70:448–51.PubMed
182.
Rider JA, Kirsner JB, Palmer WL. Active duodenal ulcer in pregnancy. Gastroenterology. 1953;24:357–61.PubMed
183.
Jones FA. Haematemesis and melaena, with special reference to bleeding peptic ulcer. Br Med J. 1947;2:477–82.PubMed
184.
Hooker RS. Maternal mortality in New York City. A study of all puerperal deaths. New York Academy of Medicine Committee on Public Relations, 1930-1932. New York: The Commonwealth Fund; 1933. p. 234.
185.
Strange SL. Massive haemorrhage from duodenal ulcer in pregnancy. Proc R Soc Med. 1962;55:798–9.PubMed
186.
Ross IG. Perforated ulcer in pregnancy. Br Med J. 1958;2:693.
187.
Burkitt R. Perforated peptic ulcer in late pregnancy. Br Med J. 1961;2:938–9.PubMed
188.
Lindell A, Tera H. Perforated gastroduodenal ulcer in late pregnancy, operated upon with survival of both mother and child. J Obstet Gynecol Br Emp. 1962;69:493–5.
189.
Johnston JL. Peptic ulcer and pregnancy; deaths from perforation and hemorrhage of peptic ulcer during pregnancy. Obstet Gynecol. 1953;2:290–6.PubMed
190.
Langmade CF. Epigastric pain in pregnancy toxemias; a report of fatal peptic ulcers in toxemias. West J Surg Obstet Gynecol. 1956;64:540–4.PubMed
191.
Baxter CR. Peptic ulcer in pregnancy. Br Med J. 1948;2:1037.
192.
Logan Jr WD, Hendee AE. Am Surg. 1962;28:728.
193.
Winchester DP, Bancroft BR. Perforated peptic ulcer in pregnancy. Am J Obstet Gynecol. 1966;94:280–1.PubMed
194.
Becker-Andersen H, Husfeldt V. Peptic ulcer in pregnancy report of two cases of surgically treated bleeding duodenal ulcer. Acta Obstet Gynecol Scand. 1971;50:391–5.PubMed
195.
Goh JT, Sidhu MS. Perforated duodenal ulcer-an unusual and often forgotten cause of an acute abdomen in pregnancy. Aust N Z J Obstet Gynaecol. 1995;35:433–4.PubMed
196.
Hsu CC, Liu YP, Lien WC, et al. A pregnant woman presenting to the ED with Valentino’s syndrome. Am J Emerg Med. 2005;23:217–8.PubMed
197.
Gali BM, Ibrahim AG, Chama CM, et al. Perforated peptic ulcer (PPU) in pregnancy during Ramadan fasting. Niger J Med. 2011;20:292–3.PubMed
198.
Erez O, Maymon E, Mazor M. Acute gastric ulcer perforation in a 35 weeks’ nulliparous patient with gastric banding. Am J Obstet Gynecol. 2004;191:1721–2.PubMed
199.
Segal M. Peptic ulcer perforation in pregnancy. Br Med J. 1959;1:1040.
200.
Essilfie P, Hussain M, Bolaji I. Perforated duodenal ulcer in pregnancy – a rare cause of acute abdominal pain in pregnancy: a case report and literature review. Case Rep Obstet Gynecol. 2011;2011:263016.PubMed
201.
Munro A, Jones PF. Abdominal surgical emergencies in the puerperium. Br Med J. 1975;4:691–4.PubMed
202.
Jones PF, McEwen AB, Bernard RM. Haemorrhage and perforation complicating peptic ulcer in pregnancy. Lancet. 1969;294:350–2.
203.
Grassi R, Romeno S, Pinto A, et al. Gastro-duodenal perforations: conventional plain film, US and CT findings in 166 consecutive patients. Eur J Radiol. 2004;50:30–6.PubMed
204.
Uchikova E, Uchikov A, Terzhumanov R, et al. Perforation of duodenal ulcer in the puerperium – a case report. Akush Ginekol (Sofiia). 2004;43:53–4.
205.
Kaczmarek R. Peptic ulcer following Cesarean section. Pol Tyg Lek. 1970;25:1905–6.PubMed
206.
Alabi-Isama L, Bolaji I, Essilfie P. Perforated duodenal ulcer in the puerperium – a rare cause of acute abdominal pain – case report and literature review. Int J Gynecol Obstet. 2009;107 Suppl 2:S414.
207.
Sule EA, Omo-Aghoja L. Perforated duodenal ulcer in the immediate puerperium following caesarean section. J Obstet Gynaecol. 2010;30:633–5.PubMed
208.
McGarvey RN, Freeman JJ, Fox PF. Perforated peptic ulcer in the puerperium. Am J Obstet Gynecol. 1952;64:655–9.PubMed
209.
Opitz C. The acute perforation of a stress ulcer in puerperium following eclampsia. (case report). Zentralbl Gynakol. 1971;93:388–90.PubMed
210.
Gaĭstruk VV, Ponomarev AP, Slobodianiuk GI. Stomach ulcer perforation in the early puerperal period. Vestn Khir Im I I Grek. 1980;125:81.PubMed
211.
Parry GK. Perforated duodenal ulcer in the puerperium. N Z Med J. 1974;80:448–9.PubMed
212.
Murray A, Holdcroft A. Incidence and intensity of postpartum lower abdominal pain. Br Med J. 1989;298:1619.
213.
Grainger AR, Allison DJ. Diagnostic radiology – a textbook of medical imaging. 4th ed. Edinburgh: Churchill Livingstone; 2001. p. 993–4.
214.
Woodring JH, Heiser MJ. Detection of pneumoperitoneum on chest radiographs: comparison of upright lateral and posteroanterior projections. Am J Roentgenol. 1995;165:45–7.
215.
Larson JD, Patatanian E, Miner PB, et al. Double-blind, placebo controlled study of ranitidine for gastroesophageal reflux symptoms during pregnancy. Obstet Gynecol. 1997;90:83–7.PubMed
216.
Finkelstein W, Isselbacker KJ. Cimetidine. N Engl J Med. 1978;229:992–6.
217.
Briggs GG, Freeman RY, Yaffe SJ. Drugs in pregnancy and lactation: a reference guide to fetal and neonatal risk. Baltimore: William and Wilkins; 2002.
218.
Kalle B. Delivery outcomes after the use of acid-suppressing drugs in early pregnancy with special reference to omeprazole. Br J Obstet Gynaecol. 1998;105:877–83.
219.
Smallwood RA, Berlin RG, Catagnoli N, et al. Safety of acid suppressing drugs. Dig Dis Sci. 1995;40(Suppl):635–8.
220.
Savarino V, Giasti M, Scalabrini P, et al. Famotidine has no significant effect on gonadal function in men. Gastroenterol Clin Biol. 1988;12:19–22.PubMed
221.
Morton DM. Pharmacology and toxicity of nizatidine. Scand J Gastroenterol. 1987;22 Suppl 136:1–8.
222.
Neubauer BL, Goode RL, Bert KK, et al. Endocrine effects of a new histamine H2 receptor antagonist, nizatidine, in the male rat. Toxicol Appl Pharmacol. 1990;102:219–32.PubMed
223.
Prilosec (product information). Wilmington, DC: Astra-Zeneca; 2004.
224.
Wilton LV, Pearce GL, Martin RM, et al. The outcomes of pregnancy in women exposed to newly marketed drugs in general practice in England. Br J Obstet Gynaecol. 1998;105:882–9.PubMed
225.
Nikfar S, Abdollahi M, Moretti ME, et al. Use of proton pump inhibitors during pregnancy and rates of major malformations. A meta-analysis. Dig Dis Sci. 2002;47:1526–9.PubMed
226.
Nielsen GL, Sorensen HT, Thulctrup AM, et al. The safety of proton pump inhibitors in pregnancy. Aliment Pharmacol Ther. 1999;13:1085–9.PubMed
227.
Larkin A, Loebstein R, Addis A, et al. The safety of omeprazole during pregnancy: a multicenter prospective controlled study group. Am J Obstet Gynecol. 1998;179:727–30.
228.
Mahfoud T, Elhassani ME, Hafidi MR, et al. Krukenberg tumor secondary to gastric carcinoma in a pregnant woman: a case report and literature review. Biol Biomed Rep. 2012;2:32–6.
229.
Prevacid (product information). Lake Forest: TAP Pharmaceutical; 2005.
230.
Diav-Citrin O, Arnon J, Shechtman S, et al. The safety of proton pump inhibitors in pregnancy: a multicenter prospective controlled study. Aliment Pharmacol Ther. 2005;21:269–75.PubMed
231.
Somogyi A, Gugler R. Cimetidine excretion in breast milk. Br J Clin Pharmacol. 1979;7:627–9.PubMed
232.
Courtney TP, Shaw RW, Cedar E, et al. Excretion of famotidine in breast milk. Br J Clin Pharmacol. 1988;26:639.
233.
Obermeyer BD, Bergstrom PF, Callagher JT, et al. Secretion of nizatidine into human breast milk after single and multiple doses. Clin Pharmacol Ther. 1990;47:724–30.PubMed
234.
Physician’s desk reference. 58th ed. Montvale: Medical Economics; 2002.
235.
Committee on Drugs. American Academy of Pediatrics. The transfer of drugs and other chemicals into human milk. Pediatrics. 1994;93:137–50.
236.
Marshall JK, Thompson ABR, Armstrong D. Omeprazole for refractory gastroesophageal reflux disease during pregnancy and lactation. Can J Gastroenterol. 1998;12:225–7.PubMed
237.
Tew WL, Holliday RL, Phibbs G. Perforated duodenal ulcer in pregnancy with double survival. Am J Obstet Gynecol. 1976;125:1151–2.PubMed
238.
Paul M, Tew WL, Holliday RL. Perforated peptic ulcer in pregnancy with survival of mother and child: case report and review of the literature. Can J Surg. 1976;19:427–9.PubMed
239.
Yamagata S, Uzuka Y. Malignant tumor during pregnancy – from the standpoint of internal medicine. J Cancer Clin. 1970;16:574–84.
240.
Ueo H, Okudaira Y, Hirabayashi M. Gastric cancer associated with pregnancy. A case report of early gastric cancer and review of 100 cases in Japan. J Jpn Soc Clin Surg. 1989;50:312–8.
241.
Silverberg E, Lubera J. Cancer statistics. Cancer. 1989;39:3–20.
242.
Kodama I, Takeda J, Koufuji K, et al. Gastric cancer during pregnancy. Kurume Med J. 1997;44:179–83.PubMed
243.
Fujimura M, Fukunda K. Gastric cancer associated with pregnancy. J Kinki Obstet. 1916;3:208.
244.
Jaspers VK, Gillessen A, Quakernack K. Gastric cancer in pregnancy: do pregnancy, age or female sex alter the prognosis? Case reports and review. Eur J Obstet Gynecol Reprod Biol. 1999;87:13–22.PubMed
245.
Fill S, Taran A, Schulz HU. Sister Mary Joseph’s nodule as the first sign of pregnancy-associated gastric cancer: a case report. World J Gastroenterol. 2008;14:951–3.PubMed
246.
Jasmi AY, Normala B, al-Amin MD. Perforated malignant gastric ulcer in a pregnant young adult: a case report. Med J Malaysia. 2000;55:135–7.PubMed
247.
Chong VH, Lim CC. Advanced disseminated gastric carcinoma in pregnancy. Singapore Med J. 2003;44:471–2.PubMed
248.
Yücesoy G, Büyükgebiz O, Yildiz K, et al. Gastric carcinoma diagnosed at the third trimester: a case report. Arch Gynecol Obstet. 2006;274:47–9.PubMed
249.
Gojnic M, Dugalic V, Vidakovic S. Hyperemesis or stomach carcinoma in pregnancy – a true diagnosis with two lives saved: a case report. Clin Exp Obstet Gynecol. 2005;32:201–2.PubMed
250.
Glisic A, Atanackovic J. Krukenberg tumor in pregnancy. The lethal outcome. Pathol Oncol Res. 2006;12:108–10.PubMed
251.
Unek IT, Celtık A, Alacacioğlu A. Gastric carcinoma during pregnancy: report of a case. Turk J Gastroenterol. 2007;18:41–3.PubMed
252.
Kurt M, Aksoy S, Cizginer S. Gastric cancer and the coincidental finding of herpetic esophagitis immediately after pregnancy: a case report. J Reprod Med. 2007;52:425–7.PubMed
253.
Ohsawa S, Kondo Y, Shiroto H, et al. A case of an early gastric cancer associated with a pregnancy. Jpn J Cancer Clin. 1992;38:1269–73.
254.
Shomura Y, Murabayashi K, Hayashi M, et al. A resected case of juvenile gastric cancer causing perforation during the course of the observation of pregnancy and an ovarian tumor. J Jpn Soc Clin Surg. 1995;56:741–5.
255.
Shinagawa T, Abe M, Tadokoro M, et al. A gastric carcinoma in a young pregnant woman with a bilateral breast metastases autopsied and breast carcinoma case findings. Jpn J Cancer Clin. 1991;37:48–54.
256.
Sato Y, Yokoyama Y, Narikawa N, et al. Krukenberg tumor metastasized from stomach cancer incidentally discovered at the caesarean section: a case report. Tokai J Obstet Gynecol. 2006;43:123–6.
257.
Shibata D, Kawai M, Niwa Y, et al. Pregnancy with gastric cancer: a case report. Obstet Gynecol (Tokyo). 1999;66:701–4.
258.
Serikawa T, Shichiri K, Sanada H. Two cases of pregnancy associated with gastric cancer. Obstet Gynecol Ther. 1996;73:605–7.
259.
Maeda S, Takigawa J, Toyoyama H, et al. Two cases of gastric cancer during pregnancy. Surgery (Geka). 2007;69:1077–80.
260.
Yoshida M, Matsuda H, Furuya K. Successful prognosis of pregnancy with gastric cancer in the second trimester: a case report. J Jpn Soc Perinat Neonat Med. 2007;43:140–2.
261.
Ando H, Maeda S, Kameoka N, et al. A case of perforated gastric cancer associated with pregnancy that was recognized at caesarean operation. J Abdom Emerg Med. 2007;27:777–9.
262.
Ozeki T, Soeda S, Watanabe T, et al. Krukenberg tumor increased rapidly with pregnancy: a case report. J Jpn Soc Gynecol Oncol. 2006;24:424–8.
263.
Kurabayashi T, Isii K, Suzuki M. Advanced gastric cancer and a concomitant pregnancy associated with disseminated intravascular coagulation. Am J Perinatol. 2004;21:295–8.PubMed
264.
Umezawa K, Kigawa N, Sudo Y, et al. A case of pregnancy with gastric cancer. Tokyo J Obstet Gynecol. 2004;53:346–8.
265.
Shimizu M, Nishida M, Eto M, et al. Gastric cancer during pregnancy: rapid cervical lymph nodes swelling and pericardial effusion at third trimester, a case report. Obstet Gynecol (Tokyo). 2004;71:381–4.
266.
Tanaka Y, Komiyama M, Akiba Y, et al. A case of advanced gastric cancer diagnosed after the delivery. Kanagawa Dist J Jpn Obstet Gynecol Soc. 2001;37:134–7.
267.
Nakagawa K. Four cases of gastric cancer during pregnancy. J Jpn Coll Surg. 2000;25:892–5.
268.
Igarashi S, Kawaguchi T, Hoshi N. Early gastric carcinoma with widespread metastasis and pulmonary tumor thrombotic microangiopathy (PTTM): report of an autopsy case. Stomach Intestine. 1997;32:861–5.
269.
Ogawa T, Higashi S, Okada Y, et al. A resected case of gastric cancer with Krukenberg tumor during pregnancy. Surgery (Geka). 1997;59:1391–3.
270.
Sakou T, Seki Y, Takeuchi Y, et al. A case of cancer of the stomach in a pregnant woman undergoing cesarean section and gastrectomy at the same time. J Jpn Soc Clin Surg. 1996;57:1631–4.
271.
Kishikawa H, Nishiwaki N, Ito K, et al. Perforated gastric cancer associated with the delivery which is misdiagnosed as abruption of placenta. J Jpn Soc Clin Surg. 1992;53:2986–9.
272.
Krukenberg F. Über das Fibrosarcoma Ovarii mucocellulare (Carcinomatodes). Arch Gynakol. 1896;50:287.
273.
Tamussino K, Scholl W, Reich O, Winter R. Gastric carcinoma presenting as a Krukenberg tumor in the 24th week of gestation. Eur J Obstet Gynecol Reprod Biol. 1995;62:251–2.PubMed
274.
Yakushiji M, Tazaki T, Nishumura H, Kato T. Krukenberg tumors of the ovary: a clinicopathologic analysis of 112 cases. Acta Obst Gynaec JPN. 1987;3:479–85.
275.
Sandemeier D, Lobrunus JA, Vial Y, et al. Bilateral Krukenberg tumor of the ovary during pregnancy. Eur J Gynecol Oncol. 1999;21:58–60.
276.
Sakamoto K, Kanda T, Ohashi M, et al. Management of patients with pregnancy-associated gastric cancer in Japan: a mini-review. Int J Clin Oncol. 2009;14:392–6.PubMed
277.
Khatib F, Shaya M, Samueloff A. Gastric carcinoma with metastasis to the placenta and amniotic fluid: case report and review of the literature. Eur J Obstet Gynecol Reprod Biol. 2003;107:208–9.PubMed
278.
Kath R, Fiehler J, Schneider CP, Höffken K. Gastric cancer in very young adults: apropos four patients and a review of the literature. J Cancer Res Clin Oncol. 2000;126:233–7.PubMed
279.
Maeta M, Yamashiro H, Oka A, et al. Gastric cancer in the young, with special reference to 14 pregnancy-associated cases: analysis based on 2,325 consecutive cases of gastric cancer. Surg Oncol. 1995;58:191–5.
280.
Furukawa H, Iwanaga T, Hicatsuka M, et al. Gastric cancer in young adults: growth accelerating effect of pregnancy and delivery. Surg Oncol. 1994;55:3–6.
281.
Hornung M, Vogel P, Schubert T, et al. A case of virilization induced by a Krukenberg tumor from gastric cancer. World J Surg Oncol. 2008;6:19.PubMed
282.
Davis JL, Chen MD. Gastric carcinoma presenting as an exacerbation of ulcers during pregnancy. A case report. J Reprod Med. 1991;36:450–2.PubMed
283.
Ha HK, Baek SY, Kim SH, et al. Krukenberg’s tumor of ovary: MR imaging features. Am J Roentgen. 1995;164:1435–9.
284.
Reichelt DC, Scherer A, Blondin D. Initial diagnosis of Krukenberg tumor in pregnancy. Rofo. 2009;181:483–5.PubMed
285.
Amendolara M, Barbarino C, Bucca D, et al. Krukenberg tumour: diagnostic findings and surgical therapy. Recent acquisitions. Chir Ital. 2007;59:591–5.PubMed
286.
Cheong JH, Hyung WJ, Chen J, et al. Survival benefit of metastasectomy for Krukenberg tumors from gastric cancer. Gynecol Oncol. 2004;94:477–82.PubMed
287.
Kim WY, Kim TJ, Kim SE, et al. The role of cytoreductive surgery for nongenital tract metastatic tumors to the ovaries. Eur J Obstet Gynecol Reprod Biol. 2010;149:97–101.PubMed
288.
Fazeny B, Marosi C. Gastric cancer as an essential differential diagnosis of minor epigastric discomfort during pregnancy. Acta Obstet Gynecol Scand. 1998;77:469–71.PubMed
289.
Yildirim Y, Erkan N, Avci E, Elveren B. Perforated gastric cancer complicating early postpartum period of pregnancy. Acta Chir Belg. 2009;109:534–7.PubMed
290.
Louw JT, Louw JH. Extra-genital surgical emergencies of the abdomen in pregnancy. S Afr Med J. 1954;28:788–93.PubMed
291.
Carson J. Edinb Med Surg J. 1946;66:25–31.
292.
Glassman O. Subcutaneous rupture of the stomach, traumatic & spontaneous. Ann Surg. 1929;89:247–63.PubMed
293.
Miller J. Spontaneous rupture of the stomach during labor. N Engl J Med. 1933;209:1085–8.
294.
Christoph RF, Pinkham EW. Unexpected rupture of the stomach in the postpartum period: a case report. Ann Surg. 1961;154:100–2.PubMed
295.
Fiester RF, Zinn LD. Spontaneous gastric rupture during pregnancy (case report). W V Med J. 1975;71:110.PubMed
296.
Seon Cha A, Krew MA, Tamlyn T, Gill P. Gastric rupture associated with pregnancy. Obstet Gynecol. 2002;100:1072–4.PubMed
297.
Mirsky S, Garlock J. Spontaneous rupture of the stomach: unusual clinical features. Ann Surg. 1965;161:466–8.PubMed
298.
Ilgenfritz HC. Preoperative and postoperative care of surgical patients. St. Louis: C. V. Mosby Co.; 1948. p. 66.
299.
Harkins HN. Surgical diseases of the stomach and duodenum. In: Allen JG, Harkins HN, Moyer CA, Rhoads JE, editors. Surgery, practice & principles. Philadelphia: J. B. Lippincott Company; 1957. p. 671.
300.
Carlson E, Ortiz C. Etiology of paralytic ileus and acute dilatation of the stomach; studies of 17-hydroxycorticoid levels. Surgery. 1960;47:177–83.PubMed
301.
Millar TM, Bruce J, Paterson JR. Spontaneous rupture of the stomach. Br J Surg. 1957;44:513–6.PubMed
302.
Burket G. Spontaneous rupture of the stomach: report of a case. J Am Med Assoc. 1949;139:27–8.PubMed
303.
Revilliod E. Rupture de l’estomac. Rev Med Suisse Romai. 1885;5:5–13.
304.
Chapius G, Tabrizian M, Saegesser F. Ruptures spontanees de l’oesophage et de l’estomac et syndrome de Mallory-Weiss. Schweiz Med Wshr. 1970;100:1060–6.
305.
Demetriades D, Van Der Veen BW, Hatzitheouphilous C. Spontaneous rupture of the stomach in an adult. S Afr Med J. 1982;61:23–4.PubMed
306.
Albo R, de Lorimier A, Silen W. Spontaneous rupture of the stomach in the adult. Surgery. 1963;53:797–805.PubMed
307.
Morton JH, Hubbard LT. Unexpected intestinal rupture in association with pregnancy. Obstet Gynecol. 1959;14:214.PubMed
308.
Skarstein A, Lekven J. Influence of gastric banding on stomach blood supply with or without concurrent splenectomy. Am J Surg. 1985;149:351–6.PubMed
309.
Weiss HG, Nehoda H, Labeck B, et al. Pregnancies after adjustable gastric banding. Obes Surg. 2001;11:303–6.PubMed