Michael Weston1
(1)
Department of Clinical Radiology, St James’s University Hospital, Leeds, England, UK
Michael Weston
Email: michael.weston2@nhs.net
22.1 Introduction
The renal tract undergoes physiological changes during pregnancy. Pregnant women may suffer from urinary tract infections, colic, stone disease and changes in renal function caused by pregnancy-related hypertensive disorders. History taking and clinical parameters such as blood pressure, urinalysis and culture as well as measurement of electrolytes may help the clinician manage the patient, but there is still a need for imaging. Ultrasound is the mainstay of imaging in pregnant women because of its ready availability and its lack of ionising radiation or any proven adverse effect on the fetus. Computed tomography (CT) is known to be the best test for urinary tract calculi in the non-pregnant patient. The purpose of this chapter is to help the reader to understand how magnetic resonance (MR) imaging fits into the cascade of imaging for renal disease in the pregnant woman.
22.2 Physiological Changes in Pregnancy
There are quite rapid changes in haemodynamics and biochemistry in the first trimester of pregnancy. Cardiac output and plasma volume increase by up to 40 %. This combined with a decrease in renal vascular resistance results in a substantial rise in glomerular filtration rate of 40–65 % [1]. This has a physical effect of making the kidneys larger by 1.0–1.5 cm by swelling the interstitial fluid volume. Biochemically, the creatinine clearance is increased, and the serum creatinine and urea levels are lowered.
Acid–base balance is affected by a relative respiratory alkalosis causing a compensatory increase in renal bicarbonate excretion.
Stone formation is altered during pregnancy by the changes in urine composition. Analysis of stones found during pregnancy shows that there is a much greater preponderance of calcium phosphate stones (about 66 % of the total) than in the non-pregnant population. The rest of the stones are calcium oxalate. Three quarters of women who form stones during pregnancy have no prior history of stones. Formation of calcium phosphate stones is pH dependant, so it is likely that the physiological elevation in urinary calcium excretion and pH during pregnancy are responsible for the observed changes [2, 3].
There has been an increase in stone incidence in the non-pregnant population over recent decades thought to be due to changes in diet, obesity, environmental temperatures and diabetes. One institution has shown that despite a near threefold rise in stone diagnoses in their non-pregnant population, there was no associated rise in the incidence of stones in pregnancy [4].
Anatomical changes occur in the pelvicalyceal systems and ureters. Physiological hydronephrosis is described as occurring in the right kidney in up to 90 % of pregnant women and in the left kidney on 67 %. There are two contributory theories: mechanical and hormonal [5].
The mechanical theory is the compression of the ureters by the gravid uterus against the pelvic brim (Fig. 22.1). Support for this theory comes from the absence of dilation of the ureters below the pelvic brim and also the absence of dilation in pelvic kidneys and in those who have had urinary diversions. Dilation is commoner on the right because of the dextrorotation of the normal gravid uterus or because the sigmoid colon protects the left ureter. Nulliparous patients have a higher rate of hydronephrosis supposedly because they have a better abdominal wall muscle tone.

Fig. 22.1
An intravenous urogram from the archives showing the dilated right ureter tapering as it passes between the pelvic brim and the gravid uterus
The hormonal theory is that progesterone affects smooth muscle dilation causing reduced peristalsis and greater dilation. This is likely to be the predominant cause in the first trimester when the uterus is not large enough to have a mechanical effect, but thereafter, mechanical causes are predominant.
22.3 Symptomatology and Demographics
Symptoms of renal disease in pregnancy are nearly all related to infection or colic. The physiological changes of pregnancy itself may, however, also produce symptoms of abdominal or flank pain, nausea and lower urinary tract symptoms, and there may be other pregnancy-related discomforts that are harder to classify and may confuse any presentation.
Stone formation risk is higher in multiparous than primiparous women. The incidence is higher in Caucasians and those with a history of renal disease and hypertension. Up to a third of women presenting with stones in pregnancy will have a prior history of stones [5].
Flank and abdominal pain is the commonest symptom in stone disease, occurring in up to 100 % of all confirmed cases. Pain may occur in other conditions too, and consideration will need to be given to differential diagnoses such as pyelonephritis, appendicitis, diverticulitis or placental abruption. Otherwise, the main consideration is to distinguish the pain due to ureteric stones from that associated with physiological dilation. Stones usually cause more severe pain requiring greater analgesia. Left-sided pain is more likely to be due to stone [6]. Stones usually present in the second and third trimesters [7].
Frank haematuria has been reported in up to a third of women with proven ureteric calculi. Microscopic haematuria is much commoner but non-specific and is generally regarded as unhelpful in identifying stone disease [8].
Stone disease in pregnant women is associated with recurrent miscarriage, pre-eclampsia, chronic hypertension, gestational diabetes and a higher rate of Caesarean section. It is also associated with urinary tract infections. However, no increased rate of adverse perinatal outcome [9] or congenital anomaly [10] has been found. There is disagreement on the effect on preterm delivery with some studies finding no effect [9, 10] and others showing a doubling of the likelihood [11].
The prevalence of symptomatic stone disease in the pregnant population is variously quoted as between 1:200 and a much lower incidence. Most studies fall in the range of 1:200–1:300. The likelihood of a woman who is hospitalised for renal colic like pain having a stone as the underlying cause is about 20 % [12]. Some authors go so far as to state that almost a quarter of women diagnosed with stones have an inaccurate diagnosis [13].
22.4 Infections
Urinary tract infections are common in pregnant women. Pregnant women should be screened for asymptomatic bacteriuria and treated if it is present [14]. The physiological and structural changes in the pregnant woman’s urinary tract promote ascending infection from the urethra. There is a 20–50-fold increased risk of pyelonephritis in women with bacteriuria compared to those without. The prevalence of asymptomatic bacteriuria in pregnant women is around 7 % [15].
Over 70 % of asymptomatic bacteriuria infections in pregnancy are due to E. coli. The remainder is due to Klebsiella species, Proteus species (particularly in diabetics or obstructed systems), enterococci, Staphylococcus saprophyticus, pseudomonas and lastly streptococci. Antibiotic therapy during pregnancy needs to be modified to take account of the potential of some antibiotics to cause fetal harm. Tetracyclines, gentamicin and other aminoglycosides and chloramphenicol are all proven to cause fetal harm and must be avoided. Amoxicillin, ampicillin, nitrofurantoin and penicillins have been taken by large numbers of pregnant women without any proven fetal harm. It is best to check the formulary for contraindications when choosing a new antibiotic therapy.
Imaging is not needed for uncomplicated urinary tract infections that respond to treatment. If the women does not respond to antibiotics or has associated flank pain or other symptoms suggesting pyelonephritis or stones, then imaging becomes appropriate. Ultrasound is the best first-line test because of its ready availability and lack of ionising radiation.
Ultrasound features of pyelonephritis include global swelling with thickening of the urothelium. There may be loss of the normal corticomedullary differentiation and effacement of sinus echoes. Focal pyelonephritis may manifest as mass lesions of various echogenicities; some are echo-bright, whereas others are echo-poor (Fig. 22.2). The lesions may be wedge shaped and are often ill defined. The affected area usually has decreased vascularity on Doppler.

Fig. 22.2
A longitudinal ultrasound image of the kidney showing a focal segmental region of cortical hyper-echogenicity, which in the right clinical context is diagnostic of focal pyelonephritis
If the ultrasound has been unhelpful or a focal lesion needs clarification, then MR scan is the next imaging test of choice. Even in the non-pregnant patient, it has now been shown that diffusion-weighted MR scan outperforms CT in the diagnosis of pyelonephritis (sensitivities: DWI 95.3 %, non-contrast CT 66.7 % and contrast-enhanced CT 88.1 %) [16]. Likewise, diffusion-weighted imaging (DWI) performs just as well as contrast-enhanced MR in the detection of pyelonephritis, so there is no need to expose a pregnant women to gadolinium contrast agents [17]. Diffusion images can be obtained using a non-breath hold, single-shot echo-planar sequence with b values of 0, 600 and 1000. Areas of inflammation show restricted diffusion and are hypointense on T2-weighted images (Fig. 22.3). Sequential MR scans can be used to show resolution or to look for further complications such as abscess formation.
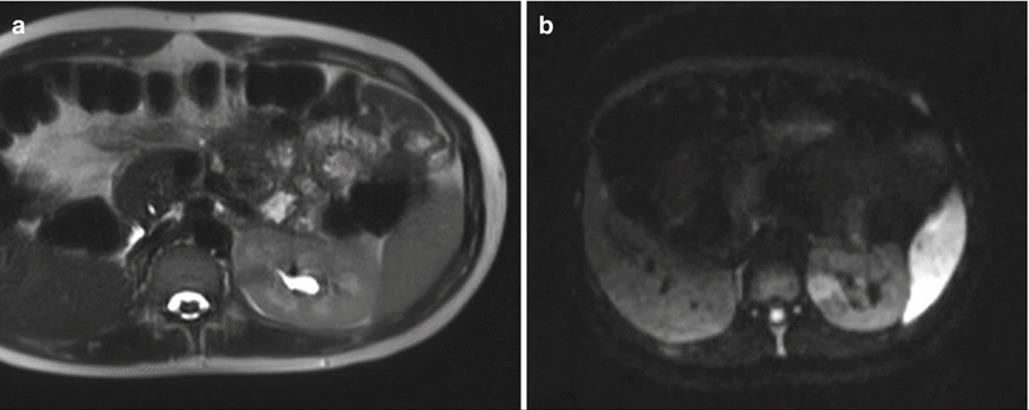
Fig. 22.3
T2-weighted (a) and diffusion-weighted (b) axial images of a focal area of pyelonephritis in the left kidney. The region is dark on T2- and bright on diffusion-weighted images. The diffusion-weighted images make the lesion more conspicuous
22.5 Renal Tract Dilation Versus Obstruction
22.5.1 Diagnosis
The essence of imaging in the presence of flank pain is to distinguish physiological dilation of the urinary tract due to pregnancy from the dilation caused by the presence of a ureteric stone. There is a very poor correlation of flank pain with the presence of hydronephrosis. A longitudinal study on pregnant women showed that many with hydronephrosis do not have any flank pain and that those with flank pain only have hydronephrosis in a third [18]. All cases resolved by 6 weeks post-partum.
22.5.2 Imaging
22.5.2.1 First-Line Imaging
Ultrasound is the primary imaging modality, agreed by all authors because of the lack of ionising radiation, ready availability and low cost. Ultrasound techniques involve identifying renal tract dilation and stones on greyscale imaging, using colour Doppler to look for the ring-down artefact from stones and to evaluate ureteric jets into the bladder and using spectral Doppler to assess the resistance index of blood flow in the interlobar arteries of the kidneys. Ultrasound is limited by the inability to view the whole ureter and by relative insensitivity to small calculi. Transvaginal ultrasound can improve visualisation of the distal ureter. Indeed, finding a dilated ureter below the level of the pelvic brim (where physiological compression is expected to occur) should alert the investigator to the possibility of a lower ureteric stone [19].
Dilation of the pelvicalyceal system alone is non-specific because of the effect of physiological dilation (Fig. 22.4). Left-sided symptoms and dilation have a higher correlation with stone disease because physiological dilation preferentially affects the right side. Renal pelvic diameter of 17 mm or less on an asymptomatic side effectively excludes the presence of stone.

Fig. 22.4
Longitudinal ultrasound image of a kidney showing quite marked pelvicalyceal dilation. This finding alone does not allow the distinction of physiological dilation of pregnancy from obstruction due to ureteric stone
Stones may be seen with ultrasound because of the focus of reflection with a posterior echo shadow (Fig. 22.5). Colour Doppler to show the ring-down artefact behind the stone can increase conspicuity (Fig. 22.6).
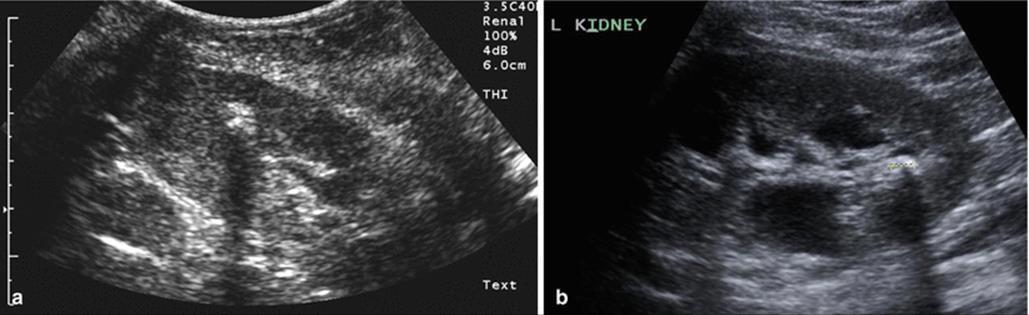
Fig. 22.5
(a, b) Two examples of a renal stone on ultrasound, both demonstrating posterior acoustic shadowing

Fig. 22.6
Axial greyscale ultrasound image of the bladder at the level of the ureteric orifice (a) showing a calculus impacted at the orifice. Colour Doppler image at the same level (b) showing both the ring-down artefact behind a stone and the ureteric jet phenomenon. The latter showing that the presence of a ureteric jet does not exclude a stone
Indirect signs of the presence of a ureteral stone are a raised resistance index (RI) and an absent ureteric jet. The kidneys that have become obstructed by a stone have a raised intrarenal pressure that affects the blood flow through the kidney. This does not occur with physiological dilation. An RI over 0.70 or a difference in RI between the two kidneys of greater than 10 % correlates with the presence of a ureteral stone (Fig. 22.7). Limitations on RI are the confounding factors of prior renal disease, treatment with nonsteroidal anti-inflammatory drugs and scanning within 6 h of the onset of obstruction or more than 48 h after obstruction.
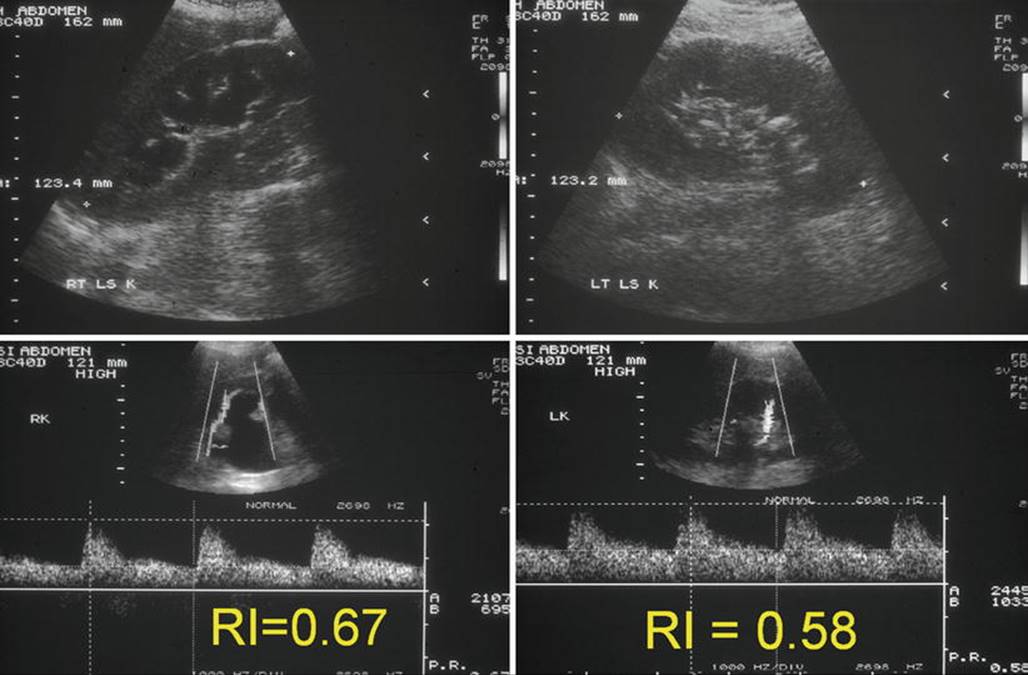
Fig. 22.7
Composite set of ultrasound images of both kidneys showing greyscale appearances and the interlobar artery spectral traces. The right kidney is hydronephrotic. There is a stone in the left kidney. The resistive index in the right kidney is greater than 10 % higher than the contralateral kidney implying that the right-sided dilation is due to a ureteric calculus
Unilateral absence of a ureteral jet into the bladder on the symptomatic side, as shown by colour Doppler, correlates with obstruction (Figs. 22.6 and 22.8). Care must be taken to image the woman in the opposite decubitus position to avoid compression of the ureter by the uterus [20, 21].

Fig. 22.8
Axial ultrasound image through the ureteric orifices. A ureteric jet is seen on the left but none on the right. The orifices should be observed together for a few minutes and the number of jets counted from both sides. A large discrepancy implies ureteric obstruction on the side with the smaller number. The circle shows the right ureteric orifice and highlights the lack of ureteric jet
Quoted ultrasound sensitivities for stone disease in pregnancy vary widely and is clearly dependent on operator expertise and the thrust of any research study. Rates vary from about a third to nearly nine out of ten cases.
22.5.2.2 Second-Line Imaging
The question arises, what should be the next step when ultrasound has not answered the clinical problem and the patient is still symptomatic despite conservative treatment? The choices lie between CT, diagnostic ureteroscopy or MR scan.
CT is undoubtedly the best test in the non-pregnant patient for the detection of urinary tract stones. It also offers an overview of the rest of the abdomen and pelvis allowing alternative causes of flank pain to be detected. The contraindication to its use in pregnancy is the radiation dose involved. This is a relative contraindication as with low-dose techniques, the dose to the fetus can be reduced to 4 mGy without losing sensitivity for stones. At this low dose, it is arguable that the risk of radiation to cause either deterministic or stochastic effects (e.g. fetal loss, teratogenicity or childhood leukaemia) is so negligible as to be considered nothing. Many authorities still advocate its use in pregnancy as shown by the compendium of guidelines published by Austin and Frush [22]. It is also recognised that CT skills and scanners are more widespread than MR and that radiologists may have far more experience in interpreting CT than MR in the pregnant patient. However, if the alternative of MR is available, then CT should be considered as the last choice given its use of radiation [23]. Repeating CT scans during pregnancy is also frowned upon because of the cumulative radiation dose.
Ureteroscopy, with or without fluoroscopy, is held by many urologists to be the next investigation step after ultrasound. The advantage is the ability to combine diagnosis with treatment [24]. General anaesthesia is used in up to two thirds of cases. It is possible to place a ureteric stent or to perform pneumatic lithotripsy with some authors reporting 100 % stone-free rates after treatment [25, 26]. An element of caution is needed as although the maternal and fetal risks are low, they are not non-existent. The rate of complications increases, the more procedures are done. One series quotes a 4 % rate of preterm delivery [27]; another describes a case of ureteral perforation [28]. In view of this, it is prudent to maximise the non-invasive imaging information prior to embarking on ureteroscopy.
In an ideal world, if ultrasound and conservative management have failed to solve the problem, then MR should be chosen as the second-line imaging test ahead of CT or ureteroscopy. MR has the advantage of not involving ionising radiation. MR without intravenous gadolinium-based contrast agents is considered a safe technique: the American College of Radiology (ACR) advises that pregnant patients can undergo MRI without risks for the fetus. MR imaging at 1.5 T or lower magnetic field strength has been used to evaluate diseases in pregnancy for over 20 years without any documented harmful effects [29]. The first trimester is generally avoided as it is difficult to establish safety because of active organogenesis. Field strengths higher than 1.5 T have not yet been proven to be safe, but as yet in the relatively short time, 3 T has been in use, there have been no adverse events reported. Theoretical risks of acoustic injury or thermal damage are limited by the manufacturers’ inbuilt limits for each pulse sequence.
Gadolinium-based contrast agents cross the placenta and are excreted by fetal kidneys into the amniotic fluid. These are classified as category C drugs by the Food and Drug Administration (FDA), i.e. animal reproduction studies have shown an adverse effect on the fetus. Well-controlled studies in humans are not available at present, but potential benefits may warrant use of the drug in pregnant women despite potential risks. For this reason, gadolinium should only be administered using the smallest dose of the most stable gadolinium agent (macrocyclic) [30] and preferably within the context of a trial.
Calculi do not themselves generate any signal on MR scan. MR needs there to be a signal generating fluid or tissue around the calculus to enable the calculus to be detected as a signal void (Fig. 22.9). MR is able to detect the secondary signs of ureteric obstruction due to stone by being able to reveal the dilated ureter, the oedema in the kidney and the perinephric fluid caused by obstruction. It has been suggested by some authors that MR can be used to define the level of obstruction, and then a limited CT scan focused on that level used to detect the stone, thereby greatly reducing the radiation dose whilst still maintaining sensitivity for stone [31]. There are clearly logistical difficulties with this approach in being able to proceed to CT straight after the MR scan such that the concept has not been adopted by other centres.
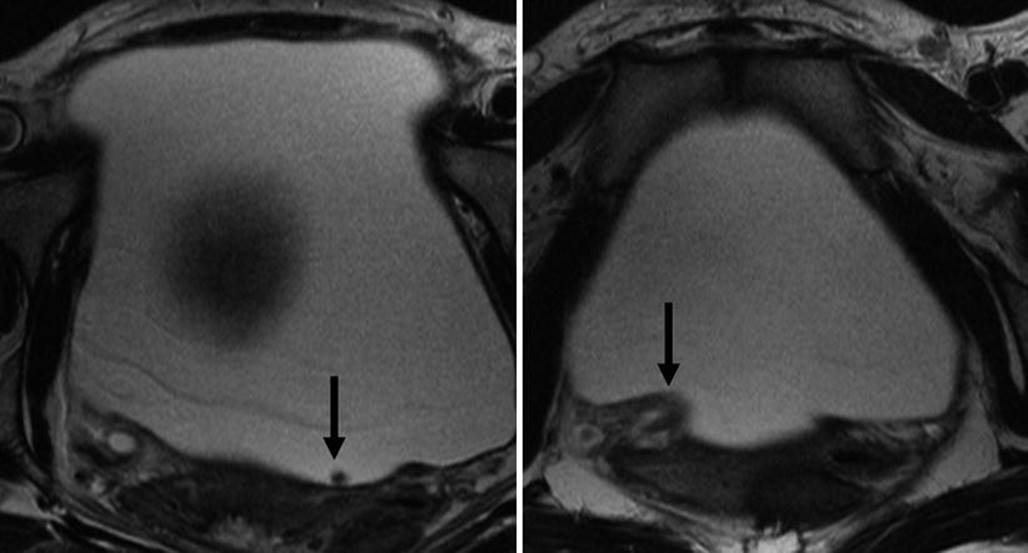
Fig. 22.9
T2-weighted axial images through the bladder. The stone in the bladder (arrow) is revealed as a signal void amongst the high signal of the urine. Note the second arrow points at the oedematous ureteric orifice implying recent passage of the stone
There are only a few published series of the use of MR in pregnancy-related renal colic [32, 33]. None have evaluated sensitivity or specificity for renal calculi. Generally, the larger the calculus, the more likely it is to be detected on MR. Thin-section scans increase the conspicuity of smaller stones (Fig. 22.10). However, the main limitation to high-resolution MR imaging in the pregnant patient is fetal movement. As a consequence, sequences able to generate images in a second or two are preferred with longer acquisitions reserved for imaging the level of obstruction.

Fig. 22.10
High-resolution axial T2-weighted images through the area of concern revealed by thick-slab SSFSE images allow the ureter to be traced (arrows) on sequential images and the stone revealed (on the middle image)
MR can be poorly tolerated by the pregnant patient because of claustrophobia or because of the need to lie in one position. Women in the third trimester often prefer to lie in a partial decubitus position as lying supine can allow the gravid uterus to compress the cava and cause fainting. A careful explanation of the examination and the use of wider bore scanners help to minimise the non-acceptance rate for MR.
Ideally, a radiologist should start by using coronal thick-slab SSFSE ‘MR urography images’ that provide a ‘road map’ of the urinary system (Fig. 22.11) looking for strictures or calibre changes and potential filling defects using fast imaging such as FISP and water-weighted sequences such as SSFSE and then to focus on these areas of interest using higher-resolution T2W imaging. The technique described in early reports using gadolinium as part of MR excretion urography [34] has not been adopted partly because of the unknown effects of gadolinium on the fetus and partly because it offers no advantage over MR urography using the intrinsic contrast available from urine. Showing delayed excretion on the affected side does not increase detection of stones (Fig. 22.12).

Fig. 22.11
(a, b) Two separate examples of thick-slab SSFSE images providing a road map of the urinary tract. In both, the dilated right ureter tapers behind the gravid uterus

Fig. 22.12
Coronal images of the kidneys from MR excretion urography following gadolinium enhancement. Note that the left kidney shows delayed excretion of the gadolinium. This is a sign of ureteric obstruction. However, this feature does not increase sensitivity for obstruction compared to un-enhanced images and because of the unknown effects of gadolinium on the fetus, the technique has fallen into disuse
MR is used to distinguish physiological dilatation of the ureters from an underlying obstructive uropathy.
At MR, physiologic dilatation demonstrates a characteristic tapering due to extrinsic obstruction of the middle third of the ureter from extrinsic compression between the gravid uterus and iliopsoas muscle (Fig 22.13).
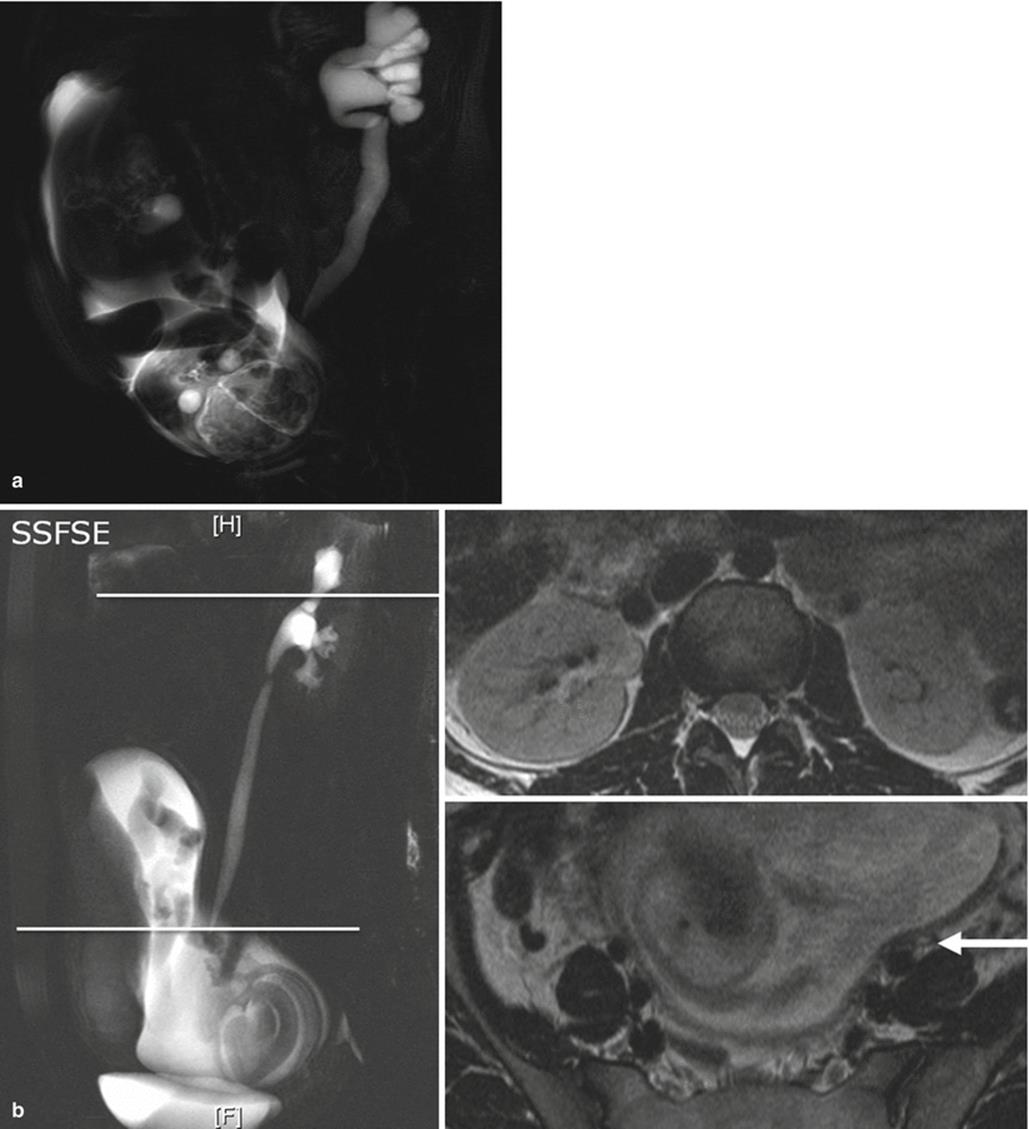
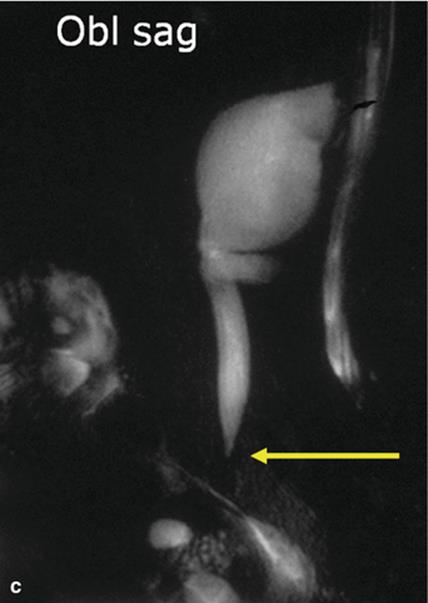
Fig. 22.13
(a) Oblique thick-slab SSFSE helps to confirm that the ureteric obstruction is at the level of the pelvic brim. (b) Composite images from a different patient showing the technique of obtaining axial T2-weighted images at the level of the kidneys and at the point of ureteric calibre change. (c) A further example of the oblique thick-slab SSFSE sequence to confirm that the ureter is not dilated below the pelvic brim. The arrow indicates the compressed ureter
The presence of a standing column of urine below the level of the pelvic brim, in addition to proximal ureteral dilation, suggests an obstructing distal ureteral calculus (‘double kink sign’) (Figs. 22.14 and 22.15) [32]. This is a similar concept to the use of transvaginal ultrasound described above to look for distal ureteric dilation. Other MR features that are indicative of pathologic rather than physiologic hydronephrosis include an ‘unusual’ site of obstruction (such as the pelvic ureteral junction or vesicoureteric junction), an abrupt ending of the ureter (rather than a smooth taper at the level of the pelvic brim), renal enlargement and perinephric or periureteral oedema (Figs. 22.15, 22.16, and 22.17) [32]

Fig. 22.14
Frontal and oblique thick-slab SSFSE views showing how the distal ureteric dilation is hidden on the frontal views but revealed on the oblique view. Arrows indicate the column of urine in the ureter below the usual point of compression behind the uterus
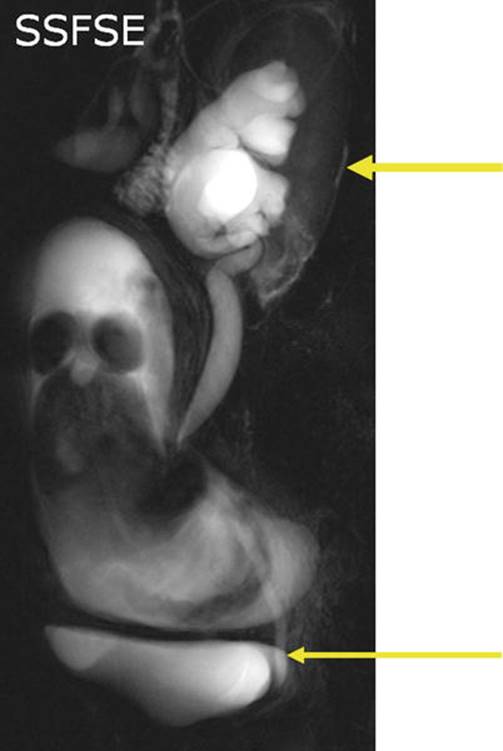
Fig. 22.15
Oblique thick-slab SSFSE showing the distal ureter is dilated beyond the pelvic brim, the so-called double kink sign. It implies a more distal obstruction than physiological dilation of pregnancy, and a stone becomes much more likely. Top arrow indicates the perinephric oedema, bottom arrow shows standing column of urine

Fig. 22.16
Coronal T2-weighted images through both kidneys. The right kidney has a higher cortical signal than the left. This is a feature of cortical oedema secondary to obstruction. The arrowindicates the renal cortex
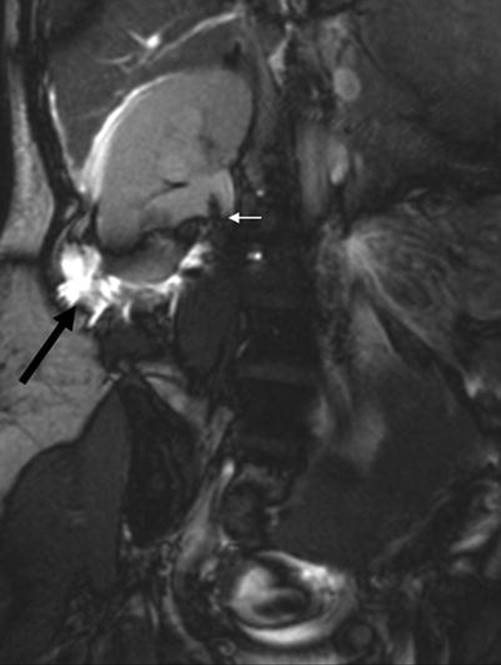
Fig. 22.17
T2-weighted images reveal extravasation of fluid around the kidney; another sign of ureteric obstruction. Black arrow shows perinephric oedema, white arrow shows stone at pelvi-ureteric junction
MR urogram necessitates T2-weighted or water-weighted images, obtained with a two-dimensional single-shot fast spin-echo and balanced gradient-echo sequences. These have the advantage of being motion insensitive and so can be performed even in patients that cannot optimally hold breath. The time acquisition is 1 slice/s, with images in multiple planes.
The T2-weighted sequence based on the half-Fourier reconstruction technique, termed either half-Fourier RARE or single-shot fast spin-echo, allows each image to be obtained in less than 1 s, overcoming or limiting artefacts due to fetal movements. Potential limitations of T2 single shot include spatial mis-registration that may occur between slices if the patient is freely breathing. In addition, T2 single-shot images may develop flow void artefacts in urine within a dilated collecting system that may mimic filling defects. These flow artefacts are typically centrally located and do not layer dependently, as would be expected in a stone within a dilated collecting system.
The detection of acute inflammatory changes is important in the imaging of acute abdominal pain. MRI provides sensitivity for inflammation by demonstration of elevated T2 signal within, or adjacent to, the affected tissues [35]. This elevated abnormal T2 signal might be obscured by the inherent high signal of intraperitoneal and retroperitoneal fat. Thus, the acquisition of an additional T2 single-shot sequence that is combined with reliable fat suppression is important. Fat suppression using a spectral adiabatic inversion recovery (SPAIR) technique has been found to produce improved suppression of lipid signal over conventional inversion recovery or spectral saturation techniques. This SPAIR technique allows the fat-suppressed T2W images to serve as a sensitive marker sequence for oedema and inflammatory changes.
Balanced gradient-echo sequences include free induction echo stimulated acquisition (FIESTA), true fast imaging with steady-state precession (FISP) and balanced steady-state free precession, depending on the manufacturer. These pulse sequences are particularly good for the depiction of larger stones as hypointense filling defects that are surrounded by hyperintense urine, with stone visibility enhanced by distension of the collecting system (Fig. 22.18).

Fig. 22.18
A composite image of MR sequences showing a dilated distal left ureter, oedema of the left renal cortex and (arrowed) the offending stone outlined by urine within the very distal ureter
Balanced steady-state free precession sequences (SSFP) may be acquired with a single-shot technique. Similar to single-shot T2W images, SSFP sequences are also respiratory motion insensitive, with excellent in-plane spatial resolution. SSFP sequences result in high-signal intensity of the fluid-containing structures. One benefit of SSFP sequences is a relative insensitivity to flow-related artefacts present on T2W images, so SSFP is useful as a problem-solving sequence in this scenario. SSFP sequences also produce uniform high-signal intensity in the vascular structures that do not require the administration of intravenous contrast [35].
22.5.3 Management
The majority of ureteric stones in pregnancy will pass spontaneously. Some patients with physiological dilation of the urinary tract will still suffer intractable pain even in the absence of stones. So the need for intervention depends on the symptomatology of the individual patient and not just on the diagnosis of the underlying cause.
Conservative management of physiological dilation involves pain relief and teaching the woman positions to adopt to try to reduce the compressive effect of the gravid uterus on the ureters at the pelvic brim. Some describe a kneeling position with the head lower than the pelvis to promote disimpaction, and others describe lying on the left side to relieve right-sided symptoms.
Standard analgesic treatment, comprising paracetamol and an antispasmodic, is reported to provide symptom relief in 84 % of pregnant women with renal colic [36]. The addition of steroids to those who didn’t respond provided relief to a further 11 % of the total. Others have shown that up to two thirds of confirmed stones will pass spontaneously [8]. Strategies such as this mean that the number of pregnant women requiring intervention during pregnancy is very low. Interestingly, the need for intervention may not correlate with the presence of stone as physiological dilation can cause intractable pain.
The choice of intervention partly depends on local expertise (Fig. 22.19). Ureteroscopy and retrograde stent placement or stone removal is known to be safe [24, 37] with a similar complication profile to the non-pregnant patient. However, some centres may have more ready access to nephrostomy as a temporising procedure. Pyosepsis is an indication to choose nephrostomy as originally described in a paper by van Sonnenberg [38]. Nephrostomy can be inserted entirely under ultrasound control without the need for fluoroscopy.

Fig. 22.19
Fluoroscopic images from a stenting procedure for a ureteric stone in pregnancy. Most ureteroscopists are able to avoid the use of fluoroscopy in pregnancy, restricting its use when passage of wire or scope is not straightforward
22.6 Pre-Existing Conditions
22.6.1 Dilation and Reflux
It must be remembered that not all renal tract dilations found during pregnancy have been caused by the pregnancy. A review of the records and history may reveal pre-existing conditions, such as ureteroceles, duplex kidneys or mega-ureters (Fig. 22.20). Pre-existing reflux nephropathy leads to an increased rate of infection, hypertension, proteinuria and oedema. Renal scarring, in particular when bilateral, produces an increase in maternal complications [39].

Fig. 22.20
Pre-existing conditions may cause increased infection rates in pregnancy. An ultrasound image (a) shows a large cyst in the pelvis. The fetal head is just visible on the edge of the image above this. Review of previous imaging in the form of an MR scan (b, c) shows that the cyst is actually a congenital giant mega-ureter
22.6.2 Cystinuria
Cystinuria is a condition that predisposes to the formation of stones in the renal tract. Standard treatment in the non-pregnant patient involves maintaining a high fluid intake. It has been shown that the same strategy remains effective in the pregnant patient [40].
22.6.3 Angiomyolipoma
Renal angiomyolipoma (AML) is a benign mesenchymal tumour that has a tendency to aneurysm formation that may rupture. The risk of rupture is greater during pregnancy, probably due to effects on oestrogen and progesterone receptors in AML and also the increased maternal circulation and the raised intra-abdominal pressure found in pregnancy. There have been 22 reports of haemorrhaging AML in pregnancy in the last 35 years [41], which have been managed conservatively in eight, with surgery in nine and with embolisation in five. Ultrasound, CT and MR have all been used to make the diagnosis (Fig. 22.21). Ultrasound and MR have the advantage of not using ionising radiation, but CT with intravenous contrast enhancement enables the bleeding point to be identified.

Fig. 22.21
Angiomyolipoma in pregnancy (a) is an ultrasound image showing the typical hyperechoic lesion in the kidney and (b) is an MR scan showing both the gravid uterus and the lesion in the left kidney. This lesion did not suffer any complications
Renal cell carcinoma rarely coexists with pregnancy. Diagnosis is with ultrasound and MR, and primary treatment is still surgical if the tumour is not disseminated [42].
22.6.4 Chronic Renal Disease
Women with chronic renal disease have reduced fertility and, if pregnancy does occur, run increased risks to their own health with deteriorating renal function. There are, furthermore, increased risks of an adverse fetal outcome. Imaging plays little part in the management of these women other than to ensure that the renal dilation of pregnancy is properly recognised and the increased chance of infection and stone formation is detected and treated. As such, the imaging algorithms using ultrasound and MR are the same. Notwithstanding this, there are clearly many issues for women with chronic kidney disease to contemplate when planning a family [43].
22.7 Acute Renal Failure
It is believed that acute renal failure occurs in 1 % of severe pre-eclampsia, 3–15 % of HELLP syndromes (haemolysis, elevated liver enzymes, low platelet count) and 60 % of acute fatty liver of pregnancy [44]. Post-partum haemorrhage in those with HELLP may in particular lead to acute renal failure. Others have shown that the rise in hypertensive disorders of pregnancy is responsible for the increase in obstetric acute renal failure in Canada [45]. The role of imaging is to exclude other causes, primarily postrenal obstruction, and to aid in biopsy if needed. Ultrasound is the mainstay.
22.8 Conclusion
Imaging the maternal kidneys during pregnancy is primarily related to detecting causes of flank pain and to distinguish between physiological dilation of pregnancy and ureteric stones. Ultrasound is the first imaging step, which coupled with effective conservative treatment will resolve the great majority of cases. When this strategy fails, then MR scan is the imaging test of choice to enable a diagnosis to be made and a decision made on the need to proceed to more invasive treatment. If MR is not available, then ureteroscopy is a safe alternative with the benefit of also allowing treatment. CT is reserved as a test of last choice because of the (albeit small) radiation dose. CT does have merits when the cause of the symptoms may not be confined to the renal tract. The radiation dose needs to be kept as low as possible.
References
1.
Conrad KP, Lindheimer MD (1999) Renal and cardiovascular alterations. In: Lindheimer MD, Roberts JM, Cunningham FG (eds) Chesley’s hypertensive disorders in pregnancy, 2nd edn. Appleton and Lange, Stamford, pp 263–326
2.
Ross AE, Handa S, Lingeman JE, Matlaga BR (2008) Kidney stones during pregnancy: an investigation into stone composition. Urol Res 36:99–102CrossRefPubMed
3.
Meria P, Members of the French Urological Association Urolithiasis Committee (2010) Stone formation and pregnancy: pathophysiological insights gained from morphoconstitutional stone analysis. J Urol 183:1412–1416CrossRefPubMed
4.
Riley JM, Dudley AG, Semins MJ (2014) Nephrolithiasis and pregnancy: has the incidence been rising? J Endourol 28:383–386CrossRefPubMed
5.
Srirangam SJ, Hickerton B, Van Cleynenbreugel B (2008) Management of urinary calculi in pregnancy: a review. J Endourol 22:867–875CrossRefPubMed
6.
Andreoiu M, MacMahon R (2009) Renal colic in pregnancy: lithiasis or physiological hydronephrosis. Urology 74:757–761CrossRefPubMed
7.
Lewis DF, Robichaux AG 3rd, Jaekle RK, Marcum NG, Stedman CM (2003) Urolithiasis in pregnancy. Diagnosis, management and pregnancy outcome. J Reprod Med 48:28–32PubMed
8.
Parulkar BG, Hopkins TB, Wollin MR, Howard PJ JR, Lal A (1998) Renal colic during pregnancy: a case for conservative treatment. J Urol 159:365–368CrossRefPubMed
9.
Rosenberg E, Sergienko R, Abu-Ghanem S et al (2011) Nephrolithiasis during pregnancy: characteristics, complications and pregnancy outcome. World J Urol 29:743–747CrossRefPubMed
10.
Banhidy F, Acs N, Puho EH, Czeizel AE (2007) Maternal kidney stones during pregnancy and adverse birth outcomes, particularly congenital abnormalities in the offspring. Arch Gynecol Obstet 275:481–487CrossRefPubMed
11.
Swartz MA, Lydon-Rochelle MT, Simon D, Wright JL, Porter MP (2007) Admission for nephrolithiasis in pregnancy and risk of adverse birth outcomes. Obstet Gynecol 109:1099–1104CrossRefPubMed
12.
Fontaine-Poitrineau C, Branchereau J, Rigaud J, Bouchot O, Caroit-Cambazard Y, Glemain P (2014) Renal colic in pregnancy: series of 103 cases. Prog Urol 24:294–300CrossRefPubMed
13.
Burgess KL, Gettman MT, Rangel LJ, Krambeck AE (2011) Diagnosis of urolithiasis and rate of spontaneous passage during pregnancy. J Urol 186:2280–2284CrossRefPubMed
14.
Matuszkiewicz-Rowinska J, Malyszko J, Wieliczko M (2015) Urinary tract infections in pregnancy: old and new unresolved diagnostic and therapeutic problems. Arch Med Sci 11:67–77PubMedCentralCrossRefPubMed
15.
Sujatha R, Nawani M (2014) Prevalence of asymptomatic bacteriuria and its antibacterial susceptibility pattern among pregnant women attending the antenatal clinic at Kanpur, India. J Clin Diagn Res 8:DCO1–DCO3CrossRef
16.
Rathod SB, Kumbhar SS, Nanivadekar A, Aman K (2015) Role of diffusion-weighted MRI in acute pyelonephritis: a prospective study. Acta Radiol 56:244–249CrossRefPubMed
17.
Faletti R, Cassinis MC, Fonio P et al (2013) Diffusion weighted imaging and apparent diffusion coefficient values versus contrast-enhanced MR imaging in the identification and characterisation of acute pyelonephritis. Eur Radiol 23:3501–3508CrossRefPubMed
18.
Watson WJ, Brost BC (2006) Maternal hydronephrosis in pregnancy: poor association with symptoms of flank pain. Am J Perinatol 23:463–466CrossRefPubMed
19.
MacNeily AE, Goldenberg SL, DiSalvo DN, Brown DL, Frates MC, Laoughlin KR (1991) Sonographic visualisation of the ureter in pregnancy. J Urol 146:298–301PubMed
20.
Shokeir AA, Mahran MR, Abdulmaaboud M (2000) Renal colic in pregnant women: role of resistive index. Urology 55:344–347CrossRefPubMed
21.
Pepe F, Pepe P (2013) Color Doppler ultrasound in the diagnosis of obstructive hydronephrosis in the pregnant women. Arch Gynecol Obstet 288:489–493CrossRefPubMed
22.
Austin LM, Frush DP (2011) Compendium of national guidelines for imaging the pregnant patient. AJR Am J Roentgenol 97:W737–W746CrossRef
23.
Semins MJ, Matlaga BR (2013) Management of urolithiasis in pregnancy. Int J Womens Health 5:599–604PubMedCentralPubMed
24.
Ishii H, Aboumarzouk OM, Somani BK (2014) Current status of ureteroscopy for stone disease in pregnancy. Urolithiasis 42:1–7CrossRefPubMed
25.
Abdel-Kader MS, Tamam AA, Elderwy AA et al (2013) Management of symptomatic ureteral calculi during pregnancy: experience of 23 cases. Urol Ann 5:241–244PubMedCentralCrossRefPubMed
26.
Keshvari Shiran M, Darabi Mahboub MR, Rahimi HR, Seyedi A (2013) The evaluation of ureteroscopy and pneumatic lithotripsy results in pregnant women with ureteral calculi. Nephrourol Mon 5:874–878CrossRef
27.
Johnson EB, Krambeck AE, White WM et al (2012) Obstetric complications of ureteroscopy during pregnancy. J Urol 188:151–154CrossRefPubMed
28.
Laing KA, Lam TB, McClinton S, Cohen NP, Traxer O, Somani BK (2012) Outcomes of ureteroscopy for stone disease in pregnancy: results from a systematic review of the literature. Urol Int 89:380–386CrossRefPubMed
29.
DeWilde JP, Rivers AW, Price DL (2005) A review of the current use of magnetic resonance imaging in pregnancy and safety implications for the fetus. Prog Biophys Mol Biol 87:335–353CrossRef
30.
Thomsen HS, Morcos SK, Almen T et al (2013) Nephrogenic systemic fibrosis and gadolinium-based contrast media: updated ESUR Contrast Medium Safety Committee guidelines. Eur Radiol 23:307–318CrossRefPubMed
31.
Blandino A, Minutoli F, Scribano E et al (2004) Combined magnetic resonance urography and targeted helical CT in patients with renal colic: a new approach to reduce delivered dose. J Magn Reson Imaging 20:264–271CrossRefPubMed
32.
Spencer JA, Chalal R, Kelly A, Taylor K, Eardley I, Lloyd SN (2004) Evaluation of painful hydronephrosis in pregnancy: magnetic resonance urographic patterns in physiological dilatation versus calculus obstruction. J Urol 171:256–260CrossRefPubMed
33.
Mullins JK, Semins MJ, Hyams ES, Bohlman ME, Matlaga BR (2012) Half Fourier single-shot turbo spin-echo magnetic resonance urography for the evaluation of suspected renal colic in pregnancy. Urology 79:1252–1255CrossRefPubMed
34.
Spencer JA, Tomlinson AJ, Weston MJ, Lloyd SN (2000) Early report: comparison of breath hold excretory urography, Doppler ultrasound and isotope renography in evaluation of symptomatic hydronephrosis of pregnancy. Clin Radiol 55:446–453CrossRefPubMed
35.
Kalb B, Sharma P, Salman K, Ogan K, Pattaras JG, Martin DR (2010) Acute abdominal pain: is there a potential role for MRI in the setting of the emergency department in a patient with renal calculi? J Magn Reson Imaging 32:1012–1023CrossRefPubMed
36.
Guichard G, Fromajoux C, Cellarier D et al (2008) Management of renal colic in pregnant women, based on a series of 48 cases [article in French]. Prog Urol 18:29–34CrossRefPubMed
37.
Bozkurt Y, Soylemez H, Atar M et al (2013) Effectiveness and safety of ureteroscopy in pregnant women: a comparative study. Urolithiasis 41:37–42CrossRefPubMed
38.
Van Sonnenberg E, Casola G, Talner LB, Wittich GR, Varney RR, D’Agostino HB (1992) Symptomatic renal obstruction or urosepsis during pregnancy: treatment by sonographically guided percutaneous nephrostomy. AJR Am J Roentgenol 158:91–94CrossRef
39.
El-Khatib M, Packham DK, Becker GJ, Kincaid-Smith P (1994) Pregnancy related complications in women with reflux nephropathy. Clin Nephrol 41:50–55PubMed
40.
Gregory MC, Mansell MA (1983) Pregnancy and cystinuria. Lancet 2(8360):1158–1160CrossRefPubMed
41.
Preece P, Mees B, Norris B, Christie M, Wagner T, Dundee P (2015) Surgical management of haemorrhaging renal angiomyolipoma in pregnancy. Int J Surg Case Rep 7:89–92PubMedCentralCrossRef
42.
Boussios S, Pavlidis N (2014) Renal cell carcinoma in pregnancy: a rare coexistence. Clin Transl Oncol 16:122–127CrossRefPubMed
43.
Tong A, Jesudason S, Craig JC, Winkelmayer WC (2015) Perspectives on pregnancy in women with chronic kidney disease: systematic review of qualitative studies. Nephrol Dial Transplant 30:652–661CrossRefPubMed
44.
Jonard M, Ducloy-Bouthors AS, Boyle E et al (2014) Postpartum acute renal failure: a multicenter study of risk factors in patients admitted to ICU. Ann Intensive Care 4:36PubMedCentralCrossRefPubMed
45.
Mehrabadi A, Liu S, Bartholomew S et al (2014) Hypertensive disorders of pregnancy and the recent increase in obstetric acute renal failure in Canada: population based retrospective cohort study. BMJ 349:g4731PubMedCentralCrossRefPubMed