Paul Lyons1
(1)
Department of Family Medicine, University of California, Riverside, Riverside, CA, USA
Key Points
1.
2.
3.
4.
Background
Multiple independent factors impact the course and outcome of pregnancy. Figure 2.1 represents a schematic diagram of many of these factors and their interrelationship during the course of pregnancy. Prior to conception, a number of factors combine to provide the background environment in which subsequent pregnancies will develop. In particular, a complex interaction between the patient-related factors and environmentally related factors contribute to the likelihood of pregnancy, the prenatal course, pregnancy outcomes, and postpartum complications.
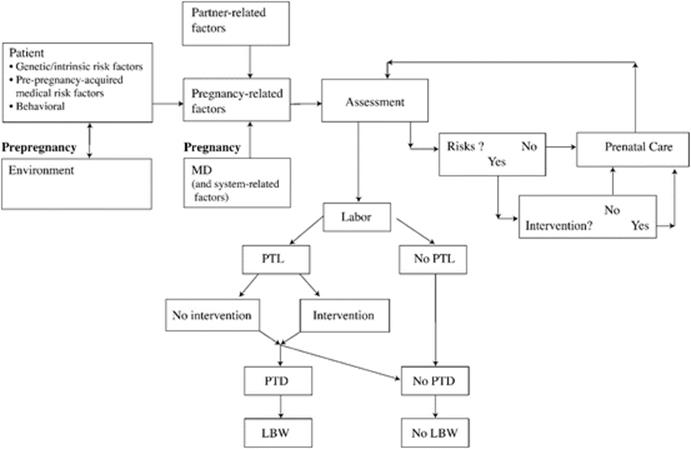
Fig. 2.1
Pregnancy outline
The Patient
Any woman who becomes pregnant brings with her a variety of genetic and acquired factors that have the potential to impact the course of pregnancy. Genetic predisposition plays a significant role in obvious ways (e.g., sickle cell trait, Tay–Sachs, cystic fibrosis) or in more subtle manners (e.g., polymorphic tumor necrosis factor-α which may contribute to a predisposition to preterm labor). Anatomic factors may also contribute (e.g., congenital cervical incompetence, anomalous uterus). Physiological considerations such as the function of the hypothalamic–pituitary–ovarian axis (e.g., oligomenorrhea, anovulatory cycles) also play a role in becoming pregnant and in maintaining pregnancy.
Pregnancy is one potential medical event in the life of a woman, but it is by no means the only one. In addition to the genetic, anatomic, and physiological factors, many women will also acquire medical conditions that may impact the course or outcome of pregnancy. Such conditions as diabetes mellitus, hypertension, and cardiac, renal, or thyroid disease all impact the course of subsequent pregnancies. Not only do underlying disease conditions have the potential to directly impact obstetrical outcomes, many of the medications and treatments for these conditions may also have obstetrical implications. Surgical interventions involving cervical, pelvic, or intra-abdominal manipulation may also have consequences in pregnancy.
A variety of behavioral issues have direct bearing on pregnancy. Nutritional status is critical and has been the focus of recent recommended interventions such as folate supplementation prior to pregnancy. Much work has focused on the detrimental effects that tobacco, alcohol, and other drug use may have during pregnancy. Intrauterine growth rates, congenital anomalies, infant addiction, and preterm complications—among others—have all been shown to be impacted by the use of these substances. Patient exercise, fitness, and activity levels may also contribute to pregnancy outcomes.
The Environment
Although potentially less obvious, the environment in which the woman lives may contribute significantly to obstetrical outcomes. For example, lower socioeconomic status is associated with higher complication rates and/or less good outcomes in a variety of obstetrical conditions such as preterm labor, pregnancy-induced hypertension, and others. Family and partner support for the pregnancy may impact the degree to which women access care during pregnancy.
All of these factors are present prior to conception providing the biopsychosocial environment in which the pregnancy will occur. Because these factors are all present—potentially identifiable and potentially modifiable—prior to conception, it is helpful to consider pregnancy and prenatal care as beginning prior to conception as well.
Preconception counseling is medical evaluation and intervention performed prior to conception with the expectation that the course and outcome of subsequent pregnancies will be improved. Preconception counseling offers providers an opportunity to assess, document, and potentially alter many of the factors that influence pregnancy outcome. Many patients will present to their provider only after discovering they are pregnant. Under such circumstances, the opportunity to impact this potentially critical period is lost. For this reason, preconception counseling is of paramount importance for all providers who care for women of childbearing age. Prior to pregnancy, some women will only seek care for other medical problems. Preconception counseling and intervention, therefore, may need to occur only in the context of care for other medical conditions.
Getting Started
Some women may raise the issue of planning for pregnancy providing the opportunity for the provider to begin the preconception assessment. For these women, providers can begin the process of risk identification/assessment, patient education, and risk intervention/reduction (when possible). Other women, however, may benefit from prompting by their provider. There are a number of ways in which to approach the issue and each provider will determine for him or herself the approach that works best. Because preconception counseling will often be initiated during visits for nonobstetrical care, providers should be prepared to raise the issue in these contexts. A review of menstrual history as part of a routine exam might be followed by open-ended questioning such as “Tell me about any plans you might have to become pregnant.” Visits for chronic medical conditions might lead providers to raise the issue of “the impact of this condition should you choose to become pregnant.” Routine gynecological visits provide another opportunity for beginning prepregnancy planning. Visits related to unprotected sex (sexually transmitted disease screening, late menses, pregnancy testing, etc.) provide an excellent and natural opportunity to discuss issues of importance prior to pregnancy. An often underutilized opportunity for preconception counseling is during routine postpartum care. Planning for subsequent pregnancies (or their prevention) can begin while the patient is still in the hospital and continue when she returns for routine outpatient postpartum care.
Screening
As noted in Table 2.1, preconception counseling should include screening for issues related to the patient and to her environment (including occupational, financial, and family-related issues, among others). A variety of standardized prenatal care flow sheets exist that capture much of this data. Less formal screening may be appropriate under many circumstances. For patients who are seen regularly, screening may occur sequentially over time and should be updated periodically to ensure accuracy.
Table 2.1
Content of preconception counseling
|
Patient-related factors |
|
Psychosocial issues |
|
Tobacco, alcohol, illicit drug use |
|
Psychiatric illness |
|
Literacy/language barriers |
|
Medications |
|
Prescription |
|
Over-the-counter |
|
Herbal, natural, and complementary/alternative therapeutics |
|
Medical |
|
Hypertension |
|
Diabetes |
|
Thyroid disease |
|
Systemic lupus erythematosus |
|
Renal disease |
|
Cardiac disease |
|
Thromboembolic disease |
|
Sickle cell disease (or trait) |
|
Hepatitis |
|
HIV/AIDS |
|
Measles (including immune status) |
|
Varicella (including immune status) |
|
Intra-abdominal or pelvic surgery |
|
Obstetrics/gynecology |
|
Pelvic anomalies |
|
Pelvic inflammatory disease |
|
Prior obstetrical history (all outcomes including full-term, preterm, spontaneous and elective abortions, living children) |
|
Macrosomic infants |
|
Fetal/neonatal death |
|
Genetic (patient, patient’s family and partner) |
|
Down syndrome |
|
Neural tube defects |
|
Cystic fibrosis |
|
Congenital anomalies |
|
Multiple gestation |
|
Environmental factors |
|
Psychosocial issues |
|
Physical/sexual abuse |
|
Partner/family support |
|
Child care |
|
Transportation |
|
Financial support |
|
Insurance status |
|
Occupational issues |
|
High-risk occupations |
|
Occupational exposures |
Education
An appropriate preconception history will allow providers to develop a list of important pregnancy-related concerns prior to conception. This list can form the focus of ongoing education designed to allow patients to make the best possible decisions concerning their health. Modifiable risk factors can be identified and addressed as noted here. For other issues, intervention or modification may be less important than education and discussion of the identified risk factors. Providers of preconception counseling can facilitate their patients’ decisions concerning the desirability and timing of and preparation for pregnancy.
Genetics counseling may be beneficial for those patients at high risk for genetic complications during pregnancy. For patients with chronic medical conditions, the risks of pregnancy, optimal timing for pregnancy, contraception (if pregnancy is medically contraindicated), and prenatal management in the case of pregnancy should all be discussed.
Intervention
A number of important interventions can be offered for women who are not yet pregnant. Patients should be counseled concerning the role of prepregnancy well-being including nutrition, exercise, and fitness. Patients should be counseled concerning the benefits of smoking cessation both for overall health and specifically related to pregnancy. Patients should be made aware of the effects of alcohol and the need to eliminate alcohol consumption prior to becoming pregnant. Use of illicit drugs should also be discouraged.
For those patients who do not plan to become pregnant for at least 1 month, review of the vaccination history may reveal the need for administration of measles mumps rubella (MMR), varicella, and Hep B vaccines. For patients planning to become pregnant in the near future, folic acid supplementation is recommended. For patients with known risk factors (see Table 2.1) for neural tube defects, 4 mg per day is recommended. Because fewer than half of all cases of neural tube defects occur in patients with known risk factors starting prenatal, vitamins and/or folic acid supplementation (0.4 mg per day) should be recommended for all patients prior to conception.
Patients’ medical conditions and medications should be reviewed for potential complications in pregnancy. For patients who take medications contraindicated or relatively contraindicated in pregnancy, providers should discuss the risks and benefits of such medications in pregnancy. Consultation with a maternal–fetal medicine specialist may be beneficial in these circumstances.
Other issues such as language, financial, or family support barriers can be discussed and problem-solving can begin prior to rather than after conception. Patients for whom insurance or financial issues may be an issue should be made aware of insurance programs—available in most states—to provide insurance for pregnant patients.