A 58-year-old man underwent an emergency laparotomy with sigmoid colectomy and colostomy for a perforated diverticulitis 7 days previously. Since the operation, the patient has had intermittent fevers to 39.0°C (102.2°F). He has been unable to eat since the surgery because of persistent abdominal distension. His indwelling urinary catheter was removed 2 days ago, and the patient denies any urinary symptoms. On examination, his temperature is 38.8°C (101.8°F), pulse rate 102 beats/min, and blood pressure 130/80 mm Hg. His skin is warm and moist. The lung examination reveals normal breath sounds in both lung fields, and his heart rate is regular without murmurs. His abdomen is distended and tender throughout, and the surgical incision is open without any evidence of infection. His current medications include maintenance intravenous fluids, morphine sulfate, and intravenous cefoxitin and metronidazole. A complete blood count reveals a white blood cell (WBC) count of 20,500/mm3.
![]() What is the most likely diagnosis?
What is the most likely diagnosis?
![]() What is the next step?
What is the next step?
ANSWERS TO CASE 25: Postoperative Fever (Intra-Abdominal Infection)
Summary: A 58-year-old man has fever and ileus following sigmoid resection and colostomy for a perforated diverticulum. His physical examination does not reveal infection of the respiratory or urinary system or of the surgical site.
• Most likely diagnosis: Intra-abdominal infection.
• Next step: A thorough fever workup including an abdominal and a pelvic computed tomography (CT) scan.
ANALYSIS
Objectives
1. Recognize the sources of fever in postoperative patients and become familiar with strategies for fever evaluation.
2. Learn the principles of diagnosis and treatment of intra-abdominal infections.
3. Learn the pathogenesis of intra-abdominal infections.
Considerations
Persistent fever following definitive operative therapy for an intra-abdominal infection suggests the persistence of infection or the development of another infectious process. It is important to bear in mind that a hospitalized patient may have various sources of fever, including nosocomial infections and noninfectious causes. The possibility of urinary, respiratory, and blood-borne infections should be assessed with urinalysis, chest radiography, and blood cultures. A CT scan of the abdomen and pelvis is a useful diagnostic modality for intra-abdominal infections and is indicated in this setting. When identified, abscesses can be drained percutaneously under CT guidance (Figure 25–1). Inflammatory changes without abscesses are suggestive of persistent secondary peritonitis. Persistent secondary peritonitis may also be caused by inappropriate or inadequate antimicrobial therapy; in these cases, treatment consists of extending the course of therapy or modifying the antimicrobial regimen.
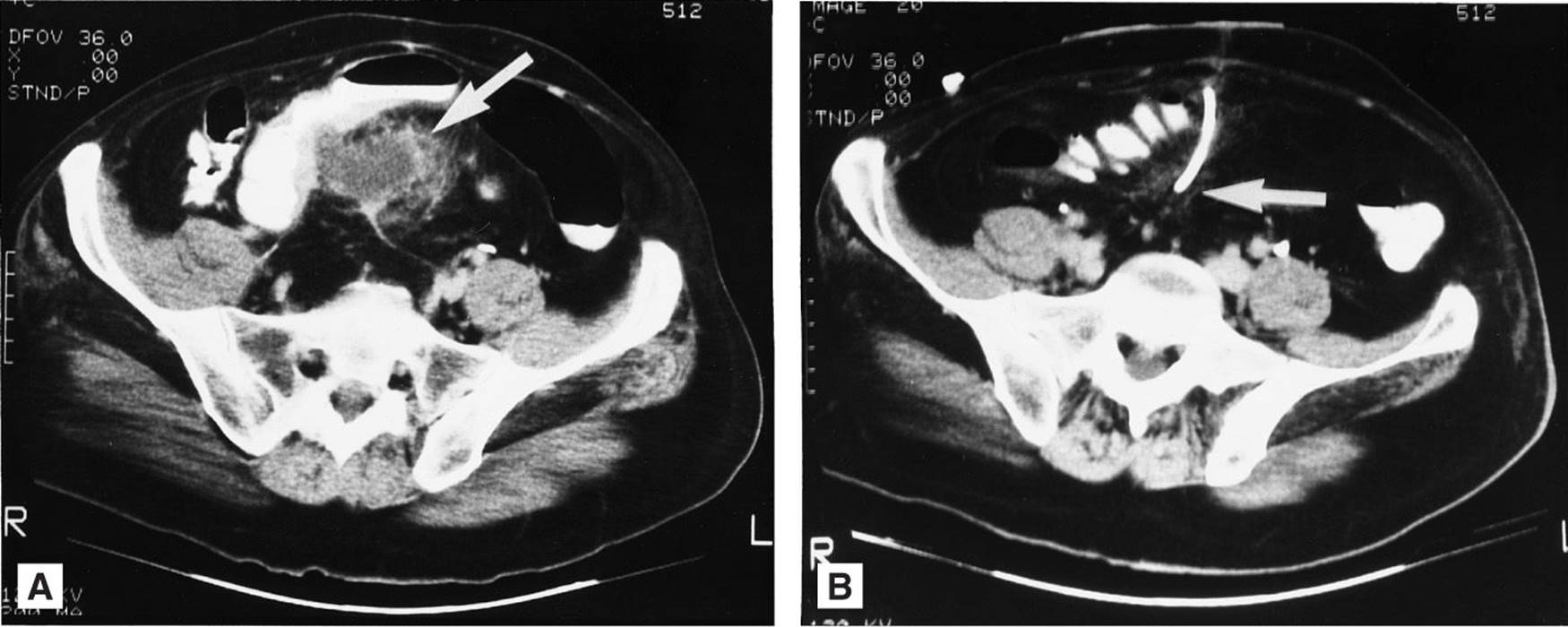
Figure 25–1. Diverticular abscess noted by arrow (A) and then evacuated by computer tomography–guided percutaneous drainage (B). (Reproduced, with permission, from Schwarz SI, Shires GT, Spencer FC, et al, eds. Principles of Surgery. 7th ed. New York, NY: McGraw-Hill; 1999:1041.)
APPROACH TO: Fever and Intra-Abdominal Infection
DEFINITIONS
POSTOPERATIVE FEVER: Fever is arbitrarily defined by most clinicians as oral temperature higher than 38.0°C to 38.5°C (100.4°F-101.3°F).
SURGICAL SITE INFECTIONS: Infections involving the skin and subcutaneous tissue, which are divided into superficial and deep categories depending on whether the fascia is involved. A CT imaging can be helpful when a deep surgical space infection is suspected.
SUPERFICIAL SURGICAL SITE INFECTIONS: Infectious processes above the fascia constitute superficial infections. These are treated primarily by wound exploration and drainage of the infected material, although systemic antibiotic therapy may be needed when there is extensive surrounding cellulitis (>2 cm from the incision margins) or if the patient is immunocompromised.
DEEP SURGICAL SITE INFECTIONS: Infectious processes involving the fascia. The presence of deep surgical site infection mandates an evaluation for possible deep surgical space infection. A CT scan should be considered if deep surgical space infection is suspected.
DEEP SURGICAL SPACE INFECTIONS: Also referred to as intra-abdominal infections in the setting of postoperative abdominal surgery, they include secondary peritonitis, tertiary peritonitis, and intra-abdominal abscesses.
SECONDARY MICROBIAL PERITONITIS: Spillage of endogenous microbes into the peritoneal cavity following viscera perforation. The persistence of this infection is affected by microbial inoculum volume, the inhibitory and synergistic effects of the polymicrobial environment, and host response. Recurrent infections may result from insufficient antimicrobial therapy or inadequate control of the infectious source.
TERTIARY MICROBIAL PERITONITIS: This condition occurs in patients who fail to recover from intra-abdominal infections despite surgical and/or antimicrobial therapy because of diminished host peritoneal response. Frequently, low virulence or opportunistic pathogens such as Staphylococcus epidermidis, Enterococcus faecalis, and Candida species are identified.
INTRA-ABDOMINAL ABSCESS: A defined intraperitoneal collection of inflammatory fluid and microbes resulting from a host compartmentalizing process in which fibrin deposition, omental containment, and ileus of the small bowel localize the infectious material. This response produces loculated, infected inflammatory fluid that cannot be eliminated by the host translymphatic clearance process.
PREEMPTIVE ANTIBIOTIC THERAPY: Administration of antibiotics when a large microbial inoculum is thought to have occurred, such as with a perforated diverticulum with significant peritoneal spillage. Therapy should be directed toward gram-negative aerobes and anaerobes. The optimal therapeutic duration and endpoints are controversial.
SEPSIS: Sepsis is defined as infection plus systemic manifestations of infections (ie, fever, tachycardia, and hyperglycemia). Severe sepsis is defined as sepsis plus sepsis-induced organ dysfunction or tissue hypoperfusion. Septic shock is defined as sepsis-induced hypotension that persists despite adequate fluid resuscitation. The Surviving Sepsis Campaign consists of set of management guidelines for the management of patients with sepsis. These guidelines were initially developed in 2001 and were most recently updated in 2008 with coordination and collaboration by a panel of international experts after careful review of published clinical and basic-science evidence.
CLINICAL APPROACH
Fever that occurs in a hospitalized surgical patient can have a number of causes. These include infections related to the original disease process, such as secondary peritonitis, intra-abdominal abscess, and wound infection. In addition, many hospital-acquired (nosocomial) infections can also occur, including urinary tract infection, pneumonia, bacteremia, intravenous catheter infection, and antibiotic-associated colitis. Noninfectious etiologies include systemic inflammatory response syndrome, endocrinopathies (adrenal insufficiency, thyrotoxicosis), drug reactions, and transfusion reactions. Generally, a febrile postoperative patient who has had abdominal surgery for an infectious process is presumed to have an intra-abdominal infectious complication until proven otherwise.
Pathophysiology of Intra-Abdominal Infections
Perforation of the gastrointestinal (GI) tract results in microbial spillage into the peritoneal cavity. The severity of peritoneal contamination is related to the location of the perforation that determines the concentration and diversity of endogenous microbes (ie, colon contents with 1011-1014 of aerobic and anaerobic microbes per gram of contents versus stomach contents containing 102-103 aerobic microbes per gram of contents). A number of adaptive host responses occur following the inoculation of bacteria into the peritoneal cavity; these include peritoneal macrophage and polymorphonuclear (PMN) (leukocyte) recruitment and the development of ileus and fibropurulent peritonitis to localize the spillage. Normal peritoneal activity includes translymphatic clearance of sequestered microbes and inflammatory cells, leading to the resolution of peritonitis. Several factors influence the resolution or progression of secondary peritonitis: the size of the microbial inoculum; the timing of diagnosis and treatment; the inhibitory, synergistic, or cumulative effects of microbes on the growth of other microbes; and the status of the host peritoneal defenses.
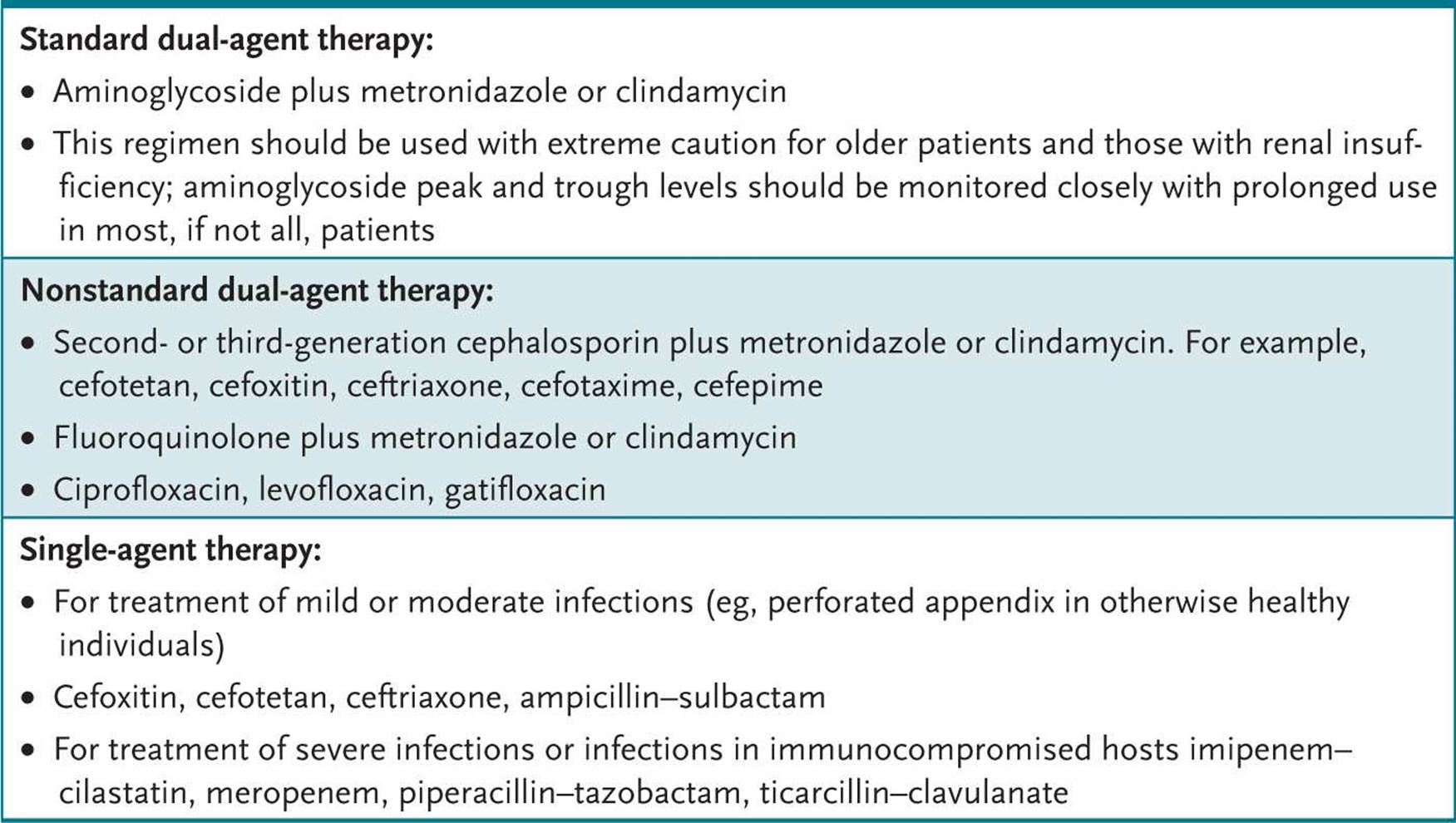
The goals in the management of secondary peritonitis are directed toward eliminating the source of microbial spillage (an appendectomy for a perforated appendix or closure of a perforated duodenal ulcer) and early initiation of preemptive antibiotic therapy. With appropriate therapy, secondary peritonitis resolves in the majority of the patients; however, approximately 15% to 30% of individuals develop complications with recurrent secondary peritonitis, tertiary peritonitis, or intra-abdominal abscesses. Factors contributing to the recurrence of secondary peritonitis include inappropriate and/or insufficient antimicrobial therapy and inadequate source control. Tertiary peritonitis, which is primarily caused by a failure of the host immune response, is treated with additional antimicrobial therapy and optimization of the host condition. Patients with suspected deep surgical space infections following abdominal surgery should undergo CT imaging to search for intra-abdominal abscesses. When identified, abscesses can be treated by percutaneous drainage. Patients with ongoing GI tract spillage or abscesses that are inaccessible by percutaneous drainage should undergo open surgical drainage to control the primary source of infection. Initial systemic antibiotic therapy for the treatment of secondary peritonitis should be directed toward anaerobes and gram-negative aerobes, which can be accomplished with a single broad-spectrum agent or combination therapy (Table 25–1).
Table 25–1 • ANTIMICROBIAL THERAPY FOR INTRA-ABDOMINAL INFECTIONS
COMPREHENSION QUESTIONS
25.1 A 66-year-old woman undergoes exploratory laparotomy for suspected appendicitis. A ruptured appendix with purulent drainage into the peritoneal cavity is noted. Which of the following statements is most correct regarding this patient’s condition?
A. The resulting infection is a difficult problem to resolve even with appropriate surgical and antimicrobial therapy.
B. The most common organisms involved are Candida and Pseudomonas species.
C. Treatment can be effectively accomplished with the use of first-generation cephalosporins.
D. This patient should be sufficiently treated with operative removal of the appendix and the evacuation of intra-abdominal infectious contents.
E. Persistent secondary peritonitis may result from inappropriate antibiotics selection or insufficient duration of therapy.
25.2 Which of the following is most accurate regarding patients who develop fever during the postoperative period?
A. They should receive broad-spectrum antibiotics until the fever resolves.
B. They require no specific therapy because fever is a physiologic response to surgical stress.
C. A thorough search for the fever source is required. Presumptive antibiotics should be given if the patient exhibits physiologic signs of sepsis or if the patient is immunocompromised.
D. The patients should undergo an immediate reoperation.
E. High doses of corticosteroids should be given to blunt the physiological responses to the infection.
25.3 A 39-year-old man undergoes ileal resection and bowel anastomosis because of a perforation related to Crohn disease. Following surgery, he has persistent fever and abdominal pain despite the administration of intravenous cefoxitin and gentamicin. A CT scan reveals a loculated 4- × 5-cm heterogeneous fluid collection in the pelvis. Which of the following is the best therapy for this patient?
A. Add vancomycin to the regimen.
B. Add fluconazole to the regimen.
C. Administer a thrombolytic to dissolve the pelvic hematoma.
D. Drain the fluid collection percutaneously.
E. Perform reexploration of the abdomen.
25.4 Which of the following is the most accurate statement regarding secondary peritonitis?
A. Selection of appropriate antimicrobic regimen always produces successful treatment outcome.
B. Successful treatment cannot be accomplished with antimicrobial therapy alone.
C. Resection of the GI tract source producing the process will always result in the resolution of secondary peritonitis.
D. Antimicrobial therapy is not useful for treatment and would only lead to the selection of resistant organisms.
E. Fungal species are the most common organisms associated with secondary peritonitis.
25.5 A 30-year-old man develops fever, abdominal distension, and leukocytosis 8 days following celiotomy and repair of three separate injuries to the small bowel produced by a gunshot wound to the abdomen. A CT scan reveals a single large fluid collection in the left upper quadrant with extensive surrounding inflammation. This collection is drained by CT-guided drainage and broad-spectrum antibiotic regimen is initiated. Despite these treatments, the patient has persistent fever and drainage of enteric contents from his drainage catheter; in addition, the patient develops drainage of purulent fluid from the inferior portion of his abdominal incision. Which of the following is the most appropriate treatment option?
A. Add empirical treatment to cover for fungal infection.
B. Repeat the CT scan.
C. Perform a celiotomy to address the intestinal leakage site.
D. Assess the patient for immunodeficiency, including skin anergy panel and CD4 cell count measurement.
E. Add a second antibiotic to target pseudomonas
ANSWERS
25.1 E. Inappropriate selection and insufficient duration of antimicrobial therapy are the major causes of persistent secondary peritonitis. Gram-negative and anaerobic bacteria are the most commonly involved bacteria. Appendectomy and drainage are insufficient for the treatment of this patient; systemic antimicrobial therapy must be added to treat the secondary bacterial peritonitis.
25.2 C. Routine antimicrobial therapy is not indicated for all febrile postoperative patients; however, patients with a poor physiologic reserve and a compromised immune system should be treated with broad-spectrum presumptive antimicrobial therapy prior to definitive diagnosis of the fever source. There is no role for high-dose steroids for the purpose of blunting the host response; however, the administration of physiologic doses of corticosteroids has been shown to improve survival and outcomes in patients with septic shock requiring vasoactive agents for hemodynamic support.
25.3 D. This patient likely has an abscess, which is best treated by percutaneous drainage with CT guidance. Reoperation may be needed, if the abscess cannot be drained by a percutaneous approach.
25.4 B. Successful treatment of secondary peritonitis cannot be accomplished by antibiotics alone. Because this form of peritonitis is generally the result of GI perforation such as perforated appendicitis, perforated diverticulitis, and intestinal anastomotic leakage, treatment must include control of leakage source, appropriate selection and duration of antibiotics, and appropriate host immunological response to infections. Fungal species and antibiotic-resistant bacterial organisms are the organisms that are generally recovered from patients with tertiary peritonitis.
25.5 B. Repeating the CT scan at this point may be helpful to determine if there are other collections of infected fluid that may need to be addressed with the placement of additional drains or, if there are multiple collections or inaccessible collections, operative drainage may be needed. The clinical presentation described here suggests that the problem may be inadequate control of leakage rather than inadequate host response. Broadening of antimicrobial coverage may be considered appropriate if additional searches for undrained infectious sources do not provide an answer.
CLINICAL PEARLS
![]() Prolonged dysfunction of the GI tract following GI surgery frequently indicates the presence of intra-abdominal infectious complications, whereas the prompt return of GI function following surgery generally indicates the absence of intra-abdominal infections.
Prolonged dysfunction of the GI tract following GI surgery frequently indicates the presence of intra-abdominal infectious complications, whereas the prompt return of GI function following surgery generally indicates the absence of intra-abdominal infections.
![]() Atelectasis is the most common cause of fever in a patient during the first 24 hours following surgery.
Atelectasis is the most common cause of fever in a patient during the first 24 hours following surgery.
![]() With the availability of many effective antibiotics against gram-negative organisms, aminoglycosides are rarely used as first-line therapy.
With the availability of many effective antibiotics against gram-negative organisms, aminoglycosides are rarely used as first-line therapy.
![]() The colon has a very large number of bacteria (1011-1014 of aerobic and anaerobic microbes per gram of contents) versus the stomach (containing 102-103 aerobic microbes per gram of contents).
The colon has a very large number of bacteria (1011-1014 of aerobic and anaerobic microbes per gram of contents) versus the stomach (containing 102-103 aerobic microbes per gram of contents).
![]() CT imaging is often helpful in identifying intra-abdominal abscesses.
CT imaging is often helpful in identifying intra-abdominal abscesses.
REFERENCES
Arnold MA, Barbul A. Surgical site infections. In: Cameron JL, ed. Current Surgical Therapy. 9th ed. Philadelphia, PA: Mosby Elsevier; 2008:1152-1160.
Beilman GJ, Dunn DL. Surgical infections. In: Brunicardi FC, Andersen DK, Billiar TR, et al, eds. Schwartz’s Principles of Surgery. 9th ed. New York, NY: McGraw-Hill; 2010:113-133.
Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Intensive Care Med. 2008;34:17-60.
Nenshi R, Marshall JC. Intraabdominal infections. In: Cameron JL, ed. Current Surgical Therapy. 9th ed. Philadelphia, PA: Mosby Elsevier; 2008:1160-1163.