Jonathan F. Finks
Presentation
A 55-year-old otherwise healthy, mildly obese (body mass index 33) woman is referred for evaluation of refractory heartburn and regurgitation. Her symptoms have been present for approximately 10 years. She initially attempted lifestyle changes, including cessation of smoking and caffeine use, as well as weight loss, but did not have significant relief. Her symptoms have improved with use of twice daily proton pump inhibitors (PPIs), but she continues to have breakthrough symptoms, especially after eating and when lying down.
Differential Diagnosis
The leading diagnosis based on these symptoms is gastroesophageal reflux disease (GERD). An important consideration is whether or not there is an accompanying hiatal hernia, as this can influence the choice of treatment. The differential diagnosis also includes achalasia. Patients with achalasia most often present with dysphagia, but they will occasionally present with complaints of regurgitation and heartburn. In the case of achalasia, heartburn occurs several hours after eating and usually results from fermentation of undigested food within the esophagus. Certain “alarm” symptoms, including dysphagia, odynophagia, weight loss, anemia, and gastrointestinal bleeding, should prompt a search for esophagogastric malignancy.
Workup
For patients with classic symptoms (heartburn and regurgitation), a good therapeutic response to a trial of PPI therapy is diagnostic of GERD. Further workup is indicated, however, in patients over 50, those with frequent breakthrough symptoms or whose symptoms have persisted for over 5 years, and those with alarm symptoms as mentioned above.
For patients with dysphagia, a barium swallow is a good first study, as it allows for assessment of esophageal strictures (benign and malignant) and diverticula. Furthermore, the barium swallow provides a detailed view of the anatomic relationships of the stomach, esophagus, and diaphragm, allowing for identification of hiatal hernias (Figure 1). A barium swallow is also a good confirmatory study for patients with manometric evidence of achalasia.
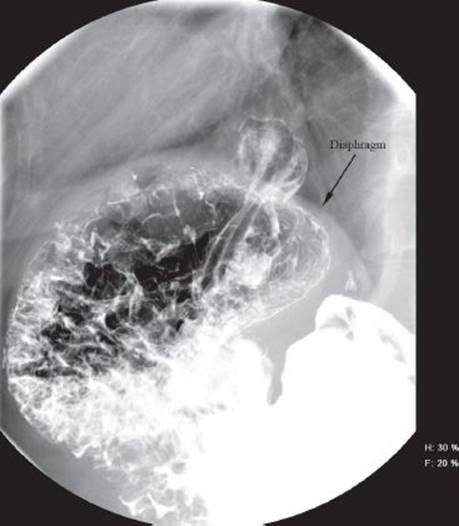
FIGURE 1 • Barium swallow demonstrating a sliding hiatal hernia.
Upper endoscopy offers direct visualization of esophageal mucosa, allowing for identification of esophagitis, Barrett’s esophagus, and esophagogastric malignancies. It is especially useful for patients with atypical, or extraesophageal, symptoms, such as cough, sore throat, and hoarseness, and is indicated in any patient for whom antireflux surgery is considered. The presence of esophagitis on upper endoscopy, in association with typical reflux symptoms (heartburn and regurgitation), is generally considered adequate evidence of reflux disease to justify antireflux surgery.
Ambulatory esophageal pH testing is indicated for patients with atypical symptoms and those with nonerosive disease for whom antireflux surgery is being considered. Generally, this study should be performed with the patient off of any antacid medicine (e.g., PPIs). A more recent alternative is the combined pH and impedance monitor, which allows for detection of both acid and nonacid reflux. This study is particularly useful for patients with persistent symptoms despite the use of maximum medical therapy as well as those with atypical symptoms.
Esophageal manometry offers a functional assessment of the lower esophageal sphincter as well as the motility in the body of the esophagus. It is indicated for patients with dysphagia, where malignancy and hiatal hernia have been ruled out by other studies. Most surgeons also consider esophageal manometry essential before antireflux surgery in order to rule out a significant motility disorder, such as achalasia or scleroderma.
Diagnosis and Treatment
The patient from our clinical scenario had classic symptoms of reflux and demonstrated improvement with the use of PPIs. However, because of her age and the duration of symptoms, she underwent an upper endoscopy that demonstrated a small hiatal hernia but no evidence of esophagitis. Ambulatory pH testing demonstrated that the fraction of time with a pH <4 was 8% (upper limit of normal is <4%), and manometry was normal. All of these findings are consistent with GERD.
In patients with refractory symptoms, as the one in the clinical scenario, or in those who do not tolerate PPIs, antireflux surgery is warranted. Although there are a number of endoluminal devices to treat GERD, some of which fire full-thickness plicators to recreate a competent antireflux valve at the gastroesophageal junction, the long-term efficacy of these devices does not appear promising in early clinical trials. Therefore, we focus instead on surgical approaches, specifically laparoscopic Nissen fundoplication.
Surgical Approach
Antireflux surgery involves restoration of the normal anatomic position of the stomach and gastroesophageal junction and recreation of the antireflux valve. There are several key elements to successful antireflux surgery. First, any hiatal hernia must be completely reduced. This process involves an extensive mediastianal dissection to ensure adequate esophageal mobilization. Second, any defect in the diaphragmatic crura must be adequately closed. Third, the fundus should be completely mobilized by division of the short gastric vessels in order to prevent twisting of the wrap, which could lead to dysphagia. Finally, a 2-cm long “floppy” fundoplication is performed around the distal esophagus over a large dilator, also for prevention of dysphagia.
The procedure is performed under general anesthesia with the patient in the split-leg position. Access to the periotoneum is obtained using a closed (Veress) or open (Hasson) technique and pneumoperitoneum is established. We employ a five-port approach with a camera port placed 15 cm below the top of the xiphoid process. The surgeon stands between the patient’s legs using two upper-quadrant ports. The assistant stands to the patient’s left, using a port in the left upper quadrant and operating the laparoscope. A final port is placed in the subxiphoid position for the liver retractor. Once the ports are placed, the patient is put into the reverse Trendelenberg position and a Nathanson retractor is used to elevate the left lateral segment of the liver.
First, the stomach is manually reduced into the abdomen in the event of a hiatal hernia. Then the gastrohepatic ligament is incised with the ultrasonic dissector, beginning in the avascular portion and extending toward the diaphragm in order to expose the right crus (Table 1). We recommend preserving the hepatic branch of the vagus nerve, both to reduce risk for subsequent gallstone formation and also to avoid injury to the accessory left hepatic artery, which can be present in up to 12% of patients (Figure 2). Next, the phrenoesophageal ligament anterior to the esophagus is opened, with care taken to avoid injury to the underlying esophagus and anterior vagus nerve. Blunt dissection is then used to develop a plane between the right crus and the esophagus. This dissection is continued until the decussation of the left and right crura is visualized. Some retroesophageal dissection may be done from the right side during this portion of the procedure. Care should be taken to prevent injury to the posterior vagus nerve and to keep the nerve up with the esophagus during the dissection.
TABLE 1. Key Technical Steps and Potential Pitfalls
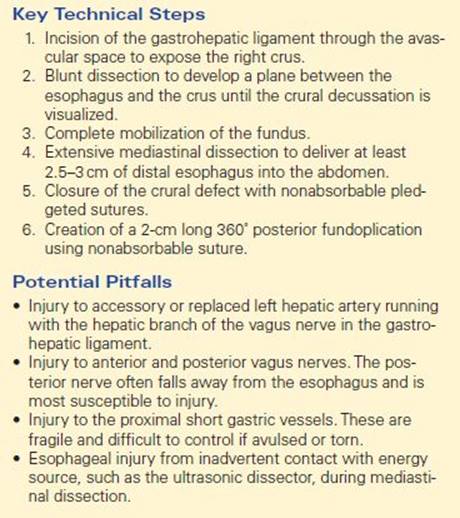
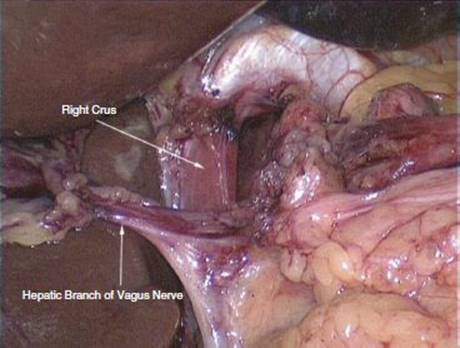
FIGURE 2 • Exposure of the right crus of the diaphragm.
Attention then turns to mobilization of the fundus (Figure 3). The short gastric vessels are divided with the ultrasonic dissector, beginning at the level of the inferior pole of the spleen and extending toward the left crus. The posterior attachments of the stomach should also be divided to ensure full mobilization of the fundus. At this point, the retroesophageal dissection is completed from the left side and a penrose drain is placed around the esophagus, with the ends anchored anteriorly using an endoscopic loop. The penrose drain facilitates retraction of the esophagus.
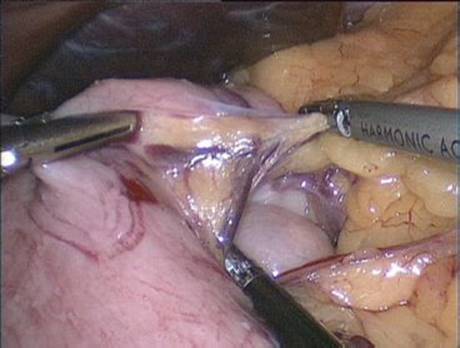
FIGURE 3 • Mobilization of the fundus
What follows is an extensive mediastinal mobilization, using both blunt and ultrasonic dissection to free the esophagus from its mediastinal attachments (Figure 4). This dissection continues until at least 2.5 to 3 cm of distal esophagus remains within the abdomen without having to apply traction to the stomach. Care should be taken to avoid injury to the anterior and posterior vagus nerves during this dissection. The diaphragmatic crura are then reapproximated using nonabsorbable suture secured with felt pledgets to prevent the suture from tearing through the muscle of the diaphragm. The closure should be snug, but not tight, around the esophagus. Calibration with a 56-to 60-French dilator may be helpful during the closure.
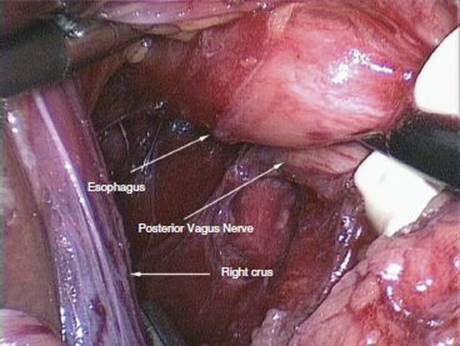
FIGURE 4 • Mediastinal dissection.
The fundus of the stomach is brought behind the esophagus and a 360° fundoplication is then performed over a large dilator (56 to 60 French) (Figure 5). The fundoplication is secured at the right anterolateral aspect of the esophagus with three nonabsorbable sutures. The sutures are placed 1 cm apart, with the most superior suture placed 2 cm above the gastroesophageal junction. Each suture incorporates a full-thickness bite of stomach on either side of the esophagus, as well as a partial thickness bite of esophagus, in order to prevent slippage of the fundus behind the wrap.
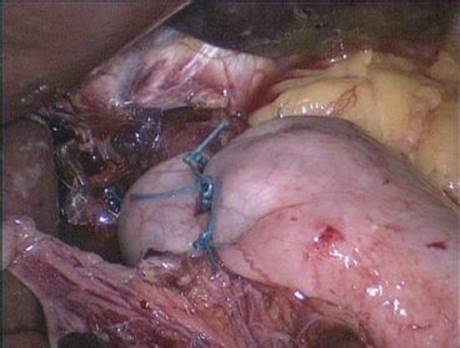
FIGURE 5 • Fundoplication.
Special Intraoperative Considerations
During the mediastinal dissection, especially in the setting of a hiatal hernia, the pleura can be adherent to the hernia sac and is then susceptible to injury. A pleural tear can result in capnothorax with resultant hypercarbia, acidosis, hypoxia, and reduced lung volumes on the affected side. There are typically no lasting consequences, as the gas will absorb rapidly once the pneumoperitoneum has been released. If untreated, however, capnothorax may require conversion to an open procedure. In the event of a pleural tear, there are several steps that will diminish the impact on the patient. First, the tear is enlarged to prevent a tension capnothorax. Next, a 14-French red rubber catheter is inserted into the abdomen. One end of the catheter is then inserted into the pleural space and the other end is left in the abdomen. This will help equalize the pressure between the two cavities. At the end of the procedure, the abdominal end of the catheter is pulled out through the left subcostal port while the pneumoperitoneum is released. The end of the catheter is placed into a water seal while deep Valsalva breaths are administered. This will allow for evacuation of any remaining gas from the affected pleural space. The red rubber catheter is then removed. A postoperative chest x-ray is useful to confirm lung reexpansion.
Postoperative Management
The Foley catheter is typically removed at the end of the procedure. Patients are placed on a scheduled antiemetic, such as ondansetron, for 24 to 48 hours, and may have PRN orders for additional antiemetics, in order to prevent nausea and retching, which can result in disruption of the wrap or early recurrent hiatal hernia. On the first postoperative night or the following day, patients are started on a clear liquid diet and then advanced to a full liquid diet. They are typically discharged on the first or second postoperative day and may advance to a mechanical soft diet within the first week after surgery.
Side effects of antireflux surgery include dysphagia and bloating. Mild dysphagia is not uncommon in the first week or two following the procedure. Because of this problem, patients are advised to avoid tough or dry meat, raw vegetables, and bread for at least 4 to 6 weeks following surgery. In the case of severe dysphagia or dysphagia persisting beyond 6 to 8 weeks, patients should undergo barium swallow to rule out a recurrent hiatal hernia or slipped fundoplication (fundus slipped behind the wrap). If neither of these findings is present, patients should undergo endoscopic dilation. The cause of bloating after antireflux surgery is not clear, but may relate to vagal stretch during the dissection or simply to competence of the wrap which does not permit belching as freely as before surgery. This side effect often resolves after several weeks and can be minimized by avoiding carbonated beverages and eating smaller meals five to six times per day.
TAKE HOME POINTS
· Careful patient selection is essential to success with antireflux surgery. Those selected for surgery should have objective evidence for reflux and symptoms that are attributable to GERD.
· All patients selected for surgery should undergo upper endoscopy and esophageal manometry. Ambulatory 24-hour pH testing should be reserved for patients with nonerosive disease and those with atypical symptoms (e.g., cough, hoarseness).
· Dysphagia is a common complaint following antireflux surgery. The risk for dysphagia can be reduced by full mobilization of the fundus and creation of a “floppy” fundoplication over a 56- to 60-French dilator.
· Recurrent hiatal hernia is the most common cause for failure of antireflux surgery. Adequate crural closure and a thorough mediastinal mobilization of the esophagus, allowing for a minimum of 2.5 to 3 cm of intra-abdominal esophageal length, will help reduce the risk for this complication.
SUGGESTED READINGS
Campos GM, Peters JH, DeMeester TR, et al. Multivariate analysis of factors predicting outcome after laparoscopic Nissen fundoplication. J Gastrointest Surg. 1999;3(3):292–300.
Hunter JG, Trus TL, Branum GD, et al. A physiologic approach to laparoscopic fundoplication for gastroesophageal reflux disease. Ann Surg. 1996;223(6):673–685.
Jobe BA, Kahrilas PJ, Vernon AH, et al. Endoscopic appraisal of the gastroesophageal valve after antireflux surgery. Am J Gastroenterol. 2004;99(2):233–243
Malhi-Chowla N, Gorecki P, Bammer T, et al. Dilation after fundoplication: timing, frequency, indications and outcome. Gastrointest Endosc. 2002;55(2):219–223.