Ralph W. Gilbert
INTRODUCTION
The scapula has been used for maxillary reconstruction and offers several advantages when compared to other reconstructive options. These advantages primarily relate to the chimeric nature of the subscapular vascular system allowing for harvest of multiple, independent skin paddles, serratus muscle with or without rib, latissimus dorsi muscle, and up to 14 cm of lateral scapular bone. This makes it an excellent option for the reconstruction of complex composite defects of the head and neck with large soft tissue requirements. In reconstructing a hemimaxillectomy defect, the advantage of the scapular tip free tissue transfer is the shape of the osseous component of the flap and how it mirrors the shape of the resected maxilla and palate. The primary disadvantage of the traditional scapular flap based on the circumflex scapular artery is the short vascular pedicle, which has led to increasing interest in the scapular tip supplied by the thoracodorsal system of vessels. The tip of the scapular flap is supplied by the angular branch of the thoracodorsal artery rather than the circumflex scapular artery. This design increases the available pedicle length (up to 12 to 14 cm) and allows for the use of the serratus anterior and teres major musculature along with the potential for integrating a latissimus dorsi myocutaneous flap or a thoracodorsal artery perforator flap.
HISTORY
Malignant lesions of the maxilla include adenocarcinoma arising from minor salivary glands, squamous cell carcinoma of the palate, or the maxillary sinus primary osseous malignancies such as osteosarcoma or odontogenic tumors. (Fig. 23.1). Patients may have a visible lesion of the oral cavity with pain, loose dentition, and bleeding. Occasionally, pain and paresthesias may indicate a cancer of the maxillary sinus that is not obvious in the oral cavity. It is important to elicit a history of prior surgery or trauma to the donor site.

FIGURE 23.1 Squamous cell carcinoma of the maxilla requiring hemimaxillectomy and reconstruction.
PHYSICAL EXAMINATION
The physical examination of patients presenting with malignant tumors of the maxilla is relatively straightforward. The extent of the lesion should be evaluated intraorally to determine the size of the lesion and structures involved such as the maxillary alveolus, soft palate, buccal mucosa, and/or pharynx. Evaluation of the patient’s dentition for resection and reconstructive planning is paramount. The donor site must be examined to evaluate for signs of trauma or prior surgery. Flexible fiberoptic examination should be performed to evaluate the involvement of the floor of the nose as well as the nasal cavity and middle meatus.
INDICATIONS
Indications for maxillary reconstruction are listed below. The most common indications are malignant lesions of the maxilla, usually squamous cell carcinoma. Additional malignant or benign lesions are common indications for maxillectomy. Congenital anomalies requiring free tissue transfer are relatively rare.
• Malignant lesions of the maxilla (squamous cell carcinoma [SCCA], cancers of minor salivary gland origin, osteosarcoma)
• Benign lesions of the maxilla (ameloblastoma, giant cell tumors, meningioma)
• Traumatic avulsion/gunshot injuries
• Congenital anomalies
CONTRAINDICATIONS
There are no specific contraindications to maxillary reconstruction with the scapular osteomyogenous free tissue transfer. General medical conditions may prohibit complex reconstructive efforts, and a discussion with the patient regarding the use of an obturator should be undertaken in these cases. The selection of a reconstructive approach versus obturation requires a careful evaluation of the benefits of reconstruction versus the benefits of obturation. In general terms, the more extensive the defect, the more likely I am to recommend reconstruction given the low probability of satisfactory retention of a denture or an obturator. In smaller defects, reconstruction may be considered by patients who have the resources to consider osseointegrated implants for dental rehabilitation. In the rare event that the scapular donor site is contraindicated by previous trauma or surgery, other osseous reconstructive options may be entertained.
PREOPERATIVE PLANNING
The preoperative planning for maxillectomy and reconstruction is relatively standard. Nevertheless, several considerations merit mention.
Anatomy
The circumflex scapular arterial system provides the vascular supply to a number of reconstructive options related to the donor site (Fig. 23.2). The circumflex artery arises from the subscapular artery, which is a branch of the axillary artery in the upper thorax. The scapula and surrounding muscle are supplied by the distal muscular and periosteal branches of the circumflex scapular artery. The cutaneous territories overlying the scapula receive blood supply via the transverse and descending cutaneous branches. The blood supply of the latissimus dorsi muscle is derived from the thoracodorsal artery, which arises from the circumflex scapular artery. Distal angular branches of the thoracodorsal artery supply the tip of scapula, and these form the basis of the scapular tip free tissue transfer.
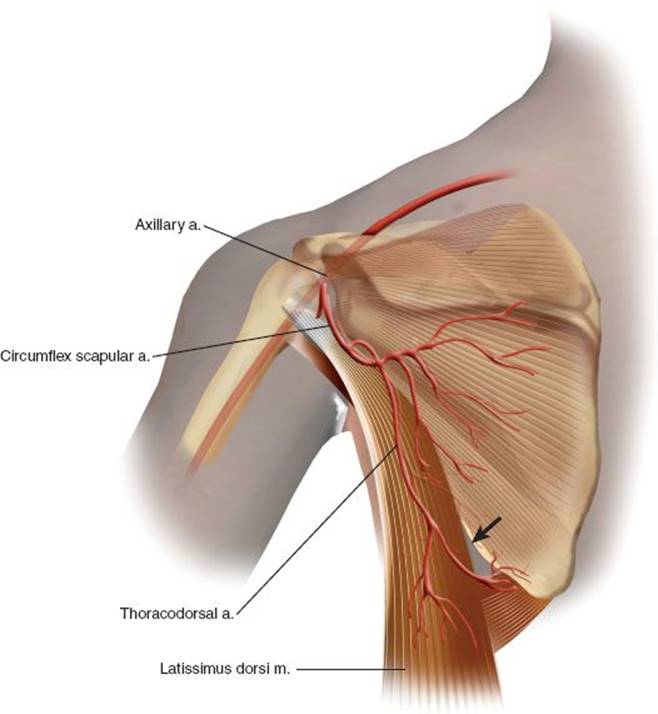
FIGURE 23.2 Anatomy of the subscapular arterial system. The arrow points to the angular branch.
Imaging Studies
The imaging studies required for successful maxillary reconstruction will vary depending on the situation; however, in general, computed tomography with contrast enhancement is relatively standard. The preoperative imaging required is usually driven by the ablative surgical plan, as imaging of the scapular donor site vascular anatomy is unnecessary.
SURGICAL TECHNIQUE
Flap Harvest
The patient is placed on a suction bean bag positioner prior to induction of anesthesia. After induction of anesthesia, the torso is turned approximately 45 degrees and the pelvis to 30 degrees. Access is sufficient when the tip of the scapula can be palpated easily, as shown in Figure 23.3. The contralateral arm is cradled without pressure on the shoulder, and all pressure points are padded. A pillow is placed between the knees and padding placed circumferentially around the feet and ankles. The patient is then secured with straps and wide tape to the operating table so that the table can be rotated without patient movement. Surgical technique starts with the incision design. If there is no plan for harvesting the skin, the incision is placed along the posterior axillary line. The anterior border of latissimus dorsi is identified, and the dorsal surface of the latissimus is mobilized to allow retraction if necessary (Fig. 23.4). Dissection of the pedicle will be anteromedial to latissimus (however, the osteotomies will be performed by retracting it anteriorly).

FIGURE 23.3 Positioning of patient for angular tip of scapular flap (note vacuum bag positioner and taping of patient to prevent movement with rotation).

FIGURE 23.4 Surgical anatomy latissimus muscle is retracted anteriorly demonstrating the teres major muscle and lateral border of the scapula.
The vascular anatomy is then defined. The anterior border of the latissimus is mobilized and the teres major muscle identified. The branches of the thoracodorsal artery to the serratus muscle are identified and followed in an antegrade dissection identifying the branches to the latissimus dorsi muscle. The branching pattern of the circumflex scapular system is somewhat variable, and great care must be taken to avoid dividing individual branches until the entire anatomy and the position of the angular branch is identified. The angular branch usually arises from the thoracodorsal artery although it may also arise from the branch to the serratus muscle or form a trifurcation with these vessels. There is some variability in the distal course of the angular branch, and there may be multiple branches supplying the tip of the scapula as well as the serratus anterior muscle. If a separate branch supplying teres major is identified, it is preserved. If a combination scapula or parascapular cutaneous flap is planned, the proximal pedicle needs to be defined, as the thoracodorsal artery arises directly from the axillary artery in approximately 5% of cases.
The pedicle is fully mobilized before the osteotomies are made to avoid injury to the blood supply. The placement of the osteotomies depends on the desired quantity and contour. The length of bone supplied by the angular branch is approximately 6 cm based on cadaveric injection studies; however, based on our experience, larger amounts of bone may be harvested safely (up to 10 cm). I usually leave a small cuff of serratus anterior muscle anteroinferiorly to protect the angular branch and vary the volume of the teres major cuff dependent on the need for volume filling or revascularization in the maxillary defect. The final dissection of the pedicle of the flap is taken to the circumflex scapular vessels, with assessment of the viability of the flap before division. Serratus anterior, subscapularis, and teres major muscles are reattached to the scapular bone using drill holes and heavy absorbable suture. A large suction drain is used because of the extensive muscle dissection.
Maxillary Reconstruction
The osseous component of the flap can be oriented either horizontally to replace the palatoalveolar complex in infrastructure resections (Fig. 23.5A and B) or vertically to restore the zygomaticomaxillary and nasomaxillary buttress (Fig. 23.6A and B). The muscular component, including the serratus and teres major muscles, can be used as a vascularized covering for the bone (Fig. 23.7). Osteotomies are not generally recommended due to the periosteal blood supply, however “greenstick” fractured segments maintaining the periosteal blood supply, and improve contouring. Fixation is performed using rigid titanium miniplates from 1.5 to 2.0 mm, and the flap is secured to the residual maxilla and zygoma. The floor of the orbit can be reconstructed with additional bone from the donor site when necessary.
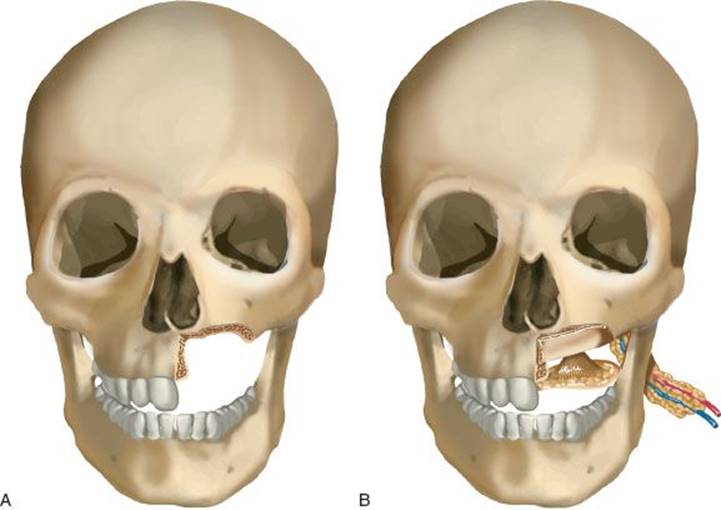
FIGURE 23.5 A. Demonstrates the infrastructure defect. B. Demonstrates the horizontal orientation of the scapula bone graft.
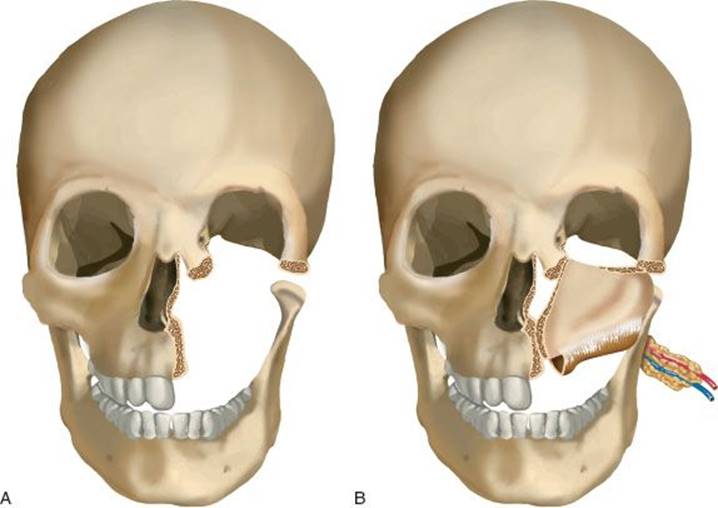
FIGURE 23.6 A. Demonstrates the vertical defect. B. Demonstrates the vertical orientation of the scapula.
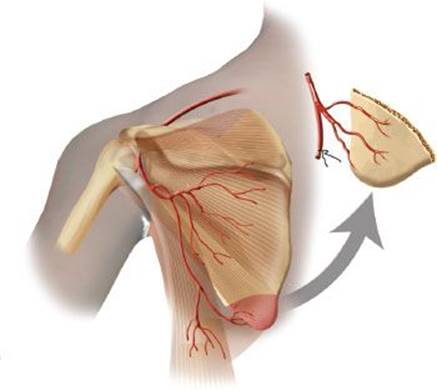
FIGURE 23.7 This illustration demonstrates the vascularization of the scapular tip and the teres muscle. The teres muscle can be harvested with the tip to provide soft tissue coverage of the palatal mucosal defect.
The vascular pedicle is then tunneled through the buccal space deep to the facial nerve and over the mandible. Vascular anastomosis is then performed using a single recipient artery and vein, most commonly the facial artery and vein. Other vessels such as the superficial temporal system or the superior thyroid vessels may be used depending on the length of the pedicle. With the angular modification, vein grafting is not usually required.
POSTOPERATIVE MANAGEMENT
Postoperative management of the patient is relatively straightforward with standard flap monitoring protocols using the Doppler pen, and the external skin paddle if present. For muscle flaps allowed to mucosalize the color of the intraoral component will often appear dark and/or purple, and this is not usually a sign of vascular compromise. The duration of NPO status varies depending on the patient and the reconstruction with longer periods indicated in the setting of preoperative radiotherapy. After 5 to 7 days, a soft diet is generally initiated. Chlorhexidine rinse may be used without detriment to the reconstruction. Nasal obstruction is common postoperatively, and intranasal saline spray may be used for comfort and to prevent crusting.
Regarding the donor site, shoulder movement commences on the first postoperative day, and a shoulder sling is unnecessary. Shoulder abduction exercises are performed daily after discharge. Formal physiotherapy is not required, but patients are advised that shoulder movement may take 6 months for full recovery.
COMPLICATIONS
Complications from maxillary reconstruction with the scapular free tissue transfer include infection, hematoma, and seroma at the donor site. The scapular donor site commonly requires prolonged drainage due to the large muscle surface dissected during harvest. Long-term complications of maxillary reconstruction include malposition of the globe, ectropion, epiphora, palatal fistula, and aesthetic compromise due to inadequate bulk. Palatal fistula after reconstruction with muscle occurs in approximately 15% to 20% of patients; however, the majority close spontaneously, and additional surgical closure is rarely required. Exposure of the hardware occurs rarely and usually after radiation therapy. Preliminary data indicate that significant shoulder dysfunction is rare after scapular harvest; however, patients with previous neck surgery and radiation ipsilateral to the donor site may be at increased risk of shoulder dysfunction.
RESULTS
Patients undergoing reconstruction of the maxilla with the scapular free tissue transfer or other myoosseous flaps usually heal quickly with rehabilitation time dependent on the speed of remucosalization of the palate defect. A hemimaxillectomy may require 4 to 6 weeks to remucosalize; however, the final functional result is far superior to transferred intraoral cutaneous paddles. Most patients prefer oral competence with separation of the nasal cavity using an obturator, and normal diet is usually achieved. Involvement of significant portions of the soft palate commonly results in velopharyngeal insufficiency, which is a characteristic of the ablative procedure rather than the reconstructive technique selected.
The innate shape of the scapular tip offers an excellent option for maxillary reconstruction and allows the goals of maxillary reconstruction to be achieved with minimal donor site morbidity, relatively low complication rates, and excellent functional results.
PEARLS
• The branching pattern of the circumflex scapular system is somewhat variable, and this may alter dissection considerably. The dissection from distal to proximal starting with the serratus branch of the thoracodorsal system will allow the entire vascular territory to be identified prior to harvesting the flap.
• Use “greenstick” osteotomies to maintain the periosteal blood supply when contouring the osseous portion of the flap.
• Vein grafting is not usually required with the angular modification.
• The scapular donor site commonly requires prolonged drainage due to the large surface area involved during harvest.
• Shoulder movement commences from postoperative day one.
PITFALLS
• Prone positioning lengthens the procedure and is unnecessary for scapular harvest.
• Careful attention to recipient vessel length in the neck will avoid unnecessary vein grafting.
• Identify the entire vascular system prior to performing osteotomies to avoid compromising the flap.
• Harvest adequate muscle bulk to cover the osseous transfer and provide closure of the oral cavity defect.
INSTRUMENTS TO HAVE AVAILABLE
• Standard head and neck surgical set
• Reciprocating bone saw
• Titanium plating system (1.5 mm)
SUGGESTED READING
Clark JR, Vesely M, Gilbert R. Scapular angle osteomyogenous flap in postmaxillectomy reconstruction: defect, reconstruction, shoulder function, and harvest technique. Head Neck 2008;30(1):10–20.
Brown J, Bekiroglu F, Shaw R. Indications for the scapular flap in reconstructions of the head and neck. Br J Oral Maxillofac Surg 2010;48(5):331–337.
Dolderer JH, Kelly JL, McCombe D, et al. Maxillofacial osseous reconstruction using the angular branch of the thoracodorsal vessels. J Reconstr Microsurg 2010;26(7):449–454.
Miles BA, Gilbert RW. Maxillary reconstruction with the scapular angle osteomyogenous free flap. Arch Otolaryngol Head Neck Surg 2011;137(11):1130–1135.