Paolo Castelnuovo
INTRODUCTION
The sphenoid sinus has attracted growing attention over the past 10 years. Development of diagnostic techniques and the introduction of selective endonasal endoscopic approaches to the sinus have established the sphenoid sinus as the corridor to sellar and parasellar areas as well as to the middle and posterior cranial base. The sinus borders on many important structures as well as the pterygomaxillary fossa and infratemporal fossa (ITF). Pneumatization of the pterygoid plate (PP) is a known variation of the anatomy of the sphenoid sinus. In the literature, pneumatization of the PP was reported in 25% to 57% of some series. Noticeably, there is a correlation between PP pneumatization and protrusions of both the vidian canal and foramen rotundum (Fig. 7.1).
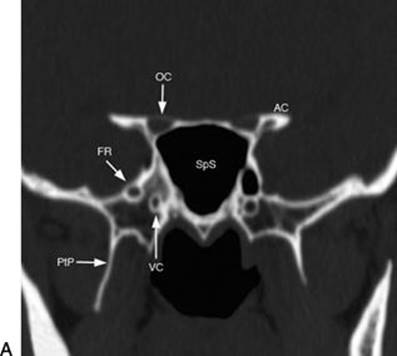
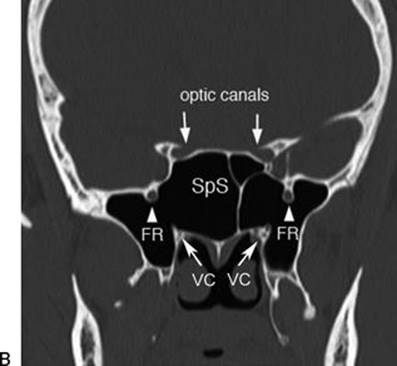
FIGURE 7.1 Radiologic examination of the lateral recess of the sphenoid sinus according to the degree of pneumatization. When the sphenoid sinus is not well pneumatized, (A) the lateral recess is a virtual space, and the vidian nerve and V2 are closely related. In the case of extensive pneumatization of the sphenoid sinus, (B) the lateral recess divides the above-mentioned nerves. (OC, optic canal; AC, internal carotid artery canal; VC, vidian canal; SpS, sphenoid sinus; PtP, pterygoid plate; FR, foramen rotundum.)
The traditional approaches to the sphenoid and its lateral recess (transantral, transpalatal, transfacial, and transcranial approaches) are considered invasive and disfiguring procedures. The development of intranasal endoscopic techniques offered a practical alternative to the traditional methods and direct access to the sphenoid sinus while preserving nearby anatomical structures. Endoscopic endonasal surgery of the middle and posterior cranial base is becoming increasingly refined, and the sphenoid sinus is considered the main anatomical landmark for a variety of approaches.
HISTORY
Isolated diseases of the sphenoid are rare according to the literature. Generally, there are no specific symptoms associated with sphenoid sinus disease. Nasal blockage and/or discharge, especially when unilateral, should always be investigated to exclude benign or malignant tumors with extension to the lateral recess of the sphenoid sinus, involving the pterygopalatine fossa or nasopharynx. Notably, when this symptom is associated with epistaxis in a young male patient, the possibility of juvenile nasopharyngeal angiofibroma (JNA) always has to be taken into account.
Headache is a general symptom that, in certain conditions or associated with other symptoms, can lead to the diagnosis of skull base disease. Often, this kind of headache is located at the vertex or retroorbital and does not respond to conventional treatments.
Watery unilateral nasal secretions could be a warning symptom, especially in a patient with previous episodes of meningitis. In this regard, female sex, postmenopausal age, and obesity are considered as risk factors for spontaneous cerebrospinal fluid (CSF) leaks associated with meningo-/encephaloceles. In these latter cases, the possibility of persistence of Sternberg canal has to be considered. In young patients with previous episodes of meningitis, it is mandatory to exclude a congenital malformation or syndrome even for patients who look phenotypically normal. Lesions of the maxillary or vidian nerves due to compression (fibro-osseous lesions, meningoencephaloceles, inflammatory or benign lesions such as schwannomas) or infiltration (malignancies) may cause numbness of the face and dry eye, respectively.
Invasive or expanding lesions of the sphenoid might destroy the adjacent vital structures. The presence of diplopia could be a sign of involvement of cranial nerve III, IV, or VI. Decreased visual acuity or light perception is an alarming sign of optic nerve involvement.
PHYSICAL EXAMINATION
Nasal endoscopy is now considered an essential diagnostic step in the evaluation of cranial base anatomy and pathology. Endoscopic exploration of the nasal fossa, nasopharynx, and cranial base is necessary for any tissue abnormality or liquorrhea. Watery nasal secretions should always be collected to detect β-2 transferrin protein, for patients with a high suspicion of CSF leak. The traditional neurologic examination of cranial nerves is always included for lesions of the cranial base. The audiometric examination could also be helpful in selected patients with a suspicion of involvement of the petrous apex.
In cases of a cranial base malformation, a thorough evaluation of the head and cranium is necessary. Most of these patients must be evaluated in a multidisciplinary manner with maxillofacial and neurosurgeons. Similarly, careful endocrinologic and neurosurgical assessments are required in case of pituitary pathology to properly plan the minimally invasive and major effective therapeutic option. A multidisciplinary approach is necessary as well for patients with orbital manifestations with screening by an ophthalmologist. Examination of the neck is required to evaluate the presence of lymphadenopathy, especially with malignant lesions of the cranial base.
INDICATIONS
The transpterygoid approach is indicated for accessing pathologies of the lateral recess of the sphenoid sinus or used as a corridor to reach pathologies of the middle cranial fossa (MCF) and posterior cranial fossa. Fibro-osseous lesions, JNA, meningo-encephalocele, schwannoma, and inverted papilloma are some examples of the diseases that can originate from or extend into the lateral recess of the sphenoid sinus. Pathologies of the paramedian–lateral structures of the middle cranial base such as the sella, parasellar area, and lateral portion of the cavernous sinus can be accessed by this approach as well (particularly in case of highly pneumatized lateral recess of the sphenoid).
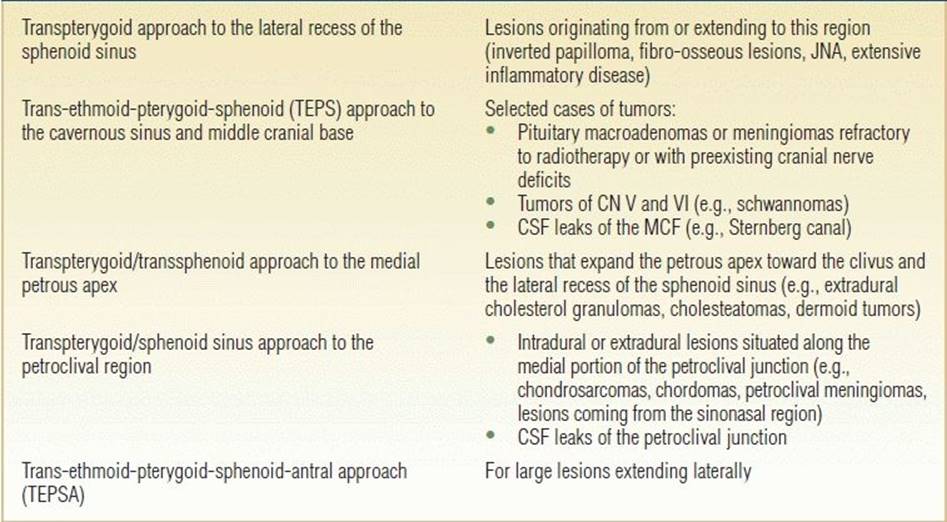
The indications for this approach depend upon the location, type, and consistency of the lesion; they are generally indicated when the neurovascular structures are not involved. Tumors with limited vascular supply and/or that compress and devascularize the cavernous sinus are most favorable for endoscopic resection. Preoperative embolization of hypervascular tumors of the cranial base can be useful. The possibility of this minimally invasive approach for biopsy procedures is particularly advantageous. Furthermore, the transpterygoid approach is indicated as a corridor to target different areas such as the medial petrous apex, infrapetrous region, inferior cavernous sinus, petroclival area, and ITF (Table 7.1).
Table 7.1 Indications for Transpterygoid Approach
CONTRAINDICATIONS
Contraindications for an exclusively endoscopic approach include the encasement of vital vascular structures (internal carotid artery [ICA] or perforating vessels) and the impossibility to treat or remove the lesion through the nasosphenoid corridor, as in the case of a tumor with a hard consistency and pial adherence. A purely endoscopic approach is also contraindicated in cases in which neurovascular surgery (ICA shunting) or orbital exenteration is needed. In these cases, a combined cranioendoscopic approach is preferable.
Nevertheless, the most important contraindication when choosing the type of approach remains the surgeon's insufficient experience in the endoscopic management of these anatomical regions and overall inability to manage complications.
PREOPERATIVE PLANNING
The routine use of nasal endoscopy, CT scans, and MRI has improved the accuracy of the diagnosis of disease of the sphenoid sinus. Endoscopic and radiologic examinations allow for evaluation of the localization, size, and extent of lesions and, in some cases, can provide preoperative diagnosis (e.g., cholesterol granuloma, JNA) without resorting to biopsy. Preoperative endoscopic examination, together with CT scans, provides details on anatomic features (e.g., septal spur, concha bullosa, pneumatization of the sphenoidal rostrum, and pneumatization of the superior turbinate) that can influence the choice of the ideal surgical corridor. Identification of radiologic landmarks such as the vidian nerve, V2, ICA, optic nerve, and pneumatization of the PP is needed to avoid potential surgical hazards.
CT is extremely helpful in delineating the integrity of the bone and the variations of density. The finding of remodeling of the bone or erosion on CT requires careful evaluation of complementary soft tissue details on MRI. MRI plays a prominent role in imaging of the sphenoid sinus and the adjacent structures. Its high-contrast resolution combined with multiplanar capability makes it a valuable tool not only in the evaluation of benign and malignant neoplasms but also in the evaluation of aggressive inflammatory lesions. MRI allows identification of intracavernous structures in extreme detail and perfectly highlighting the intracavernous portion of the cranial nerves. The boundaries of the cavernous sinus, dura, and CSF are well defined. CT and MRI with contrast and angiography are particularly important to determine the consistency of the lesion, which helps to form the differential diagnosis. The imaging also helps to understand the relationship between the lesion and adjacent blood vessels. PET–CT is necessary for staging in malignant lesions prone to regional or distant metastasis.
Tissue biopsy is an essential step of the pretreatment evaluation. However, some pathology can be diagnosed based on clinical and radiologic assessment such as highly vascular lesions and meningo-encephalocele when biopsy is contraindicated. Before planning removal of a lesion, it is important to consider the histology of the tumor to avoid unnecessary surgery.
Early diagnosis is crucial because the presenting symptoms are both delayed and nonspecific, and often, diagnosis is made after the complication arises.
In order to avoid excessive bleeding during surgery, the patient should suspend all anticoagulant drugs and nonsteroidal anti-inflammatory drugs. Infectious sinonasal conditions should be resolved prior to surgery.
The patient must be informed about the possible risks of this operation, the hazards of neurovascular injury, and the possibility of duraplasty and that an external approach might be used as an alternative or complementary procedure. Of course, treatment should be based on multidisciplinary input including an otorhinolaryngologist, neurosurgeon, neurovascular interventionist, maxillofacial surgeon, neuroradiologist, and other related specialists.
SURGICAL TECHNIQUE
The patient should be anesthetized and placed in the supine position. A magnetic neuronavigation system is applied using CT angiography or CT/MRI fusion for better delineation of the vascular structures during dissection. A 0-degree endoscope is used to perform a wide maxillary antrostomy in order to expose the posterior wall of the maxillary sinus. Then, an anteroposterior sphenoethmoidectomy is performed. This approach is a lateral extension of the transethmoidal approach to the medial wall and apex of the orbit, and the base of the pterygoid should be exposed. During this step, attention must be paid to cauterization of the descending palatine artery encountered during posterior enlargement of the maxillary antrostomy toward the PP. Subtotal resection of the middle turbinate with preservation of the superior attachment is required.
The site where both the nasal branch and septal branch of the sphenopalatine artery emerge is identified and electrocoagulated with bipolar forceps. The sphenopalatine foramen is then identified, and the pterygomaxillary fossa is opened with Kerrison forceps. Good lateral vision is obtained using a 45-degree endoscope. By lateralizing the contents of the pterygomaxillary fossa, the vidian foramen and the foramen rotundum can be seen. After electrocoagulation of the vidian artery, the base of the pterygoid and the base of the sphenoid sinus are exposed, especially at the bony margin that links the two ostia (vidian and rotundum). In this manner, it is possible to have a complete view of the pterygoid recess of the sphenoid. In the case of a well-pneumatized PP, the posterior wall of the maxilla can be removed to expose the ITF. Subsequently, the vidian canal has to be well exposed as an important safety landmark for the medial genu of the paraclival ICA (Fig. 7.2).

FIGURE 7.2 Anatomical cadaveric representation of the lateral recess of the sphenoid sinus and the surrounding surgical landmarks that the endoscopist has to recognize. (C, clivus; ICA, internal carotid artery; V2, maxillary nerve; VC, vidian canal; SPA, sphenopalatine artery; lrSS, lateral recess of sphenoid sinus.)
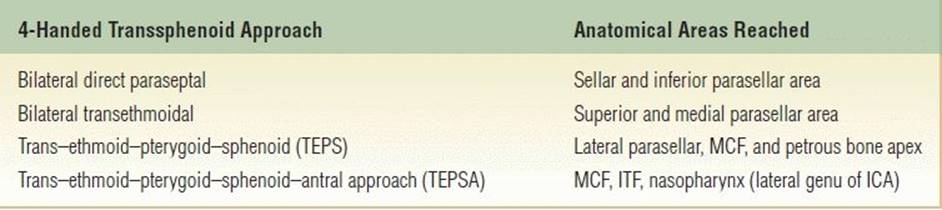
In the four-handed technique (Table 7.2), an ipsilateral approach is considered sufficient for treatment of minor lesions. A contralateral paraseptal approach is performed for medium and large lesions, by removing the intersphenoid septum and sphenoid rostrum. Thereafter, a portion of the vomer is removed to reach the floor of the contralateral MCF and for better accessibility of instruments in case of a four-handed technique. If this approach has to be extended to the ITF, an endoscopic medial maxillectomy is added to gain as much lateral exposure as possible.
Table 7.2 Transsphenoidal Approaches
In the case of a meningo-encephalocele or iatrogenic CSF leak occurring at the level of the MCF, reconstruction of the cranial base with a multilayer technique is necessary. I prefer using autologous materials such as temporalis (or abdominal) fascia, fascia lata, septal or mucoperiosteum of the septum or turbinate, quadrangular cartilage, or turbinate bone although heterologous materials can be used as well. The choice of material depends on the type of surgical approach employed, the location, and the degree of the dural defect. Middle turbinate bone and mucoperiosteum can be used as free grafts. The reconstruction technique depends upon placing the grafts in a multilayer manner (extradural intracranial layer, then an extracranial layer) to guarantee a watertight closure. Another intradural intracranial layer is applied only for large dural defects. In critical areas where neurovascular structures are close by, this technique might be risky to apply. Gasket seal closure gives better results in such situations. The technique is to simply spread a large graft in an overlay fashion. A piece of cartilage that is slightly larger than the defect is introduced over the graft and gently pushed intracranial, while the edges of the graft are kept extracranial to prevent any contact between the graft and adjacent neurovascular structures.
Larger defects require a larger flap such as the nasoseptal flap (Hadad-Bassagasteguy flap). In order to harvest this flap, the surgeon should preserve the septal branches of sphenopalatine artery with section of the arterial branches passing through bony canals (i.e., descending palatine artery, palatovaginal artery, and vidian artery). This allows preservation of the vascular pedicle of the flap and permits more freedom of movement.
At the end of the procedure, fibrin glue should be applied over the grafts/flaps and not between them to avoid creating empty spaces and consequently the possible recurrence of a CSF leak once the glue is absorbed. Some surgeons like to use a balloon stent in the sphenoid sinus as a support for the graft. Silicone sheets are placed paraseptally, and nasal packing is inserted.
Obliteration of the sphenoid sinus, alone or with an overlay graft, has been often used to close defects located in the lateral sphenoidal recess. This option can be used in small sphenoid cavities where accurate removal of mucosa can be obtained, but in the case of well-pneumatized sphenoid sinuses, this might be a burden. In our series, the first seven cases with adipose tissue obliteration did not have a CSF leak recurrence. However, one patient developed pain related to the V2 distribution area. An arachnoid cyst arose under the temporal lobe very close to the bone defect and V2 canal. We have considered this condition (arachnoid cyst formation) a very rare complication of adipose tissue obliteration of the sphenoid sinus. Since then, we have not performed sinus obliteration because the efforts should be directed toward repairing the bony defect in the cranial base, which is not achieved by sinus obliteration alone.
Lumbar drainage is not routinely indicated at the time of surgery unless the patient has signs of intracranial hypertension. In case of preexisting intracranial hypertension, the possibility of placing a ventriculoperitoneal shunt should be considered. Some authors find lumbar drainage helpful during the postoperative course for 5 to 6 days in case they are suspicious of a CSF leak.
POSTOPERATIVE MANAGEMENT
Nasal packing is removed on the first or second postoperative day. Silicone sheets, which are placed paraseptally at the end of the surgery to avoid synechiae and crust formation, are removed two weeks later. Nasal irrigation with mucolytic and saline solution allows for better cleansing of the nasal fossae. During hospitalization, CT scan or MRI is usually carried out 24 hours after surgery to check for any intracranial hemorrhage, ischemia, or pneumocephalus as well as to screen for any gross residual tumor.
Patients should undergo a regular follow-up program according to the pathology. Malignant lesions should have a strict clinical and radiologic screening based on monthly endoscopic examination and MRI every 4 months during the 1st year; endoscopic examination and MRI every 2 and 6 months, respectively, during the 2nd year; and, subsequently, both examinations at 6-month intervals.
During the first follow-up, the surgical cavity should be cleansed of residual crusting, and the state of the flap, if used, should be examined. The presence of infection and macroscopic CSF leak should be sought.
COMPLICATIONS
Risks
· CSF leak
· Internal carotid artery injury
· Cavernous sinus injury
· Orbital apex–optic nerve injury
· Maxillary nerve injury
· Nerve injury V2
· Dry eye (vidian nerve)
A complete understanding of anatomical relationships is a fundamental prerequisite. The basic extra- and intracranial landmarks must be constantly kept under control during surgery to guarantee safe access to deep structures.
When accessing the sphenoid sinus, the surgeon should keep in mind the need to identify the superior border of the choana and the sphenoid rostrum along with the tail of the superior and supreme turbinates. Opening of the cavernous sinus is made after the exposure of the vidian canal and foramen rotundum, recognizing that cranial nerve VI runs freely crossing the cavernous sinus from medial to lateral and inferior to superior direction. While accessing the petrous apex, the medial pterygoid lamina, vidian canal, and medial genu of the ICA must be identified (Fig. 7.3). This is necessary to avoid CSF leak from the posterior cranial fossa and to prevent severe damage to the internal carotid artery or inferior hypophyseal artery. Hemorrhage from the internal carotid artery or major vessels can result in devastating neurologic deficits or death.
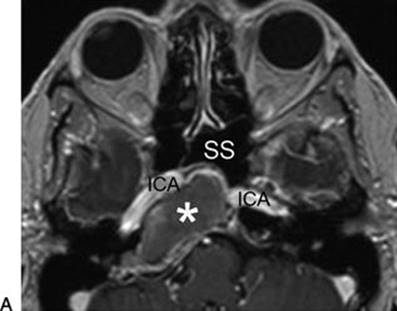
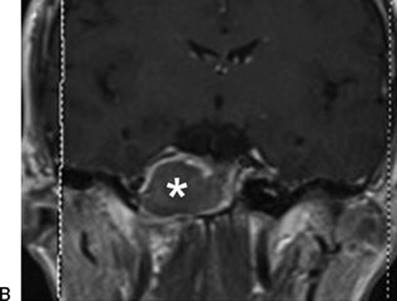
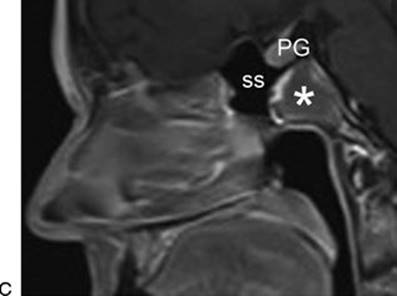
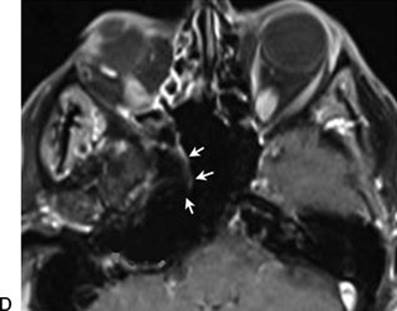
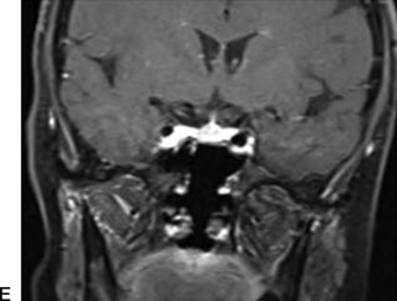
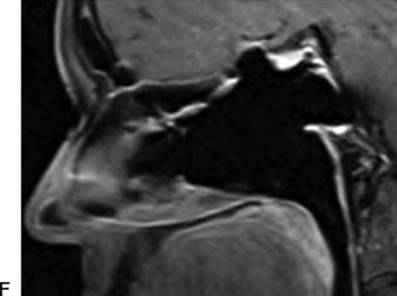
FIGURE 7.3 Huge cholesterol granuloma of the right petrous apex (marked with asterisk). Preoperative MR scan (with contrast enhancement, T1 weighted) in axial (A), coronal (B), and sagittal (C) views is characterized by hyperintensity in the capsule of the lesion. Paraseptal transsphenoidal approach with vidian canal dissection above medial PP, leaving the ethmoid sinus intact, allowed marsupialization of the lesion. Nasoseptal flap was harvested to maintain the patency of the surgical corridor (marked with white arrows). The 2-year follow-up MR scan in axial (D), coronal (E), and sagittal (F) views confirmed good ventilation of the surgical cavity. (PG, pituitary gland; SS, sphenoidal sinus; ICA, internal carotid artery.)
Many reports in the literature show a significant reduction in CSF leak complications with the use of the nasoseptal flap. When this is not feasible, using a temporoparietal flap passed through the pterygopalatine fossa is a reliable alternative. The use of temporary lumbar subarachnoid drainage during the postoperative period does not seem to decrease the rate of recurrence of CSF leak. Generalized epilepsy due to intraoperative massive CSF loss and consequent pneumocephalus has been observed.
Cranial nerves can be damaged either directly or by injury to the vessels supplying them. Temporary or permanent paralysis is possible. We have observed temporary paralysis of CN VI in one case in the absence of direct surgical trauma. This occurred after lavage of the cavernous sinus to facilitate complete removal of a dermoid lesion. Another serious complication is injury to the optic nerve with subsequent mono-binocular blindness. Facial and palatal numbness and dry eye are possible complications when V2 and vidian nerve, respectively, are damaged. Other complications include ascending bacterial meningitis, infections of the paranasal sinuses, postoperative epistaxis, and nasal airway narrowing due to scarring.
A key aspect in surgical training is the acquisition of three-dimensional anatomical knowledge. This basic familiarity should allow the surgeon to achieve intraoperative orientation based on the integration of macroscopic, radiologic, and tactile perception to recreate a complete three-dimensional mental scheme. In this sense, neuronavigation offers an additional advantage to avoid complications but is not a substitute for anatomical knowledge and good surgical technique.
RESULTS
Transsphenoidal endonasal endoscopic approach for solid and cystic lesions of the lateral sphenoid recess is a highly conservative procedure (Fig. 7.4). The results are comparable to those obtained with traditional microscopic transfacial-transcranial approaches (lateral rhinotomy/Caldwell-Luc-midfacial degloving-transtemporal-transcranial lateral approaches). The endonasal endoscopic approach avoids disfiguring facial scarring, risks to the facial nerve, and interference with cochlear and vestibular functions. Furthermore, no external skin incision is required, and it offers less hospitalization and intensive care admission. This minimally invasive approach allows for a larger and more natural corridor through the sinuses, which makes endoscopic postoperative follow-up easier for the detection of recurrences (Fig. 7.5). In addition, the endonasal endoscopic approach provides visual magnification of deeper lesions and the anatomical structures.

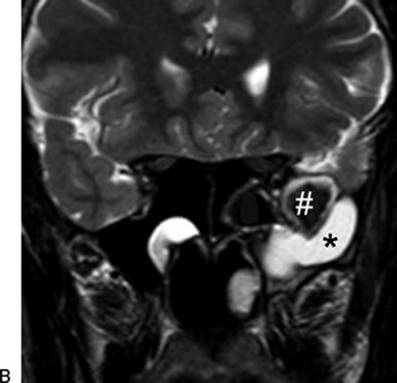
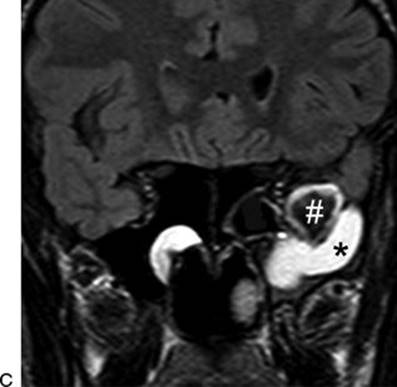
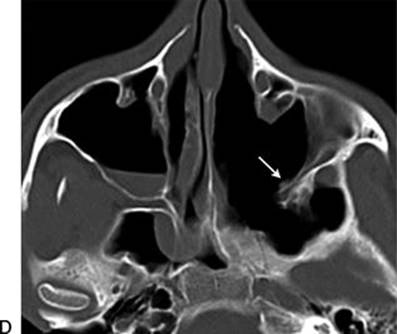
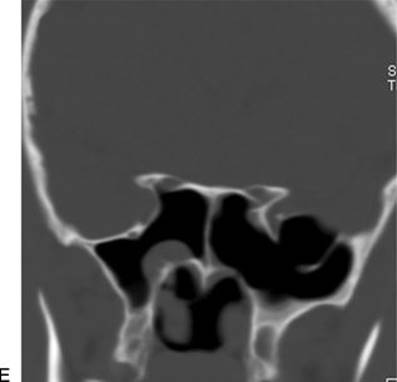
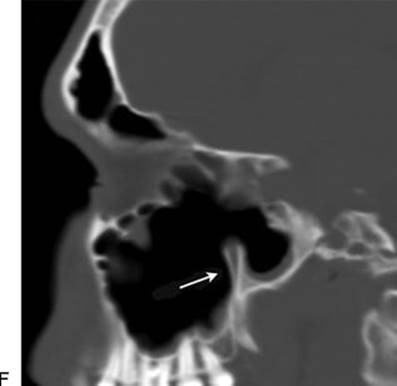
FIGURE 7.4 Left sphenoid sinus fluid lesions with different MR intensities (marked with the symbols asterisk and hash) reflect different fluid/protein content. The hyperintensity on T2-weighted MR scan in axial (A) and coronal (B) views demonstrates the liquid component of the lesion. The maintained hyperintensity on FLAIR-T2 sequence with suppression of CSF signal (in coronal view) (C) is very useful to exclude CSF leaks. The TEPS endoscopic endonasal corridor allows us to reach the fluid lesion localized in the lateral recess of the left sphenoid sinus, up to the cystic lesion in the temporal region that was marsupialized just below V2. Postoperative CT scan in axial (D), coronal (E), and sagittal (F) views. Radiologic identification of the consistency of the lesion allowed us to spare additional transantral approach (the preserved posterior maxillary wall is marked with white arrows).
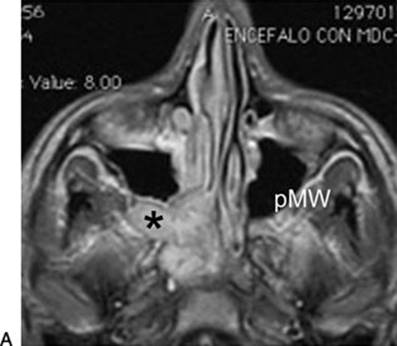
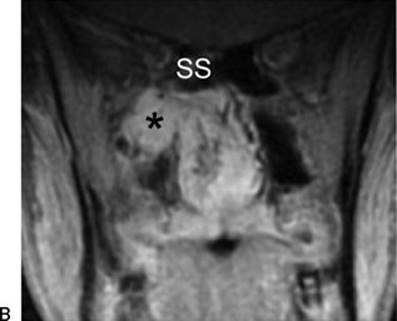
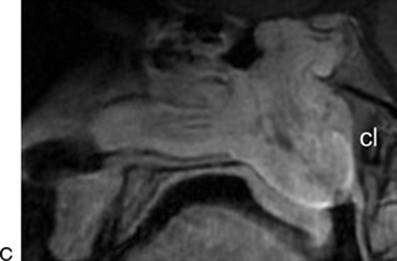
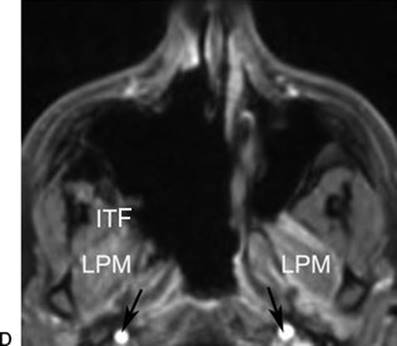
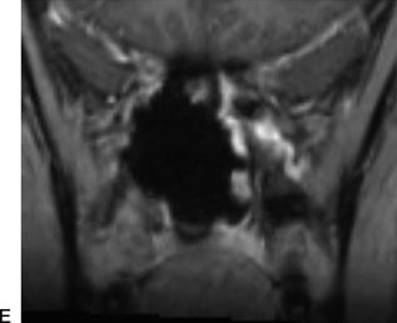
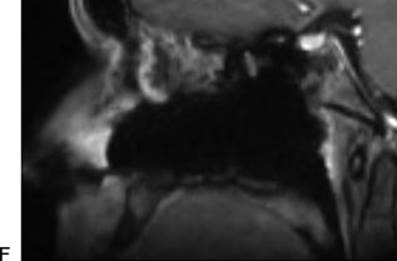
FIGURE 7.5 Juvenile nasopharyngeal angiofibroma (Andrews stage IIIB) with infratemporal extension (marked with asterisk). Preoperative MR scan (T1 weighted with contrast enhancement) in axial (A), coronal (B), and sagittal (C) views. The patient underwent preoperative embolization followed by an endoscopic endonasal resection, opening a transmaxillary window to reach the ITF and drilling of the pterygoid processes and basisphenoid. The postoperative MR scan (T1 weighted) in axial (D), coronal (E), and sagittal (F) views shows the radical resection of the lesion. The black arrows mark the internal carotid artery bilaterally. (SS, sphenoid sinus; LPM lateral pterygoid muscle; cl, clivus; pMW, posterior maxillary wall; ITF, infratemporal fossa.)
In contrast, extensive lesions involving the cavernous sinus cannot always be completely removed by transnasal neuroendoscopic techniques. As a consequence, medical therapy and radiotherapy (stereotactic radiotherapy and radiosurgery) are still used as primary treatment for most lesions of the cavernous sinus. External intra-extradural approaches allow for the best surgical control in the 1% to 4% of pituitary tumors, which extend to areas inaccessible by a purely endoscopic route. In cases of large tumors with critical anatomic relationships, radiosurgery can be used after neuroendoscopic transnasal subtotal resection to provide long-term tumor control.
In our published series of 15 patients with defects of the cranial base located at the lateral sphenoid recess, no CSF leaks or serious complication has been observed. We rely on multilayer technique or gasket seal closure for most of our cases without a need for sinus obliteration or balloon stenting.
PEARLS
· Intranasal “four-handed” technique has offered otorhinolaryngologists and neurosurgeons the opportunity of “between-specialist” surgical training that leads to a profitable exchange of technical skills.
· It is important to use a neuronavigation system with CT/MR fusion images or angio-CT for better visualization of adjacent vascular structures. Surgical Doppler ultrasound is a helpful device for detection of major vessels.
· Preservation of the cranial part of the basal lamella (common lamella) and olfactory neuroepithelium is recommended.
· During opening of the lateral wall of the sphenoid sinus, the intrasphenoidal anatomical landmarks have to be identified.
· The posterior wall of the maxillary sinus, vidian foramen, foramen rotundum, Eustachian tube, and sphenoid indentation of ICA are important landmarks.
· The VI cranial nerve runs through the cavernous sinus in a midlateral direction.
· The use of fibrillar collagen and fibrin glue permits management of venous bleeding.
PITFALLS
· Before the decision is made to operate, it is important to establish a tentative diagnosis by considering the radiologic characteristics and then confirm this by tissue biopsy.
· It is important to determine the relationship of the lesion with the surrounding neurovascular structures. Investigate the presence of any vascular adherence or invasion in order to avoid iatrogenic damage or pointless surgical removal.
· It must be stressed that every time an endonasal endoscopic approach is encountered, thorough knowledge of the anatomy of the area is the primary prerequisite. Training by cadaver dissection is one way for better understanding this complex anatomy. The surgeon should have a thorough knowledge of the traditional external approaches to be able to handle any complications that may arise.
· Patients should be always informed about the possible surgical approaches, whether endonasal, external, or combined approaches. A thorough discussion about the risk of complications and sequelae of the operation should be clarified. Patient education is important for a better perioperative period and long-term follow-up.
· It is extremely important to practice in a teamwork fashion. Treatment decisions should be approved by a multidisciplinary group to provide the patient with the maximum benefits of the expertise.
INSTRUMENTS TO HAVE AVAILABLE
· Neuronavigation system with CT/MR fusion images or angio-CT
· Surgical Doppler ultrasound
· Dedicated cranial base surgical equipment (straight and angled endoscopes, dedicated cutting instruments, and suctions)
· High-speed intranasal drill
· Intranasal bipolar cautery
· Hemostatic materials
SUGGESTED READING
Kassam AB, Gardner P, Snyderman C, et al. Expanded endonasal approach: fully endoscopic, completely transnasal approach to the middle third of the clivus, petrous bone, middle cranial fossa, and infratemporal fossa. Neurosurg Focus 2005;19(1):E6.
Castelnuovo P, Dallan I, Pistochini A, et al. Endonasal endoscopic repair of Sternberg's canal cerebrospinal fluid leaks. Laryngoscope 2007;117(2):345–349.
Dallan I, Lenzi R, Bignami M, et al. Endoscopic transnasal anatomy of the infratemporal fossa and upper parapharyngeal regions: correlations with traditional perspectives and surgical implications. Minim Invasive Neurosurg 2010;53(5–6):261–269.
Stamm AC, ed. Transnasal Endoscopic Skull Base and Brain Surgery: Tips and Pearls. Thieme Medical Publishers, New York, NY. August 2011. ISBN: 1604063106.
Kennedy DW, ed. Rhinology: Diseases of the Nose, Sinuses, and Skull Base. Thieme Medical Publishers Inc., New York, NY. May 2012 ISBN: 1604060603.