Eric J. Wall and James R. Romanowski
DEFINITION
![]() Patellar instability in children and adolescents usually involves an episode of complete dislocation of the patella from the trochlear groove. Occasionally there can be episodes of patella subluxation without gross dislocation.
Patellar instability in children and adolescents usually involves an episode of complete dislocation of the patella from the trochlear groove. Occasionally there can be episodes of patella subluxation without gross dislocation.
![]() There are two types of patella dislocation.
There are two types of patella dislocation.
![]() Acute traumatic patella dislocation
Acute traumatic patella dislocation
![]() Atraumatic dislocations or subluxation secondary to ligamentous laxity
Atraumatic dislocations or subluxation secondary to ligamentous laxity
![]() First-time patella dislocations tend to occur most commonly in adolescent high-level athletes.2
First-time patella dislocations tend to occur most commonly in adolescent high-level athletes.2
![]() Pain is often associated with episodes of dislocation, but chronic patellofemoral pain is not usually the primary complaint.
Pain is often associated with episodes of dislocation, but chronic patellofemoral pain is not usually the primary complaint.
![]() The incidence of primary patella dislocation in 10- to 17-year-olds is reported at 29 and 43 per 100,000.6
The incidence of primary patella dislocation in 10- to 17-year-olds is reported at 29 and 43 per 100,000.6
ANATOMY
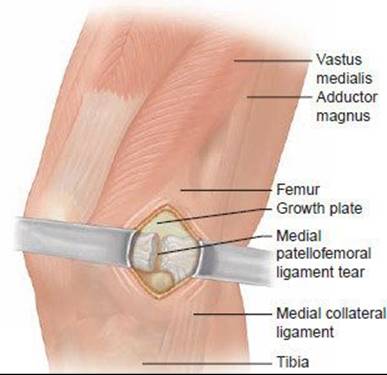
![]() Traumatic dislocation of the patella occurs almost exclusively in the lateral direction and often results in a tear of the medial patellofemoral ligament (MPFL) off the femur or the patella or in its midsubstance (FIG 1A).
Traumatic dislocation of the patella occurs almost exclusively in the lateral direction and often results in a tear of the medial patellofemoral ligament (MPFL) off the femur or the patella or in its midsubstance (FIG 1A).
![]() The MPFL provides 50% to 80% of the restraining force to lateral patella displacement.8
The MPFL provides 50% to 80% of the restraining force to lateral patella displacement.8
![]() It is a flat band adjacent to the medial retinaculum that courses between the medial epicondyle of the femur and the medial patella.
It is a flat band adjacent to the medial retinaculum that courses between the medial epicondyle of the femur and the medial patella.
![]() It inserts into the superior two thirds of the patella on its medial aspect.
It inserts into the superior two thirds of the patella on its medial aspect.
![]() Specifically, the MPFL attaches into the femur just distal to the adductor tubercle and just superoposterior to the medial epicondyle (FIG 1B).12
Specifically, the MPFL attaches into the femur just distal to the adductor tubercle and just superoposterior to the medial epicondyle (FIG 1B).12
![]() In a skeletally immature patient, the MPFL appears to attach to the femur between the growth plate and the medial epicondyle.
In a skeletally immature patient, the MPFL appears to attach to the femur between the growth plate and the medial epicondyle.
![]() Traumatic dislocation can cause a serious fracture of the medial patella facet (FIG 1C) or the lateral femoral condyle (FIG 1D) and can be cartilaginous or osteocartilaginous.
Traumatic dislocation can cause a serious fracture of the medial patella facet (FIG 1C) or the lateral femoral condyle (FIG 1D) and can be cartilaginous or osteocartilaginous.
![]() Stanitski found a 71% incidence of osteochondral injury at arthroscopy after patella dislocation, most of which was radiographically occult.16
Stanitski found a 71% incidence of osteochondral injury at arthroscopy after patella dislocation, most of which was radiographically occult.16
![]() More frequently there is a less serious nonarticular avulsion fracture of the MPFL off the medial patella.
More frequently there is a less serious nonarticular avulsion fracture of the MPFL off the medial patella.
![]() There can be an immediate or delayed appearance of an ossific lesion at the avulsion site off the medial patella (FIG 1E).
There can be an immediate or delayed appearance of an ossific lesion at the avulsion site off the medial patella (FIG 1E).
![]() A shallow trochlea groove, patella alta, patellar tilt, and a lateralized tibial tubercle can increase the risk of dislocation,5 along with a hypoplastic tibial tubercle and valgus knee alignment.
A shallow trochlea groove, patella alta, patellar tilt, and a lateralized tibial tubercle can increase the risk of dislocation,5 along with a hypoplastic tibial tubercle and valgus knee alignment.
PATHOGENESIS
![]() Noncontact patellar dislocation during sports usually involves lower extremity internal rotation combined with knee valgus on a planted foot (a mechanism very similar to anterior cruciate ligament injury).
Noncontact patellar dislocation during sports usually involves lower extremity internal rotation combined with knee valgus on a planted foot (a mechanism very similar to anterior cruciate ligament injury).
![]() Less commonly, patella dislocation is caused by a direct blow that pushes the kneecap laterally.
Less commonly, patella dislocation is caused by a direct blow that pushes the kneecap laterally.
![]() Most episodes of traumatic patella dislocation spontaneously reduce in the field.
Most episodes of traumatic patella dislocation spontaneously reduce in the field.
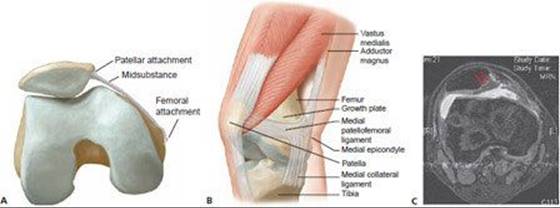

FIG 1 • A. The medial patellofemoral (MPFL) ligament can tear off the femoral or patellar origin or in its midsubstance. B. The MPFL tethers the medial patella to the medial condyle of the femur. It arises from the superior two thirds of the medial border of the patella and inserts between the adductor tubercle and medial epicondyle. Its insertion is just distal to the growth plate. C. The entire medial cartilaginous facet of the patella has separated from the underlying bone after a primary traumatic patellar dislocation. D. After patellar dislocation this patient has an osteochondral fracture of the lateral femoral condyle. E. Insignificant avulsion fracture off medial patella, which is pathognomonic for patellar dislocation.
![]() The common finding of a lateral femoral condyle bone bruise at the sulcus terminalis suggests that dislocation usually occurs at 70 to 80 degrees of flexion.14
The common finding of a lateral femoral condyle bone bruise at the sulcus terminalis suggests that dislocation usually occurs at 70 to 80 degrees of flexion.14
![]() Multiple anatomic factors are theorized to increase the risk of patella dislocation, such as family history, increased Q angle, femoral intorsion, tibial extorsion, knee valgus, trochlear groove dysplasia, and foot pronation. Only patella alta is a proven risk factor.3
Multiple anatomic factors are theorized to increase the risk of patella dislocation, such as family history, increased Q angle, femoral intorsion, tibial extorsion, knee valgus, trochlear groove dysplasia, and foot pronation. Only patella alta is a proven risk factor.3
NATURAL HISTORY
![]() After a primary patellar dislocation, there is only a 17% risk of recurrence. The risk of recurrence jumps to 49% if there is a history of prior patellar dislocation or subluxation.
After a primary patellar dislocation, there is only a 17% risk of recurrence. The risk of recurrence jumps to 49% if there is a history of prior patellar dislocation or subluxation.
![]() Young age was also associated with recurrence, as was a positive family history.6
Young age was also associated with recurrence, as was a positive family history.6
![]() At 6 months after patellar dislocation, only 69% of patients had returned to sports.3
At 6 months after patellar dislocation, only 69% of patients had returned to sports.3
![]() At 2 to 5 years of follow-up after patellar dislocation, Fithian and coworkers6 showed no radiographic or scintigraphic evidence of degenerative joint disease.
At 2 to 5 years of follow-up after patellar dislocation, Fithian and coworkers6 showed no radiographic or scintigraphic evidence of degenerative joint disease.
![]() At 6 to 26 years of follow-up after nonoperative treatment for patellar dislocation, 22% of knees showed arthritic changes compared to 11% of each patient's opposite uninjured knee.9
At 6 to 26 years of follow-up after nonoperative treatment for patellar dislocation, 22% of knees showed arthritic changes compared to 11% of each patient's opposite uninjured knee.9
![]() At least 30% to 50% of patients with patella dislocation will have knee pain more than 2 years after injury,7 and 69% of athletes will decrease their sports activity.
At least 30% to 50% of patients with patella dislocation will have knee pain more than 2 years after injury,7 and 69% of athletes will decrease their sports activity.
![]() Young age and skeletal immaturity, especially in females, is associated with worse prognosis.11
Young age and skeletal immaturity, especially in females, is associated with worse prognosis.11
![]() Overall, the natural history is not improved with the routine operative stabilization of primary dislocations.2,4,11
Overall, the natural history is not improved with the routine operative stabilization of primary dislocations.2,4,11
PATIENT HISTORY AND PHYSICAL FINDINGS
![]() Most episodes of patellar dislocation spontaneously reduce in the field.
Most episodes of patellar dislocation spontaneously reduce in the field.
![]() Patients with an acute traumatic patella dislocation often present to the emergency room with a history of a noncontact or contact injury to their knee, and many do not recognize the injury as a patellar dislocation.
Patients with an acute traumatic patella dislocation often present to the emergency room with a history of a noncontact or contact injury to their knee, and many do not recognize the injury as a patellar dislocation.
![]() An effusion is usually present after traumatic dislocation but is rarely present after atraumatic dislocations. If the patella is still dislocated, the emergency physician usually performs a reduction by slowly extending the knee from its flexed position.
An effusion is usually present after traumatic dislocation but is rarely present after atraumatic dislocations. If the patella is still dislocated, the emergency physician usually performs a reduction by slowly extending the knee from its flexed position.
![]() Patella dislocation that spontaneously reduces in the field may mimic the history and presentation of an anterior cruciate ligament tear.
Patella dislocation that spontaneously reduces in the field may mimic the history and presentation of an anterior cruciate ligament tear.
![]() The patella apprehension sign is the best test for patellar instability. With the knee flexed over a bolster at 25 degrees, the patella is translated laterally. If the patient exhibits apprehension, the test is positive.
The patella apprehension sign is the best test for patellar instability. With the knee flexed over a bolster at 25 degrees, the patella is translated laterally. If the patient exhibits apprehension, the test is positive.
![]() Patella glide test: With knee flexed 25 to 30 degrees, the patella is gently translated laterally. Lateral translation of more than two quadrants of the patella may indicate instability.
Patella glide test: With knee flexed 25 to 30 degrees, the patella is gently translated laterally. Lateral translation of more than two quadrants of the patella may indicate instability.
![]() Testing for the J sign (patella pulls laterally as knee reaches full extension, in the path of an upside-down J) can identify proximal alignment issues.
Testing for the J sign (patella pulls laterally as knee reaches full extension, in the path of an upside-down J) can identify proximal alignment issues.
IMAGING AND OTHER DIAGNOSTIC STUDIES
![]() Knee radiographs should include the anteroposterior (AP), lateral, and sunrise (or Merchant) views.
Knee radiographs should include the anteroposterior (AP), lateral, and sunrise (or Merchant) views.
![]() The sunrise or Merchant view requires a patient to flex the knee 30 to 45 degrees, which may be impossible owing to pain at the initial time of presentation in the emergency department. The sunrise view can usually be obtained at the first follow-up visit.
The sunrise or Merchant view requires a patient to flex the knee 30 to 45 degrees, which may be impossible owing to pain at the initial time of presentation in the emergency department. The sunrise view can usually be obtained at the first follow-up visit.
![]() Plain radiographs can miss 40% of arthroscopically documented chondral or osteochondral lesions. Many reparable osteochondral injuries show only a sliver of bone on one view in the plain radiographic series, which can be easily overlooked (FIG 2A).
Plain radiographs can miss 40% of arthroscopically documented chondral or osteochondral lesions. Many reparable osteochondral injuries show only a sliver of bone on one view in the plain radiographic series, which can be easily overlooked (FIG 2A).
![]() Because of the high rate of occult articular or osteoarticular injury, we recommend an MRI scan on patients who present with a large traumatic effusion.
Because of the high rate of occult articular or osteoarticular injury, we recommend an MRI scan on patients who present with a large traumatic effusion.
![]() The site of MPFL ligament disruption can often be identified on MRI. MRI is reported to be 85% sensitive and 70% accurate (FIG 2B).15
The site of MPFL ligament disruption can often be identified on MRI. MRI is reported to be 85% sensitive and 70% accurate (FIG 2B).15
![]() Patellar dislocation produces a signature bone contusion pattern in which the medial patella and the midportion of the lateral femoral condyle show increased signal (FIG 2C). This bone bruise pattern is distinct from that associated with anterior cruciate ligament tears.
Patellar dislocation produces a signature bone contusion pattern in which the medial patella and the midportion of the lateral femoral condyle show increased signal (FIG 2C). This bone bruise pattern is distinct from that associated with anterior cruciate ligament tears.
DIFFERENTIAL DIAGNOSIS
![]() Anterior cruciate, medial collateral, lateral collateral, or posterior cruciate ligament tear
Anterior cruciate, medial collateral, lateral collateral, or posterior cruciate ligament tear
![]() Meniscal tear
Meniscal tear
![]() Patellofemoral pain syndrome
Patellofemoral pain syndrome
![]() Knee contusion
Knee contusion
![]() Osteoarticular fracture
Osteoarticular fracture
NONOPERATIVE MANAGEMENT
![]() Initial management of traumatic patellar dislocation after reduction is with a knee immobilizer, analgesia with oral narcotics, and crutch walking (weight bearing as tolerated).
Initial management of traumatic patellar dislocation after reduction is with a knee immobilizer, analgesia with oral narcotics, and crutch walking (weight bearing as tolerated).
![]() The risk of redislocation is three times higher in patients treated with immediate mobilization versus immobilization with cast or brace.10 The authors use a knee immobilizer for 4 weeks.
The risk of redislocation is three times higher in patients treated with immediate mobilization versus immobilization with cast or brace.10 The authors use a knee immobilizer for 4 weeks.
![]() Initial nonoperative management of acute patellar instability in children begins with the management of any residual acute symptoms, such as pain and swelling.
Initial nonoperative management of acute patellar instability in children begins with the management of any residual acute symptoms, such as pain and swelling.
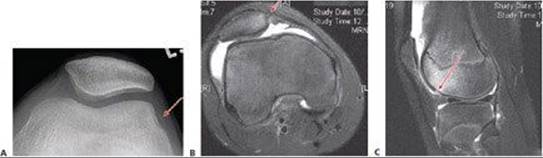
FIG 2 • A. Osteochondral fragment. Post-patellar dislocation radiographic sunrise view shows a subtle sliver of bone (arrow), which on arthroscopy proved to be a large osteochondral fracture from the lateral condyle that was repaired with screw fixation. B. Medial patellofemoral ligament (MPFL) tear off patella. MRI shows disruption of MPFL off its origin from the patella (arrow), with increased signal on medial patella. C. Lateral femoral condyle bone bruise on MRI scan after a patella dislocation. There is a subtle break in the articular cartilage (arrow). The location of the bruise provides evidence that the patella usually dislocates with the knee in 70 to 80 degrees of flexion.
![]() Modalities and exercise are used to control effusion, restore normal range of motion, and initiate quadriceps activation.
Modalities and exercise are used to control effusion, restore normal range of motion, and initiate quadriceps activation.
![]() Once these symptoms have resolved, the focus of conservative management turns to providing dynamic stability through strengthening. This typically includes proximal hip and core strengthening as well as local quadriceps and hamstrings strengthening.
Once these symptoms have resolved, the focus of conservative management turns to providing dynamic stability through strengthening. This typically includes proximal hip and core strengthening as well as local quadriceps and hamstrings strengthening.
![]() The final stages of rehabilitation before return to activity focus on restoring functional strength and assessing the child's dynamic stability and readiness to return safely to functional activities with minimal risk of recurrence.
The final stages of rehabilitation before return to activity focus on restoring functional strength and assessing the child's dynamic stability and readiness to return safely to functional activities with minimal risk of recurrence.
SURGICAL MANAGEMENT
![]() Operative treatment is indicated for first-time patellar dislocation that fails to reduce concentrically, or that involves osteochondral damage necessitating repair or removal of a loose body.
Operative treatment is indicated for first-time patellar dislocation that fails to reduce concentrically, or that involves osteochondral damage necessitating repair or removal of a loose body.
![]() Osteochondral lesions larger than 1 cm in diameter should be repaired if any bone is attached to the chondral fragment. Fixation devices should be countersunk 1 to 2 mm beneath the cartilage surface.
Osteochondral lesions larger than 1 cm in diameter should be repaired if any bone is attached to the chondral fragment. Fixation devices should be countersunk 1 to 2 mm beneath the cartilage surface.
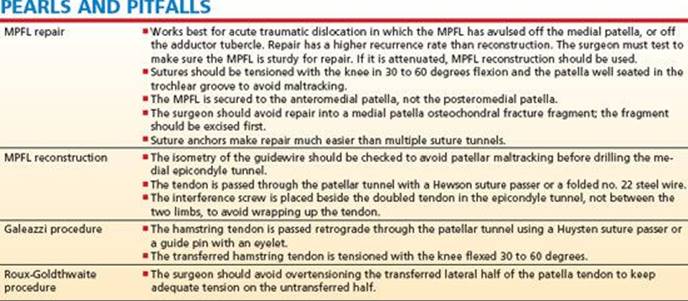
![]() The MPFL can be repaired at the time of surgery for osteochondral lesions in acute dislocations, but the recurrence rate is higher with repair versus reconstruction.
The MPFL can be repaired at the time of surgery for osteochondral lesions in acute dislocations, but the recurrence rate is higher with repair versus reconstruction.
![]() Reconstruction (versus repair) is indicated for recurrent instability, or in patients who are noted to have an attenuated MPFL at the time of surgery.
Reconstruction (versus repair) is indicated for recurrent instability, or in patients who are noted to have an attenuated MPFL at the time of surgery.
![]() MPFL reconstruction is not indicated for malalignment, patellofemoral pain, or arthrosis.
MPFL reconstruction is not indicated for malalignment, patellofemoral pain, or arthrosis.
![]() Lateral release is rarely necessary with repair or reconstruction of the MPFL.
Lateral release is rarely necessary with repair or reconstruction of the MPFL.
![]() Recurrent traumatic dislocations and recurrent atraumatic dislocations that fail bracing and physical therapy can benefit from surgical patella realignment.
Recurrent traumatic dislocations and recurrent atraumatic dislocations that fail bracing and physical therapy can benefit from surgical patella realignment.
![]() Tibial tubercle realignment procedures should be avoided in skeletally immature patients with open growth plates because of the risk of creating iatrogenic genu recurvatum from growth arrest.
Tibial tubercle realignment procedures should be avoided in skeletally immature patients with open growth plates because of the risk of creating iatrogenic genu recurvatum from growth arrest.
Preoperative Planning
![]() MRI scans should be reviewed to determine the size and location of osteochondral fractures and their potential for repair versus removal.
MRI scans should be reviewed to determine the size and location of osteochondral fractures and their potential for repair versus removal.
![]() Small metallic or bioabsorbable screws or pins should be available for osteochondral fracture repair.
Small metallic or bioabsorbable screws or pins should be available for osteochondral fracture repair.
![]() MRI can locate the site of MPFL failure with 70% accuracy to help target the site of repair (patella versus femoral side of ligament).
MRI can locate the site of MPFL failure with 70% accuracy to help target the site of repair (patella versus femoral side of ligament).
![]() Examination under anesthesia involves testing lateral patella tracking and checking overall knee stability.
Examination under anesthesia involves testing lateral patella tracking and checking overall knee stability.
Positioning
![]() The patient is positioned supine on a table that will allow knee imaging (FIG 3).
The patient is positioned supine on a table that will allow knee imaging (FIG 3).
![]() An intravenous bag is taped to the table to allow blocking the knee at about 30 to 60 degrees flexion during patella repair and reconstruction tensioning.
An intravenous bag is taped to the table to allow blocking the knee at about 30 to 60 degrees flexion during patella repair and reconstruction tensioning.
Approach
![]() The surgeon uses an approach through the anterior knee midline or a medial parapatellar approach. If needed, the hamstring semitendinosus graft is harvested through a standard proximal medial tibial approach with a tendon stripper.
The surgeon uses an approach through the anterior knee midline or a medial parapatellar approach. If needed, the hamstring semitendinosus graft is harvested through a standard proximal medial tibial approach with a tendon stripper.

FIG 3 • Operating room position. Patients are positioned supine on a radiolucent operating room table. A bump is placed under the ipsilateral hip to help balance the knee in flexed position. An intravenous bag is taped to the table to act as a block to hold the knee in flexion during tensioning of the repair or reconstruction.
TECHNIQUES
MEDIAL PATELLOFEMORAL LIGAMENT REPAIR
![]() A 3- to 5-cm longitudinal incision is made centered over the medial border of the patella.
A 3- to 5-cm longitudinal incision is made centered over the medial border of the patella.
![]() Sharp dissection is carried to the bony surface of the patella with a subperiosteal incision down to bone in a vertical line about 1.5 cm lateral to the medial patellar border (TECH FIG 1A).
Sharp dissection is carried to the bony surface of the patella with a subperiosteal incision down to bone in a vertical line about 1.5 cm lateral to the medial patellar border (TECH FIG 1A).
![]() The periosteum and all overlying soft tissues are collectively elevated off the medial patella and a tissue plane is developed in the fatty plane between the retinaculum and synovial joint capsule using Metzenbaum or curved tenotomy scissors.
The periosteum and all overlying soft tissues are collectively elevated off the medial patella and a tissue plane is developed in the fatty plane between the retinaculum and synovial joint capsule using Metzenbaum or curved tenotomy scissors.
![]() This soft tissue tunnel is expanded down toward the medial epicondyle of the femur.
This soft tissue tunnel is expanded down toward the medial epicondyle of the femur.
![]() It is not necessary to enter the joint space, and this should be avoided.
It is not necessary to enter the joint space, and this should be avoided.
![]() A finger is placed in the tunnel that lies just outside the synovium of the knee joint but is deep to the MPFL.
A finger is placed in the tunnel that lies just outside the synovium of the knee joint but is deep to the MPFL.
![]() The MPFL can be digitally palpated on its inner surface down to the medial epicondyle to determine its suitability for repair versus reconstruction.
The MPFL can be digitally palpated on its inner surface down to the medial epicondyle to determine its suitability for repair versus reconstruction.
![]() It should feel like a stout band of tissue originating from the medial epicondyle when traction is applied on its patellar end with a Kocher clamp (TECH FIG 1B).
It should feel like a stout band of tissue originating from the medial epicondyle when traction is applied on its patellar end with a Kocher clamp (TECH FIG 1B).
![]() A rongeur or burr is used for superficial decortication of the exposed anterior medial patella, thus creating a bed for healing of the advanced MPFL.
A rongeur or burr is used for superficial decortication of the exposed anterior medial patella, thus creating a bed for healing of the advanced MPFL.
![]() Multiple extra-articular drill holes (three or four) are placed in the patella to create transosseous suture tunnels for imbrication.
Multiple extra-articular drill holes (three or four) are placed in the patella to create transosseous suture tunnels for imbrication.
![]() Suture anchors can be used as an alternative for fixation to the patella (TECH FIG 1C).
Suture anchors can be used as an alternative for fixation to the patella (TECH FIG 1C).
![]() No. 2 or stronger nonabsorbable sutures are placed through the patella tunnels and woven through the advanced MPFL.
No. 2 or stronger nonabsorbable sutures are placed through the patella tunnels and woven through the advanced MPFL.
![]() The MPFL should be sutured to the anteromedial surface of the patella, not the posteromedial surface (TECH FIG 1D).
The MPFL should be sutured to the anteromedial surface of the patella, not the posteromedial surface (TECH FIG 1D).
![]() The tension should be set with the knee at 45 to 60 degrees of flexion to prevent overcorrection or undercorrection.
The tension should be set with the knee at 45 to 60 degrees of flexion to prevent overcorrection or undercorrection.
![]() The remaining free lateral edge of the MPFL tissue is sewn down to the patellar soft tissue with a running 2-0 suture.
The remaining free lateral edge of the MPFL tissue is sewn down to the patellar soft tissue with a running 2-0 suture.
![]() The knee should be placed through a range of motion to assess the repair's ability to prevent dislocation and maltracking in all degrees of knee flexion and extension.
The knee should be placed through a range of motion to assess the repair's ability to prevent dislocation and maltracking in all degrees of knee flexion and extension.
![]() The wounds are irrigated and the skin is closed.
The wounds are irrigated and the skin is closed.
TECH FIG 1 • A. Medial patellofemoral ligament (MPFL) repair. A 3- to 5-cm incision is made just medial to the patella and the soft tissue and periosteum are elevated off the medial 1 to 1.5 cm of the patella. Soft tissue is elevated down to the fatty layer just outside the knee capsule and synovium. B. MPFL palpation. The surgeon's finger is placed in the extrasynovial tunnel created deep to the MPFL and medial retinaculum. From inside out, the MPFL is palpated to determine its suitability for repair or the necessity for reconstruction. The MPFL should feel like a stout band originating off the medial epicondyle. C. Suture is placed through holes drilled in the medial patellar bone. D. A no. 2 nonabsorbable suture is woven through the MPFL and secured down to the medial patellar bone.
MEDIAL PATELLOFEMORAL LIGAMENT RECONSTRUCTION
![]() A 3- to 5-cm medial patellar longitudinal skin incision is carried down to the medial patella and the initial dissection is similar to the above MPFL repair.
A 3- to 5-cm medial patellar longitudinal skin incision is carried down to the medial patella and the initial dissection is similar to the above MPFL repair.
![]() A thick periosteal flap is elevated off the medial 1 to 1.5 cm of the patella and carried down to the medial fibrofatty layer just outside the knee synovium.
A thick periosteal flap is elevated off the medial 1 to 1.5 cm of the patella and carried down to the medial fibrofatty layer just outside the knee synovium.
![]() An extrasynovial tunnel is created down to the medial epicondyle.
An extrasynovial tunnel is created down to the medial epicondyle.
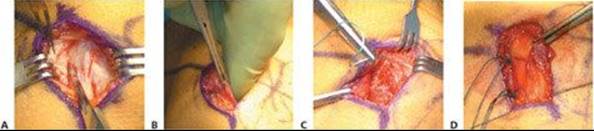
![]() The semitendinosus tendon (single tendon) is harvested using standard technique with a tendon stripper, and no. 2 Ethibond suture is placed in each end of tendon with a Krackow type of locking stitch (TECH FIG 2A).
The semitendinosus tendon (single tendon) is harvested using standard technique with a tendon stripper, and no. 2 Ethibond suture is placed in each end of tendon with a Krackow type of locking stitch (TECH FIG 2A).
![]() The doubled tendon is sized usually to 5 to 6 mm in diameter.
The doubled tendon is sized usually to 5 to 6 mm in diameter.
![]() A 2-cm incision is made over the medial epicondyle and an anterior cruciate ligament guide pin is placed just anterior and proximal to the medial epicondyle.
A 2-cm incision is made over the medial epicondyle and an anterior cruciate ligament guide pin is placed just anterior and proximal to the medial epicondyle.
![]() Because the medial epicondyle is difficult to palpate, the guide pin's location should be verified with AP and lateral fluoroscopy.
Because the medial epicondyle is difficult to palpate, the guide pin's location should be verified with AP and lateral fluoroscopy.
![]() In skeletally immature children, the guide pin should be 4 to 5 mm distal to the growth plate.
In skeletally immature children, the guide pin should be 4 to 5 mm distal to the growth plate.
![]() A 4-mm transosseous tunnel is drilled in the medial patella just superior to the equator.
A 4-mm transosseous tunnel is drilled in the medial patella just superior to the equator.
![]() An umbilical tape is passed through the patella tunnel and under the medial retinaculum and around the guide pin to test isometry. The tape is tightened at 30 to 60 degrees of flexion.
An umbilical tape is passed through the patella tunnel and under the medial retinaculum and around the guide pin to test isometry. The tape is tightened at 30 to 60 degrees of flexion.

TECH FIG 2 • A. Harvest of semitendinosus, showing the fibrous band diverging posteromedially toward the gastrocnemius. These bands must be cut before passing a tendon stripper. B,C. A soft tissue interference screw is placed in the femoral bone tunnel to lock the hamstring graft into the tunnel after the looped graft is pulled into the tunnel when the guide pin is advanced across the femur.
![]() If the patella tracks medially in flexion, the pin is moved distal; if the patella tracks medial in extension, the pin is moved slightly proximally. If the pin is too anterior, the tape will tighten in terminal extension and flexion. If the pin is too posterior, the tape will loosen in terminal extension and flexion.
If the patella tracks medially in flexion, the pin is moved distal; if the patella tracks medial in extension, the pin is moved slightly proximally. If the pin is too anterior, the tape will tighten in terminal extension and flexion. If the pin is too posterior, the tape will loosen in terminal extension and flexion.
![]() The Beath needle guide pin is advanced across the distal femur condyle until it comes out the lateral skin, avoiding the patellofemoral joint anteriorly and the common peroneal nerve posteriorly. A 5 × 25-mm tunnel is drilled over the guide pin.
The Beath needle guide pin is advanced across the distal femur condyle until it comes out the lateral skin, avoiding the patellofemoral joint anteriorly and the common peroneal nerve posteriorly. A 5 × 25-mm tunnel is drilled over the guide pin.
![]() The tendon is folded in half and looped over a no. 5 nonabsorbable suture. The no. 5 suture ends are placed into the eyelet of the Beath needle.
The tendon is folded in half and looped over a no. 5 nonabsorbable suture. The no. 5 suture ends are placed into the eyelet of the Beath needle.
![]() The folded end of the tendon is drawn into the tunnel as the guidewire and no. 5 suture are advanced across the knee condyles to exit laterally.
The folded end of the tendon is drawn into the tunnel as the guidewire and no. 5 suture are advanced across the knee condyles to exit laterally.
![]() A soft tissue interference screw matched to the tunnel size (same size) is then placed to lock the folded double end of the hamstring graft securely in the tunnel (TECH FIG 2B,C).
A soft tissue interference screw matched to the tunnel size (same size) is then placed to lock the folded double end of the hamstring graft securely in the tunnel (TECH FIG 2B,C).
![]() The two free ends of the graft are routed under the medial retinaculum up toward the patella.
The two free ends of the graft are routed under the medial retinaculum up toward the patella.
![]() One end of the tendon is passed through the patella tunnel and then sewn to the other end of the tendon with the knee flexed to about 45 degrees while the patella is held firmly in the trochlear groove.
One end of the tendon is passed through the patella tunnel and then sewn to the other end of the tendon with the knee flexed to about 45 degrees while the patella is held firmly in the trochlear groove.
![]() Patella tracking and stability are tested through a full range of motion.
Patella tracking and stability are tested through a full range of motion.
![]() Standard closure is performed and a knee immobilizer is placed.
Standard closure is performed and a knee immobilizer is placed.
GALEAZZI PROCEDURE (SEMITENDINOSUS TENODESIS)
![]() The semitendinosus tendon (posterior and distal to the gracilis) is harvested with an open tendon stripper and the distal tendon is left attached to the proximal tibia.
The semitendinosus tendon (posterior and distal to the gracilis) is harvested with an open tendon stripper and the distal tendon is left attached to the proximal tibia.
![]() The free end of the tendon is secured with a Krakow type of locking stitch of no. 2 nonabsorbable suture.
The free end of the tendon is secured with a Krakow type of locking stitch of no. 2 nonabsorbable suture.
![]() Through a midline incision, the patella is exposed to allow an oblique 4- to 5-mm drill hole placed from proximal lateral to distal medial in the coronal plane of the patella.
Through a midline incision, the patella is exposed to allow an oblique 4- to 5-mm drill hole placed from proximal lateral to distal medial in the coronal plane of the patella.
![]() A lateral release is performed about 1 cm lateral to the patella, extending from the proximal tibia to 1 cm above the proximal patella.
A lateral release is performed about 1 cm lateral to the patella, extending from the proximal tibia to 1 cm above the proximal patella.
![]() The free end of the semitendinosus is passed retrograde up through the oblique tunnel and the free end is folded back across the anterior surface of the patella periosteum and sutured to the anterior patella, or sewn back to itself if its length permits (TECH FIG 3).
The free end of the semitendinosus is passed retrograde up through the oblique tunnel and the free end is folded back across the anterior surface of the patella periosteum and sutured to the anterior patella, or sewn back to itself if its length permits (TECH FIG 3).
![]() The graft should be tensioned and fixed with the knee at 45 to 60 degrees flexion.
The graft should be tensioned and fixed with the knee at 45 to 60 degrees flexion.
![]() A knee immobilizer is placed, and the patient may bear weight as tolerated. Early motion is encouraged.
A knee immobilizer is placed, and the patient may bear weight as tolerated. Early motion is encouraged.
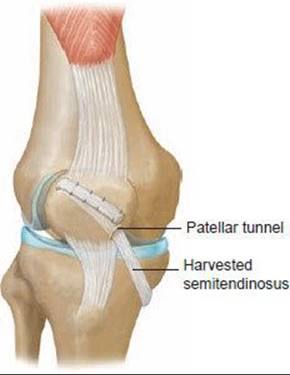
TECH FIG 3 • Galeazzi procedure. Semitendinosus is harvested and left attached distally. The free end of the graft is fixed into the oblique patellar tunnel.
ROUX-GOLDTHWAITE PATELLA TENDON HEMITRANSFER
![]() A midline incision about 5 to 6 cm long is taken down to the patella tendon and the proximal tibia.
A midline incision about 5 to 6 cm long is taken down to the patella tendon and the proximal tibia.
![]() A lateral release is performed from about 1 to 2 cm above the proximal pole of the patella, distal to the tibial tubercle.
A lateral release is performed from about 1 to 2 cm above the proximal pole of the patella, distal to the tibial tubercle.
![]() The patella tendon is split in its midline and the distal end of the lateral half is released from the proximal tibia insertion without damaging the cartilaginous tibial tubercle.
The patella tendon is split in its midline and the distal end of the lateral half is released from the proximal tibia insertion without damaging the cartilaginous tibial tubercle.
![]() The free end of the lateral tendon is passed posterior to the medial tendon and brought out and sewn into the soft tissue of the medial proximal tibia, preferably into the insertion of the sartorius muscle (TECH FIG 4).
The free end of the lateral tendon is passed posterior to the medial tendon and brought out and sewn into the soft tissue of the medial proximal tibia, preferably into the insertion of the sartorius muscle (TECH FIG 4).
![]() The hemitransfer is tensioned in 45 to 60 degrees of flexion, with equal tension on both halves of the tendon.
The hemitransfer is tensioned in 45 to 60 degrees of flexion, with equal tension on both halves of the tendon.
![]() The knee is immobilized for 4 to 6 weeks.
The knee is immobilized for 4 to 6 weeks.
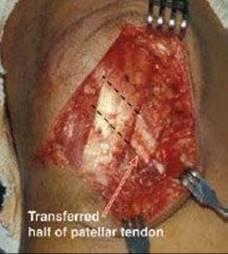
TECH FIG 4 • Roux-Goldthwaite procedure in which the lateral half of the patella tendon is transferred into the soft tissue of the medial proximal tibia.
MEDIAL PATELLOFEMORAL LIGAMENT REPAIR ON FEMORAL SIDE
![]() A 4-cm oblique incision is made over the adductor tubercle and medial epicondyle down through the covering fascia.
A 4-cm oblique incision is made over the adductor tubercle and medial epicondyle down through the covering fascia.
![]() The distal belly of the vastus medius obliquus muscle and the torn edge of the MPFL are repaired to the soft tissue stump, or the avulsed edge is repaired to the bare bone of the adductor tubercle with suture anchors (TECH FIG 5).
The distal belly of the vastus medius obliquus muscle and the torn edge of the MPFL are repaired to the soft tissue stump, or the avulsed edge is repaired to the bare bone of the adductor tubercle with suture anchors (TECH FIG 5).
![]() Care is taken to avoid damage to the branches of the saphenous nerve.
Care is taken to avoid damage to the branches of the saphenous nerve.
![]() Early mobilization, weight bearing, and strengthening are encouraged to avoid knee stiffness.14
Early mobilization, weight bearing, and strengthening are encouraged to avoid knee stiffness.14
TECH FIG 5 • Medial patellofemoral ligament (MPFL) repair of femoral-side tear or avulsion. The MPFL is directly repaired across the torn tendon or fixed back to bone.
POSTOPERATIVE CARE
![]() MPFL repair and reconstruction patients are placed in a knee immobilizer and are weight bearing as tolerated. Full range of motion starts 1 to 2 weeks postoperatively, and patients are advanced to plyometrics at 6 weeks postoperatively.
MPFL repair and reconstruction patients are placed in a knee immobilizer and are weight bearing as tolerated. Full range of motion starts 1 to 2 weeks postoperatively, and patients are advanced to plyometrics at 6 weeks postoperatively.
![]() Galeazzi procedure patients have similar rehabilitation due to solid fixation if the tendon is sewn to itself.
Galeazzi procedure patients have similar rehabilitation due to solid fixation if the tendon is sewn to itself.
![]() Roux-Goldthwaite procedure patients are kept toe-touch weight bearing for 6 weeks postoperatively owing to the less secure fixation of the transferred tendon into medial proximal tibia soft tissue.
Roux-Goldthwaite procedure patients are kept toe-touch weight bearing for 6 weeks postoperatively owing to the less secure fixation of the transferred tendon into medial proximal tibia soft tissue.
OUTCOMES
![]() MPFL reconstruction appears to be more reliable at preventing redislocation than other soft tissue procedures.
MPFL reconstruction appears to be more reliable at preventing redislocation than other soft tissue procedures.
![]() Nomura and associates13 reported that only 2 of 22 patients had a repeat subluxation or dislocation episode after MPFL reconstruction, with an average follow-up of 11.9 years.
Nomura and associates13 reported that only 2 of 22 patients had a repeat subluxation or dislocation episode after MPFL reconstruction, with an average follow-up of 11.9 years.
![]() Thaunat and Erasmus17 found that 3 of 148 MPFL reconstructions redislocated with an anatomically placed double loop of autogenous gracilis tendon. All failures were related to repeat trauma occurring at least 4 years from the index surgery.
Thaunat and Erasmus17 found that 3 of 148 MPFL reconstructions redislocated with an anatomically placed double loop of autogenous gracilis tendon. All failures were related to repeat trauma occurring at least 4 years from the index surgery.
![]() Andrish1 suggested that failed MPFL reconstructions associated with trochlear or patellar dysplasia often necessitate a trochleoplasty, tibial tubercle transfer, or both.
Andrish1 suggested that failed MPFL reconstructions associated with trochlear or patellar dysplasia often necessitate a trochleoplasty, tibial tubercle transfer, or both.
COMPLICATIONS
![]() Recurrence is seen in less than 10% of patients after MPFL reconstruction.
Recurrence is seen in less than 10% of patients after MPFL reconstruction.
![]() Patellofemoral pain is often unchanged from the preoperative condition.
Patellofemoral pain is often unchanged from the preoperative condition.
![]() Patients with severe patellofemoral arthrosis and patellofemoral pain syndrome may not benefit from these procedures.
Patients with severe patellofemoral arthrosis and patellofemoral pain syndrome may not benefit from these procedures.
![]() Skeletally mature patients may benefit from a procedure that moves the tibial tubercle more anterior (Fulkerson osteotomy).
Skeletally mature patients may benefit from a procedure that moves the tibial tubercle more anterior (Fulkerson osteotomy).
![]() Overtightening of medial soft tissue can result in medial dislocation. This is especially possible if a medial repair is tensioned in full extension or is combined with an extensive lateral release.
Overtightening of medial soft tissue can result in medial dislocation. This is especially possible if a medial repair is tensioned in full extension or is combined with an extensive lateral release.
![]() Care must be taken to avoid patella articular cartilage penetration when drilling patella holes, especially with the Galeazzi procedure.
Care must be taken to avoid patella articular cartilage penetration when drilling patella holes, especially with the Galeazzi procedure.
![]() With the Roux-Goldthwaite procedure, there are reports of patellar tendon rupture of the untransferred tendon.
With the Roux-Goldthwaite procedure, there are reports of patellar tendon rupture of the untransferred tendon.
REFERENCES
1. Andrish J. Surgical reconstruction of the medial patellofemoral ligament. Tech Knee Surg 2006;5:121–127.
2. Arnbjornsson A, Egund N, Rydling O, et al. The natural history of recurrent dislocation of the patella: long-term results of conservative and operative treatment. J Bone Joint Surg 1992;74B:140–142.
3. Atkin D, Fithian D, Marangi K, et al. Characteristics of patients with primary acute lateral patellar dislocation and their recovery within the first 6 months of injury. Am J Sports Med 2000;28:472–479.
4. Buncher M, Baudendistel B, Sabo D, et al. Acute traumatic primary patellar dislocation: long-term results comparing conservative and surgical treatment. Clin J Sport Med 2005;15:62–66.
5. Dejour H, Walch G, Nove-Josserand L, et al. Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc 1994;2:19–26.
6. Fithian D, Paxton E, Cohen A. Indications in the treatment of patellar instability. J Knee Surg 2004;17:47–56.
7. Hawkins RJ, Bell RH, Anisette G. Acute patellar dislocation: the natural history. Am J Sports Med 1985;14:117–120.
8. Hinton RY, Sharma KM. Acute and recurrent patellar instability in the young athlete. Orthop Clin North Am 2003;34:385–396.
9. Maenpaa H, Lehton MU. Patellar dislocation: the long-term results of nonoperative management in 100 patients. Am J Sports Med 1997;25:213–217.
10. Maenpaa H, Lehto MU. Patellefemoral osteoarthritis after patellar dislocation. Clin Orthop Relat Res 1997;339:156–162.
11. Nikku RL, Nietosvaara Y, Aalto K, et al. Operative treatment of primary patellar dislocation does not improve medium-term outcome. Acta Orthop 2005;76:699–704.
12. Nomura E, Horiuchi Y, Inoue M. Correlation of MR imaging findings and open exploration of medial patellofemoral ligament injuries in acute patellar dislocations. Knee 2002;9:139–143.
13. Nomura E, Inoue M, Kobayashi S. Long-term follow-up and knee osteoarthritis change after medial patellofemoral ligament reconstruction for recurrent patellar dislocation. Am J Sports Med 2007;35:1851–1858.
14. Sallay PI, Poggi J, Speer KP, et al. Acute dislocation of the patella: a correlative pathoanatomic study. Am J Sports Med 1996;24:52–60.
15. Sanders TG, Morrison WB, Singleton BA, et al. Medial patellofemoral ligament injury following acute transient dislocation of the patella: MR findings with surgical correlation in 14 patients. J Comput Assist Tomogr 2001;25:957–962.
16. Stanitski CL, Paletta GA Jr. Articular cartilage injury with acute patellar dislocation in adolescents: arthroscopic and radiographic correlation. Am J Sports Med 1998;26:52–55.
17. Thaunat M, Erasmus PK. Recurrent patellar dislocation after medial patellofemoral ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 2008;16:40–43.