John D. Lubahn and D. Patrick Williams
DEFINITION
![]() Rheumatoid arthritis is a progressive disease that, if uncontrolled, leads to joint destruction secondary to progressive synovitis, ligament instability, joint dislocation or subluxation, and attrition of adjacent tendons either by bony erosion or direct tenosynovial infiltration.
Rheumatoid arthritis is a progressive disease that, if uncontrolled, leads to joint destruction secondary to progressive synovitis, ligament instability, joint dislocation or subluxation, and attrition of adjacent tendons either by bony erosion or direct tenosynovial infiltration.
![]() When tendon rupture occurs on the dorsum of the hand or wrist, patients cannot extend their fingers and have difficulty grasping objects.
When tendon rupture occurs on the dorsum of the hand or wrist, patients cannot extend their fingers and have difficulty grasping objects.
![]() The most common tendon ruptures on the dorsum of the hand begin on the ulnar side and usually are a result of subluxation of the distal radial ulnar joint (DRUJ), the so-called Vaughan-Jackson or caput ulnae syndrome.6
The most common tendon ruptures on the dorsum of the hand begin on the ulnar side and usually are a result of subluxation of the distal radial ulnar joint (DRUJ), the so-called Vaughan-Jackson or caput ulnae syndrome.6
![]() On the volar side of the wrist, the most common tendons to rupture are the flexor pollicis longus and the adjacent flexor digitorum profundus (FDP) tendon to the index finger or possibly the long finger. This is referred to as Mannerfelt syndrome.3
On the volar side of the wrist, the most common tendons to rupture are the flexor pollicis longus and the adjacent flexor digitorum profundus (FDP) tendon to the index finger or possibly the long finger. This is referred to as Mannerfelt syndrome.3
ANATOMY
![]() The extensor tendons of the hand and forearm pass beneath the extensor retinaculum at the wrist. The retinaculum is divided into six separate compartments lined by tenosynovium, which can become involved in the pathology of rheumatoid arthritis.
The extensor tendons of the hand and forearm pass beneath the extensor retinaculum at the wrist. The retinaculum is divided into six separate compartments lined by tenosynovium, which can become involved in the pathology of rheumatoid arthritis.
![]() The first compartment contains the tendons of the abductor pollicis longus and the extensor pollicis brevis. The former tendon often contains multiple slips, which can contribute to limited space in its respective compartment and secondary De Quervain tenosynovitis.
The first compartment contains the tendons of the abductor pollicis longus and the extensor pollicis brevis. The former tendon often contains multiple slips, which can contribute to limited space in its respective compartment and secondary De Quervain tenosynovitis.
![]() The second compartment consists of the extensor carpi radialis longus (ECRL) and brevis (ECRB), the former tendon inserting at the base of the index metacarpal and the latter at the base of the long finger metacarpal.
The second compartment consists of the extensor carpi radialis longus (ECRL) and brevis (ECRB), the former tendon inserting at the base of the index metacarpal and the latter at the base of the long finger metacarpal.
![]() The third compartment contains only the tendon of the extensor pollicis longus (EPL), which passes around the tubercle of Lister at a fairly sharp angle. While frequently involved in tendon ruptures in rheumatoid arthritis, the EPL may also present as an isolated tendon rupture after nondisplaced fractures of the distal radius.
The third compartment contains only the tendon of the extensor pollicis longus (EPL), which passes around the tubercle of Lister at a fairly sharp angle. While frequently involved in tendon ruptures in rheumatoid arthritis, the EPL may also present as an isolated tendon rupture after nondisplaced fractures of the distal radius.
![]() The fourth compartment contains the extensor indicis proprius (EIP) and the extensor digitorum communis (EDC), sending tendons from the common extensor muscle in the forearm to each of the fingers. The EIP is a separate muscle tendon unit located within the fourth compartment. It can be differentiated by its distal muscle belly.
The fourth compartment contains the extensor indicis proprius (EIP) and the extensor digitorum communis (EDC), sending tendons from the common extensor muscle in the forearm to each of the fingers. The EIP is a separate muscle tendon unit located within the fourth compartment. It can be differentiated by its distal muscle belly.
![]() The fifth extensor compartment contains the extensor digiti quinti (EDQ), often consisting of two slips and passing almost directly over the DRUJ.
The fifth extensor compartment contains the extensor digiti quinti (EDQ), often consisting of two slips and passing almost directly over the DRUJ.
![]() The sixth compartment contains only the extensor carpi ulnaris.
The sixth compartment contains only the extensor carpi ulnaris.
![]() On the palmar side of the wrist, the flexor pollicis longus is located most radially and passes over the radiocarpal joint adjacent to the trapeziometacarpal joint of the thumb. The flexor pollicis, along with the median nerve and the profundus and sublimis tendons to each digit, passes beneath the deep transverse carpal ligament and represents the contents of the carpal canal.
On the palmar side of the wrist, the flexor pollicis longus is located most radially and passes over the radiocarpal joint adjacent to the trapeziometacarpal joint of the thumb. The flexor pollicis, along with the median nerve and the profundus and sublimis tendons to each digit, passes beneath the deep transverse carpal ligament and represents the contents of the carpal canal.
![]() Tenosynovial proliferation can exist within the carpal tunnel, arising from the undersurface of the ligament but more commonly proliferating along the tendons themselves.
Tenosynovial proliferation can exist within the carpal tunnel, arising from the undersurface of the ligament but more commonly proliferating along the tendons themselves.
PATHOGENESIS
![]() Tendon rupture on the dorsum of the wrist is usually the result of instability in the DRUJ, leading to secondary subluxation and bony erosion through the capsule of the joint and then the tendon.
Tendon rupture on the dorsum of the wrist is usually the result of instability in the DRUJ, leading to secondary subluxation and bony erosion through the capsule of the joint and then the tendon.
![]() The tendon initially affected is the EDQ. As the carpus supinates and subluxates volarly, causing the distal ulna to be more dorsal, tendons typically rupture sequentially in an ulnar to radial direction.
The tendon initially affected is the EDQ. As the carpus supinates and subluxates volarly, causing the distal ulna to be more dorsal, tendons typically rupture sequentially in an ulnar to radial direction.
![]() The tendons may also be compromised by direct infiltration from the tenosynovium.
The tendons may also be compromised by direct infiltration from the tenosynovium.
![]() While the ulnar tendons are involved most commonly, it is possible for all of the tendons crossing the dorsum of the wrist to rupture, making reconstruction more difficult.
While the ulnar tendons are involved most commonly, it is possible for all of the tendons crossing the dorsum of the wrist to rupture, making reconstruction more difficult.
![]() On the volar side of the wrist, the flexor pollicis longus may become compromised through erosion by osteophytes and rough bony surfaces at the level of the trapeziometacarpal joint of the thumb or the scaphotrapezial articulation. The adjacent profundus tendon to the index and occasionally the long finger can rupture as well.
On the volar side of the wrist, the flexor pollicis longus may become compromised through erosion by osteophytes and rough bony surfaces at the level of the trapeziometacarpal joint of the thumb or the scaphotrapezial articulation. The adjacent profundus tendon to the index and occasionally the long finger can rupture as well.
![]() Tendons of the flexor surface of the wrist and forearm are also subject to rupture via direct tenosynovial infiltration, but this is less common.
Tendons of the flexor surface of the wrist and forearm are also subject to rupture via direct tenosynovial infiltration, but this is less common.
NATURAL HISTORY
![]() Before the advent of treatment for rheumatoid arthritis, the natural history was one of progression. The disease would occasionally “burn itself out,” however, with the radiocarpal joint subluxing in a volar and radial direction, leading to instability and loss of function.
Before the advent of treatment for rheumatoid arthritis, the natural history was one of progression. The disease would occasionally “burn itself out,” however, with the radiocarpal joint subluxing in a volar and radial direction, leading to instability and loss of function.
![]() Also, before the development and routine use of antitumor necrosis factor drugs, patients were occasionally refractory to nonsteroidal medication, corticosteroids, and stronger antiinflammatory drugs such as methotrexate. When these drug combinations failed, proliferative tenosynovitis occasionally occurred on the dorsum of the wrist, leading to direct tendon rupture as a result of tenosynovial ingrowth into the tendon and collagen destruction and rupture (FIG 1).
Also, before the development and routine use of antitumor necrosis factor drugs, patients were occasionally refractory to nonsteroidal medication, corticosteroids, and stronger antiinflammatory drugs such as methotrexate. When these drug combinations failed, proliferative tenosynovitis occasionally occurred on the dorsum of the wrist, leading to direct tendon rupture as a result of tenosynovial ingrowth into the tendon and collagen destruction and rupture (FIG 1).
![]() The worst-case scenario is secondary rupture of all of the finger extensors, with subluxation of the extensor carpi ulnaris volar to the axis of wrist motion such that it becomes more of a wrist flexor and ulnar deviator than a wrist extensor. The radial wrist extensors may also rupture; however, in part as a result of the more robust nature of the tendons themselves, they tend to remain intact even with progressive disease.
The worst-case scenario is secondary rupture of all of the finger extensors, with subluxation of the extensor carpi ulnaris volar to the axis of wrist motion such that it becomes more of a wrist flexor and ulnar deviator than a wrist extensor. The radial wrist extensors may also rupture; however, in part as a result of the more robust nature of the tendons themselves, they tend to remain intact even with progressive disease.

FIG 1 • Exposure of the extensor tendons of the wrist shows proliferative tenosynovitis originating from the tenosynovial lining of the extensor retinaculum. If left unchecked, such proliferative tenosynovitis can contribute to extensor tendon rupture at the level of the wrist.
![]() The French Impressionist painter Pierre Auguste Renoir was said to have had such severe rheumatoid arthritis that in his later years he would tape a brush to his hand to paint.
The French Impressionist painter Pierre Auguste Renoir was said to have had such severe rheumatoid arthritis that in his later years he would tape a brush to his hand to paint.
PATIENT HISTORY AND PHYSICAL FINDINGS
![]() Patients often note a spontaneous loss of finger motion, but there may be minimal swelling and discomfort. Patients occasionally report a snap or twinge of discomfort as the tendon ruptures.
Patients often note a spontaneous loss of finger motion, but there may be minimal swelling and discomfort. Patients occasionally report a snap or twinge of discomfort as the tendon ruptures.
![]() With an extensor tendon rupture, patients cannot actively extend the metacarpophalangeal (MCP) joints of the involved digit.
With an extensor tendon rupture, patients cannot actively extend the metacarpophalangeal (MCP) joints of the involved digit.
![]() In the case of isolated rupture of the extensor digiti quinti, an intact EDC to the small finger may make it difficult to confirm the diagnosis.
In the case of isolated rupture of the extensor digiti quinti, an intact EDC to the small finger may make it difficult to confirm the diagnosis.
![]() The proximal and distal interphalangeal joints of the finger may be extended through the intrinsics even when the extensors are ruptured.
The proximal and distal interphalangeal joints of the finger may be extended through the intrinsics even when the extensors are ruptured.
![]() Wrist flexion should result in MCP joint extension through tenodesis if the extensor tendons are intact. When the finger extensors are ruptured, this tenodesis effect is absent (FIG 2A,B).
Wrist flexion should result in MCP joint extension through tenodesis if the extensor tendons are intact. When the finger extensors are ruptured, this tenodesis effect is absent (FIG 2A,B).
![]() On the volar side of the wrist, the examiner should check closely for the possibility of associated tenosynovial proliferation proximal and deep to the transverse carpal ligament.
On the volar side of the wrist, the examiner should check closely for the possibility of associated tenosynovial proliferation proximal and deep to the transverse carpal ligament.
![]() Active digital motion may cause palpable crepitance at this level.
Active digital motion may cause palpable crepitance at this level.
![]() Such proliferation may result in coexisting carpal tunnel syndrome (CTS). The examiner should question the patient regarding symptoms of CTS and should assess for signs of CTS.
Such proliferation may result in coexisting carpal tunnel syndrome (CTS). The examiner should question the patient regarding symptoms of CTS and should assess for signs of CTS.
![]() The patient should also be examined carefully for active flexion at the distal interphalangeal joints of the index and long fingers as well as the interphalangeal joint of the thumb.
The patient should also be examined carefully for active flexion at the distal interphalangeal joints of the index and long fingers as well as the interphalangeal joint of the thumb.
![]() Absence of flexion should alert the surgeon to the possibility of rupture of the flexor pollicis longus and the FDP to the index and occasionally the long finger.
Absence of flexion should alert the surgeon to the possibility of rupture of the flexor pollicis longus and the FDP to the index and occasionally the long finger.
![]() These tendons are particularly vulnerable when subluxation and spur formation are present at the trapeziometacarpal or scaphotrapezial joints as well as the volar radiocarpal joint.
These tendons are particularly vulnerable when subluxation and spur formation are present at the trapeziometacarpal or scaphotrapezial joints as well as the volar radiocarpal joint.
![]() Tendon rupture at this level is referred to as Mannerfelt syndrome (FIG 2C) and needs to be differentiated from an anterior interosseous nerve palsy.
Tendon rupture at this level is referred to as Mannerfelt syndrome (FIG 2C) and needs to be differentiated from an anterior interosseous nerve palsy.
![]() Direct pressure on the flexor pollicis longus muscle in the forearm should lead to passive flexion in the interphalangeal joint of the thumb if the tendon is intact.
Direct pressure on the flexor pollicis longus muscle in the forearm should lead to passive flexion in the interphalangeal joint of the thumb if the tendon is intact.
![]() The tenodesis test also is effective for the flexor pollicis longus and profundus and sublimis tendons to the fingers; however, in patients with progressive rheumatoid arthritis, the radiocarpal joint and the interphalangeal joints may become arthritic, making passive motion of the wrist and fingers somewhat more difficult and therefore the test more unreliable.
The tenodesis test also is effective for the flexor pollicis longus and profundus and sublimis tendons to the fingers; however, in patients with progressive rheumatoid arthritis, the radiocarpal joint and the interphalangeal joints may become arthritic, making passive motion of the wrist and fingers somewhat more difficult and therefore the test more unreliable.
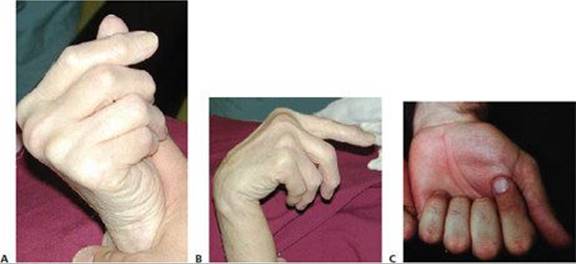
FIG 2 • A. Passive wrist extension results in passive finger flexion with intact finger flexors. B. Passive wrist flexion should result in passive finger extension when the finger extensor tendons are intact. In this situation, however, those tendons are not intact and passive wrist flexion results in the long, ring, and small extensor fingers remaining in a flexed position. C. In a patient with Mannerfelt syndrome, attempted active flexion of the thumb and fingers results in absent flexion of the interphalangeal joint of the thumb and in this situation the distal interphalangeal joint of the index finger. Clinically this is similar to anterior interosseous nerve syndrome and must be distinguished clinically and often by electromyography.

FIG 3 • AP radiograph of the wrist of the patient in Figure 4 shows osteophyte formation in the distal radioulnar joint (arrow). (From Lubahn JD, Wolfe TL. Surgical treatment and rehabilitation and tendon ruptures in the rheumatoid hand. In: Mackin EJ, Callahan AD, Skirven TM, et al, eds. Rehabilitation of the Hand and Upper Extremity, ed 5. St. Louis: Mosby, 2002:1598–1607.)
IMAGING AND OTHER DIAGNOSTIC STUDIES
![]() AP and lateral radiographs of the hand and wrist should be obtained to look for subtle changes of the DRUJ, such as subluxation or a small osteophyte (FIG 3), which may be consistent with the physical findings of tendon rupture (FIG 4).
AP and lateral radiographs of the hand and wrist should be obtained to look for subtle changes of the DRUJ, such as subluxation or a small osteophyte (FIG 3), which may be consistent with the physical findings of tendon rupture (FIG 4).
![]() Similar attention should be paid to the volar surface of the radiocarpal joint and the trapeziometacarpal joint of the thumb as well as the scaphotrapezial and trapezoidal joints.
Similar attention should be paid to the volar surface of the radiocarpal joint and the trapeziometacarpal joint of the thumb as well as the scaphotrapezial and trapezoidal joints.
![]() Radiographs may reveal arthrosis and deformity in the digits themselves responsible for motion loss.
Radiographs may reveal arthrosis and deformity in the digits themselves responsible for motion loss.

FIG 4 • The clinical consequences of a spur in the distal radioulnar joint: rupture of the extensor digiti quinti and extensor digitorum communis to the ring and small fingers. When the patient attempts to actively extend the fingers, the ring and small finger remain flexed. (From Lubahn JD, Wolfe TL. Surgical treatment and rehabilitation and tendon ruptures in the rheumatoid hand. In: Mackin EJ, Callahan AD, Skirven TM, et al, eds. Rehabilitation of the Hand and Upper Extremity, ed 5. St. Louis: Mosby, 2002:1598–1607.)
![]() Radiographs of the cervical spine may reveal subluxation, possibly causing nerve compression and secondary digital motion loss or weakness.
Radiographs of the cervical spine may reveal subluxation, possibly causing nerve compression and secondary digital motion loss or weakness.
![]() CT and MRI are not routinely needed.
CT and MRI are not routinely needed.
![]() Electromyography and nerve conduction studies are crucial in the evaluation of the patient with potential tendon ruptures, particularly if tenodesis testing is normal in the face of a loss of active finger extension or flexion.
Electromyography and nerve conduction studies are crucial in the evaluation of the patient with potential tendon ruptures, particularly if tenodesis testing is normal in the face of a loss of active finger extension or flexion.
![]() Compression of both the anterior interosseous and posterior interosseous nerves can occur in rheumatoid arthritis, usually secondary to ganglion cyst formation at the level of the elbow joint.
Compression of both the anterior interosseous and posterior interosseous nerves can occur in rheumatoid arthritis, usually secondary to ganglion cyst formation at the level of the elbow joint.
DIFFERENTIAL DIAGNOSIS
![]() In the case of tendon ruptures on the dorsum of the hand and wrist, the differential diagnosis is primarily with that of posterior interosseous nerve compression or posterior interosseous nerve syndrome.
In the case of tendon ruptures on the dorsum of the hand and wrist, the differential diagnosis is primarily with that of posterior interosseous nerve compression or posterior interosseous nerve syndrome.
![]() Compression of the posterior interosseous branch of the radial nerve, or the radial nerve itself more proximally, needs to be considered as the cause of the patient's inability to extend the fingers. Diagnosis can be suspected by history and clinical examination. Electrophysiologic testing may also prove helpful.
Compression of the posterior interosseous branch of the radial nerve, or the radial nerve itself more proximally, needs to be considered as the cause of the patient's inability to extend the fingers. Diagnosis can be suspected by history and clinical examination. Electrophysiologic testing may also prove helpful.
![]() Cervical disc disease or rheumatoid arthritis of the cervical spine with subluxation or instability may also be the cause for weakness of the finger or wrist extensors, and the cervical spine should also be imaged.
Cervical disc disease or rheumatoid arthritis of the cervical spine with subluxation or instability may also be the cause for weakness of the finger or wrist extensors, and the cervical spine should also be imaged.
![]() With respect to Mannerfelt syndrome, absence of flexion at the interphalangeal joint of the thumb and the distal interphalangeal joints in the index and long fingers should be differentiated from the anterior interosseous nerve syndrome, which when present in rheumatoid arthritis is usually due to a large ganglion originating on the volar surface of the elbow.
With respect to Mannerfelt syndrome, absence of flexion at the interphalangeal joint of the thumb and the distal interphalangeal joints in the index and long fingers should be differentiated from the anterior interosseous nerve syndrome, which when present in rheumatoid arthritis is usually due to a large ganglion originating on the volar surface of the elbow.
NONOPERATIVE MANAGEMENT
![]() Nonoperative management probably is more feasible with respect to Mannerfelt syndrome than with the Vaughn-Jackson or caput ulnae syndrome. While the functional deficit is generally greater with loss of finger extensors than loss of active flexion of the interphalangeal joint of the thumb and distal interphalangeal joints of the index and long fingers, some patients may still function remarkably well.
Nonoperative management probably is more feasible with respect to Mannerfelt syndrome than with the Vaughn-Jackson or caput ulnae syndrome. While the functional deficit is generally greater with loss of finger extensors than loss of active flexion of the interphalangeal joint of the thumb and distal interphalangeal joints of the index and long fingers, some patients may still function remarkably well.
![]() Supportive measures in patients who for one reason or another are not deemed suitable surgical candidates may be provided by a certified hand therapist or occupational therapist able to assist the patient with his or her activities of daily living.
Supportive measures in patients who for one reason or another are not deemed suitable surgical candidates may be provided by a certified hand therapist or occupational therapist able to assist the patient with his or her activities of daily living.
![]() With median nerve entrapment and compression from the proliferative tenosynovitis at the level of the radiocarpal joint, disability becomes more progressive and nonsurgical treatment more difficult. There may be a role for corticosteroid injection at the level of the radiocarpal joint, and certainly referral to a rheumatologist is crucial for the control and management of the disease before any surgical intervention.
With median nerve entrapment and compression from the proliferative tenosynovitis at the level of the radiocarpal joint, disability becomes more progressive and nonsurgical treatment more difficult. There may be a role for corticosteroid injection at the level of the radiocarpal joint, and certainly referral to a rheumatologist is crucial for the control and management of the disease before any surgical intervention.
![]() In the case of wrist or finger extensor tendon rupture, nonsurgical treatment may be beneficial in terms of resting the radiocarpal joint and interphalangeal joints of the fingers to prevent further tendon rupture by attrition. Splinting the wrist or hand may prove beneficial, particularly if motion in the radiocarpal joint or fingers is painful.
In the case of wrist or finger extensor tendon rupture, nonsurgical treatment may be beneficial in terms of resting the radiocarpal joint and interphalangeal joints of the fingers to prevent further tendon rupture by attrition. Splinting the wrist or hand may prove beneficial, particularly if motion in the radiocarpal joint or fingers is painful.
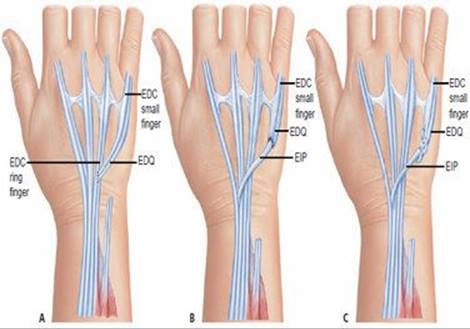
FIG 5 • A. When extensor tendon rupture leads to loss of extension in only one digit, such as the small finger, end-to-side transfer of the distal ruptured tendon to the more proximal, adjacent extensor digitorum communis tendon of the ring finger can be performed. B. If the ruptured end is distal to the mid-metacarpal region, this transfer may lead to abduction of the small finger metacarpal, and under these circumstances, tendon transfer of the extensor indicis proprius to the distal stump of the extensor digiti quinti is undertaken (depicted here as an end-to-end transfer). C. Extensor indicis proprius to extensor digiti quinti, depicted here as a Pulvertaft weave between the distal tendon and the proximal transferred extensor indicis proprius.
SURGICAL MANAGEMENT
Extensor Tendon Rupture
![]() A variety of tendon transfers are available for reconstruction of single and multiple extensor tendon ruptures.
A variety of tendon transfers are available for reconstruction of single and multiple extensor tendon ruptures.
![]() It is important for the surgeon to locate the site of tendon rupture, and identify as well as treat the cause.
It is important for the surgeon to locate the site of tendon rupture, and identify as well as treat the cause.
![]() Usually, rupture is secondary to the distal ulna subluxing dorsally through the attenuated fibers of the DRUJ. When subluxation occurs at this level, it erodes through the floor of the fourth and fifth extensor compartments.
Usually, rupture is secondary to the distal ulna subluxing dorsally through the attenuated fibers of the DRUJ. When subluxation occurs at this level, it erodes through the floor of the fourth and fifth extensor compartments.
![]() Tendon reconstruction is therefore not complete unless it involves removal of the dorsal osteophyte by a modified Darrach procedure and coverage of the distal ulna with a flap of extensor retinaculum.
Tendon reconstruction is therefore not complete unless it involves removal of the dorsal osteophyte by a modified Darrach procedure and coverage of the distal ulna with a flap of extensor retinaculum.
![]() When the distal ulna is unstable, the pronator quadratus may be brought dorsal to stabilize the bone.
When the distal ulna is unstable, the pronator quadratus may be brought dorsal to stabilize the bone.
![]() Small finger extension loss
Small finger extension loss
![]() Single tendon rupture of the EDQ may go unnoticed, particularly if there is a strong EDC to the small finger. Often, however, this common extensor to the small finger is hypoplastic or absent and all that is present is a juctura tendinae from the small finger to the adjacent ring finger. Isolated loss of function in the EDQ is manifest by weakness or lack of extension of the small finger.
Single tendon rupture of the EDQ may go unnoticed, particularly if there is a strong EDC to the small finger. Often, however, this common extensor to the small finger is hypoplastic or absent and all that is present is a juctura tendinae from the small finger to the adjacent ring finger. Isolated loss of function in the EDQ is manifest by weakness or lack of extension of the small finger.
![]() The distal stump of the ruptured tendon is sewn end to side to the intact ring finger EDC tendon. The risk of this transfer, however, is excessive abduction of the small finger when the distal tendon is short (FIG 5A).
The distal stump of the ruptured tendon is sewn end to side to the intact ring finger EDC tendon. The risk of this transfer, however, is excessive abduction of the small finger when the distal tendon is short (FIG 5A).
![]() Alternatively, an EIP transfer may be performed (FIG 5B,C).
Alternatively, an EIP transfer may be performed (FIG 5B,C).
![]() Ring and small finger extension loss (Fig 4)
Ring and small finger extension loss (Fig 4)
![]() In addition to the EDC tendons to the ring and small fingers, the EDQ usually will have ruptured.
In addition to the EDC tendons to the ring and small fingers, the EDQ usually will have ruptured.
![]() The EIP is transferred to the EDQ.
The EIP is transferred to the EDQ.
![]() The distal ring finger EDC tendon is transferred end to side to the adjacent intact long finger EDC tendon (FIG 6).
The distal ring finger EDC tendon is transferred end to side to the adjacent intact long finger EDC tendon (FIG 6).
![]() Long and ring finger extension loss (FIG 7A)
Long and ring finger extension loss (FIG 7A)
![]() Although two fingers are seemingly involved, the EDC tendon to the small finger is usually ruptured as well. The EDQ remains intact.
Although two fingers are seemingly involved, the EDC tendon to the small finger is usually ruptured as well. The EDQ remains intact.
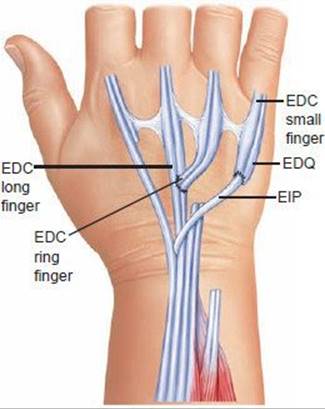
FIG 6 • In cases of double rupture in the ring and small fingers, transfer of the extensor indicis proprius to the distal extensor digiti quinti, with end-to-side transfer of the distal extensor digitorum communis of the ring finger to the adjacent extensor digitorum communis to the long finger, is a standard transfer.
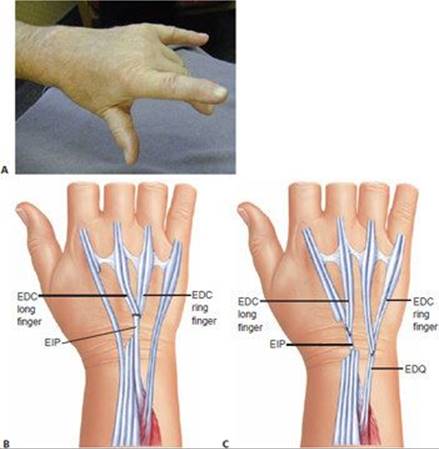
FIG 7 • A. Clinical appearance of a hand with rupture of the extensor digitorum communis (EDC) to the long and ring fingers. (From Lubahn JD, Wolfe TL. Surgical treatment and rehabilitation and tendon ruptures in the rheumatoid hand. In: Mackin EJ, Callahan AD, Skirven TM, et al, eds. Rehabilitation of the Hand and Upper Extremity, ed 5. St. Louis, Mosby, 2002:1598–1607.) B. Optional tendon transfer when the EDC to the index finger is intact is transfer of the extensor indicis proprius (EIP) to the distal stumps of the long and ring fingers. C. When the EDC to the index finger has been ruptured and EIP transfer is not an option, transfer of the distal EDC of the long finger to the adjacent EIP of the index, and transfer of the distal ring EDC to the adjacent small finger extensor, is shown here. (B,C from Williams DP, Lubahn JD. Reconstruction of extensor tendons. Atlas Hand Clin 2005;10:209–222.)
![]() If the index finger EDC tendon is intact, EIP transfer to the long and ring finger EDC tendons is performed (FIG 7B).
If the index finger EDC tendon is intact, EIP transfer to the long and ring finger EDC tendons is performed (FIG 7B).
![]() If the EDC tendon to the index finger has ruptured, endto-side transfer of the distal tendon of the long finger EDC to the adjacent intact EIP and transfer of the distal tendon of the ring finger EDC to the adjacent intact EDQ may be considered (FIG 7C).
If the EDC tendon to the index finger has ruptured, endto-side transfer of the distal tendon of the long finger EDC to the adjacent intact EIP and transfer of the distal tendon of the ring finger EDC to the adjacent intact EDQ may be considered (FIG 7C).
![]() Long, ring, and small finger extension loss
Long, ring, and small finger extension loss
![]() If the EIP and EDC tendons to the index finger are intact, the EIP can be transferred to the distal stumps of the ring and small finger EDC tendons using end-to-end or end-to-side techniques, depending on the length of the distal stumps.
If the EIP and EDC tendons to the index finger are intact, the EIP can be transferred to the distal stumps of the ring and small finger EDC tendons using end-to-end or end-to-side techniques, depending on the length of the distal stumps.
![]() The EDC to the long finger is transferred end to side to the adjacent intact index EDC tendon (FIG 8).
The EDC to the long finger is transferred end to side to the adjacent intact index EDC tendon (FIG 8).
![]() If only the EIP is intact and all remaining tendons on the dorsum of the wrist have ruptured, transfer of the flexor digitorum sublimis (FDS) of the ring finger around the radial or ulnar border of the forearm is the next logical choice.
If only the EIP is intact and all remaining tendons on the dorsum of the wrist have ruptured, transfer of the flexor digitorum sublimis (FDS) of the ring finger around the radial or ulnar border of the forearm is the next logical choice.
![]() In patients with partial or complete wrist fusion, or in patients with limited wrist motion, transfer of the ECRL may be considered. Although not “in phase” with the finger extension, the line of pull matches reasonably well.
In patients with partial or complete wrist fusion, or in patients with limited wrist motion, transfer of the ECRL may be considered. Although not “in phase” with the finger extension, the line of pull matches reasonably well.
![]() Index, long, ring, and small finger extension loss
Index, long, ring, and small finger extension loss
![]() The two most common transfers are the FDS around the radial and ulnar sides of the forearm or through the interosseous membrane (FIG 9A,B).
The two most common transfers are the FDS around the radial and ulnar sides of the forearm or through the interosseous membrane (FIG 9A,B).
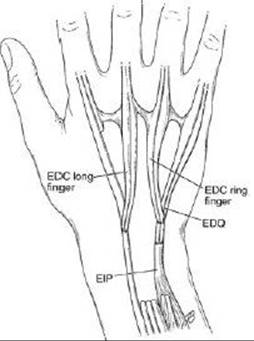
FIG 8 • Rupture of the common extensors to the long, ring, and small fingers with extensor digiti quinti rupture can be treated, as shown here, with transfer of the extensor indicis proprius to the distal stumps of the ring and small finger with distal endto-side transfer from the extensor digitorum communis to the long finger to the adjacent index extensor digitorum communis.
![]() Transfer of one of the radial wrist extensors is a suitable alternative (FIG 9C).
Transfer of one of the radial wrist extensors is a suitable alternative (FIG 9C).
![]() Loss of thumb extension
Loss of thumb extension
![]() EPL rupture is common and often results in minimal loss of function.
EPL rupture is common and often results in minimal loss of function.
![]() If diagnosed early, an interposition graft may be used.2 The palmaris tendon, a strip of the flexor carpi radialis, and a slip of the EDQ are suitable choices.
If diagnosed early, an interposition graft may be used.2 The palmaris tendon, a strip of the flexor carpi radialis, and a slip of the EDQ are suitable choices.
![]() Late or chronic ruptures require transfer of the EIP to the distal end of the EPL. The proximal muscle will usually begin to atrophy and become nonfunctional by 6 months after the injury.
Late or chronic ruptures require transfer of the EIP to the distal end of the EPL. The proximal muscle will usually begin to atrophy and become nonfunctional by 6 months after the injury.
![]() If the EIP is not available, transfer of the FDS from the long or ring finger can be considered. The FDS can be routed through the interosseous membrane or around the radial side of the forearm as described for transfer to restore finger extension.7
If the EIP is not available, transfer of the FDS from the long or ring finger can be considered. The FDS can be routed through the interosseous membrane or around the radial side of the forearm as described for transfer to restore finger extension.7
![]() Chronic synovitis at the thumb MCP joint may lead to attritional rupture of the dorsal capsule and the extensor pollicis brevis.
Chronic synovitis at the thumb MCP joint may lead to attritional rupture of the dorsal capsule and the extensor pollicis brevis.
![]() This boutonnière deformity of the thumb is a type I as described by Nalebuff4 and Nalebuff and Millender5 (FIG 10).
This boutonnière deformity of the thumb is a type I as described by Nalebuff4 and Nalebuff and Millender5 (FIG 10).
![]() The deformity usually progresses after extensor pollicis brevis rupture. The EPL shifts ulnarward, the collateral ligaments weaken, and the thumb metacarpal becomes abducted radially. The interphalangeal joint hyperextends as a reciprocal response to the MCP joint flexion.
The deformity usually progresses after extensor pollicis brevis rupture. The EPL shifts ulnarward, the collateral ligaments weaken, and the thumb metacarpal becomes abducted radially. The interphalangeal joint hyperextends as a reciprocal response to the MCP joint flexion.
![]() Transfer of the EPL to the extensor pollicis brevis and dorsal capsule is performed. Local anesthesia is typically adequate.
Transfer of the EPL to the extensor pollicis brevis and dorsal capsule is performed. Local anesthesia is typically adequate.
Flexor Tendon Rupture
![]() Tendon transfer for the treatment of flexor tendon disruption in the rheumatoid patient is much less common than for extensor tendon rupture.
Tendon transfer for the treatment of flexor tendon disruption in the rheumatoid patient is much less common than for extensor tendon rupture.
![]() Mannerfelt syndrome should be treated by transfer of the brachioradialis tendon to the flexor pollicis longus.
Mannerfelt syndrome should be treated by transfer of the brachioradialis tendon to the flexor pollicis longus.
![]() Associated disruption of a FDP tendon is usually treated by transferring the distal stump end to side to the adjacent digit's FDP tendon.
Associated disruption of a FDP tendon is usually treated by transferring the distal stump end to side to the adjacent digit's FDP tendon.
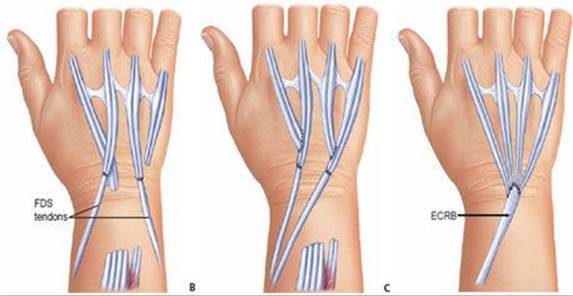
FIG 9 • A. Rupture of all four finger extensors may be treated alternatively with transfer of the flexor digitorum superficialis (FDS) to the long and ring fingers, harvested in the distal palm and transferred around the radius and ulna, with the two forearm bones serving as pulleys for the transferred tendon. B. Alternatively, both FDS tendons may be transferred around the radial side of the forearm and sutured to the distal stumps of the extensor digitorum communis tendons. C. With rupture of all common extensor tendons to the fingers as well as the extensor indicis proprius and the extensor digiti quinti, extension may be restored through transfer of one of the radial wrist extensors. This is ideal when a partial wrist fusion is being planned, as shown.

FIG 10 • Extensor pollicis brevis rupture. Boutonnière deformity of the thumb (Nalebuff type I).
Preoperative Planning
![]() All patients with rheumatoid arthritis require a thorough general physical examination as well as careful evaluation of their cervical spine, including posteroanterior and lateral radiographs, often with flexion and extension views to evaluate cervical spine instability.
All patients with rheumatoid arthritis require a thorough general physical examination as well as careful evaluation of their cervical spine, including posteroanterior and lateral radiographs, often with flexion and extension views to evaluate cervical spine instability.
![]() Review the patients medication with their Rheumatologist, consider withholding some Anti Tumor Necrosis Factor drugs for the week of surgery.
Review the patients medication with their Rheumatologist, consider withholding some Anti Tumor Necrosis Factor drugs for the week of surgery.
![]() Limited joint mobility is a contraindication to tendon transfer.
Limited joint mobility is a contraindication to tendon transfer.
![]() Brachioradialis tendon transfer to the flexor pollicis longus is an ideal transfer and is likely to yield an excellent result, but only if there is adequate passive motion at the interphalangeal joint and MCP joint as well as the basal joint and the thumb. If these joints are stiff, the brachioradialis might be better saved for other needs as the patient's arthritis progresses.
Brachioradialis tendon transfer to the flexor pollicis longus is an ideal transfer and is likely to yield an excellent result, but only if there is adequate passive motion at the interphalangeal joint and MCP joint as well as the basal joint and the thumb. If these joints are stiff, the brachioradialis might be better saved for other needs as the patient's arthritis progresses.
![]() The carpus should be examined for stability. In particular, the DRUJ on the ulnar side of the wrist should be checked for dorsal instability and subluxation and the volar, radial side of the wrist for palmar subluxation.
The carpus should be examined for stability. In particular, the DRUJ on the ulnar side of the wrist should be checked for dorsal instability and subluxation and the volar, radial side of the wrist for palmar subluxation.
![]() Planning needs to take into consideration the results of preoperative radiographs of the wrist, hand, and cervical spine as well as electromyographic tests.
Planning needs to take into consideration the results of preoperative radiographs of the wrist, hand, and cervical spine as well as electromyographic tests.
![]() If the findings on electromyography are negative and the surgeon is certain that tendon rupture is responsible for the lack of active finger motion, plans should be made to transfer expendable existing tendons to those that have ruptured. In the case of multiple extensor tendon ruptures to the fingers, the ECRL and the FDS from the long and ring fingers are two of the most common donor tendons.
If the findings on electromyography are negative and the surgeon is certain that tendon rupture is responsible for the lack of active finger motion, plans should be made to transfer expendable existing tendons to those that have ruptured. In the case of multiple extensor tendon ruptures to the fingers, the ECRL and the FDS from the long and ring fingers are two of the most common donor tendons.
![]() If radiographs reveal significant joint destruction and instability, appropriate arthrodesis or arthroplasty should be considered rather than tendon transfer.
If radiographs reveal significant joint destruction and instability, appropriate arthrodesis or arthroplasty should be considered rather than tendon transfer.
![]() Instruments and suture needed for tendon weaves and repairs are extremely valuable.
Instruments and suture needed for tendon weaves and repairs are extremely valuable.
![]() Sharp tendon passers facilitate a Pulvertaft weave. When sharp, pointed tendon passers are not available, a no. 11 blade can be passed through the tendon followed by a hemostat to grasp the knife and guide the hemostat through the tendon. The hemostat then grasps the transferred tendon, weaving it through the recipient tendon.
Sharp tendon passers facilitate a Pulvertaft weave. When sharp, pointed tendon passers are not available, a no. 11 blade can be passed through the tendon followed by a hemostat to grasp the knife and guide the hemostat through the tendon. The hemostat then grasps the transferred tendon, weaving it through the recipient tendon.
![]() 3-0 and 4-0 braided nonabsorbable sutures on appropriate needles are required for tendon repairs.
3-0 and 4-0 braided nonabsorbable sutures on appropriate needles are required for tendon repairs.
Positioning
![]() Most tendon transfers are done with the patient in the supine position on the operating table.
Most tendon transfers are done with the patient in the supine position on the operating table.
![]() The contralateral arm or lower extremity may be sterilely draped in the event that a tendon graft is needed.
The contralateral arm or lower extremity may be sterilely draped in the event that a tendon graft is needed.
![]() Anesthesia may be either general or an axillary block, depending on the patient's preference and the stability of the cervical spine.
Anesthesia may be either general or an axillary block, depending on the patient's preference and the stability of the cervical spine.
TECHNIQUS
EXTENSOR INDICIS PROPRIUS TENDON TRANSFER
![]() Isolate the EIP through a 1-cm longitudinal or curvilinear incision on the dorsal ulnar aspect of the index MCP joint.
Isolate the EIP through a 1-cm longitudinal or curvilinear incision on the dorsal ulnar aspect of the index MCP joint.
![]() The EIP is usually the ulnar tendon of the two located dorsal to the MCP joint of the index finger.
The EIP is usually the ulnar tendon of the two located dorsal to the MCP joint of the index finger.
![]() Make a second 2-to 3-cm incision over the mid-dorsal wrist (unless a dorsal wrist incision has already been made for another procedure).
Make a second 2-to 3-cm incision over the mid-dorsal wrist (unless a dorsal wrist incision has already been made for another procedure).
![]() Incise the retinaculum overlying the fourth extensor compartment and locate the EIP tendon ulnar and deep to the EDC tendons.
Incise the retinaculum overlying the fourth extensor compartment and locate the EIP tendon ulnar and deep to the EDC tendons.
![]() The EIP muscle belly is the most distal in the fourth extensor compartment.
The EIP muscle belly is the most distal in the fourth extensor compartment.
![]() Once the identity of the EIP is confirmed proximally and distally, suture the index EIP and EDC tendons together as far distal as possible using 4-0 nonabsorbable, usually braided nylon, suture.
Once the identity of the EIP is confirmed proximally and distally, suture the index EIP and EDC tendons together as far distal as possible using 4-0 nonabsorbable, usually braided nylon, suture.
![]() Invert or bury the knot to void prominence under thin rheumatoid skin.
Invert or bury the knot to void prominence under thin rheumatoid skin.
![]() Incise the EIP just proximal to the stitch, then free any tendinous interconnections over the dorsum of the hand.
Incise the EIP just proximal to the stitch, then free any tendinous interconnections over the dorsum of the hand.
![]() Use a blunt instrument or Penrose drain to pull the EIP tendon into the wrist wound.
Use a blunt instrument or Penrose drain to pull the EIP tendon into the wrist wound.
![]() Transfer the EIP to the exposed recipient tendon using a Pulvertaft weave.
Transfer the EIP to the exposed recipient tendon using a Pulvertaft weave.
![]() A single weave, while usually sufficient for smaller tendons, should be supplemented with an additional one or two weaves if possible. This will significantly strengthen the repair site.
A single weave, while usually sufficient for smaller tendons, should be supplemented with an additional one or two weaves if possible. This will significantly strengthen the repair site.
![]() If insufficient distal tendon is present for a weave, either an end-to-end repair or a weave in which the transferred tendon is brought through a transverse incision in the distal recipient stump from volar to dorsal is an effective option.
If insufficient distal tendon is present for a weave, either an end-to-end repair or a weave in which the transferred tendon is brought through a transverse incision in the distal recipient stump from volar to dorsal is an effective option.
![]() Skin incisions are closed and a splint is applied.
Skin incisions are closed and a splint is applied.
FLEXOR DIGITORUM SUPERFICIALIS TENDON TRANSFER
![]() In the case of rupture of all of the extensor tendons on the dorsum of the wrist, and when wrist motion is still intact, tendon transfer of the FDS, as suggested by Boyes,1 is a reliable method to restore finger extension.
In the case of rupture of all of the extensor tendons on the dorsum of the wrist, and when wrist motion is still intact, tendon transfer of the FDS, as suggested by Boyes,1 is a reliable method to restore finger extension.
![]() The FDS and FDP to each of the donor fingers must be intact.
The FDS and FDP to each of the donor fingers must be intact.
![]() Pre-existing swan-neck deformity in a donor digit may worsen after harvest of the FDS tendon.
Pre-existing swan-neck deformity in a donor digit may worsen after harvest of the FDS tendon.
![]() Long and ring FDS tendons are used most often.
Long and ring FDS tendons are used most often.

TECH FIG 1 • Transfer of the flexor digitorum sublimis to the long and ring fingers. The distal incision in the palm is used to isolate the sublimis tendon as far distal as possible by flexing the finger so that the chiasm of Camper is visible in the wound. The tendon is divided just proximal to the chiasm, leaving enough distal tendon to contribute to the stability of the proximal interphalangeal joint in extension and thereby avoiding a secondary instability of that joint and possible swan-neck deformity.
![]() Make a transverse incision in the distal palm and divide the FDS tendon proximal to the bifurcation, leaving the chiasm of Camper intact to provide proximal interphalangeal stability and help prevent development of a swan-neck deformity (TECH FIG 1).
Make a transverse incision in the distal palm and divide the FDS tendon proximal to the bifurcation, leaving the chiasm of Camper intact to provide proximal interphalangeal stability and help prevent development of a swan-neck deformity (TECH FIG 1).
![]() Splinting the proximal interphalangeal joint in flexion postoperatively will also help to minimize the risk of developing a swan-neck deformity.
Splinting the proximal interphalangeal joint in flexion postoperatively will also help to minimize the risk of developing a swan-neck deformity.
![]() Isolate the FDS tendon proximally through a Henry-type incision in the distal forearm and atraumatically deliver it into that incision.
Isolate the FDS tendon proximally through a Henry-type incision in the distal forearm and atraumatically deliver it into that incision.
![]() Pass the tendon deep to the median nerve, the FDP, the flexor carpi radialis, the flexor pollicis longus, and the radial artery and the nerve at the wrist with a blunt tendon passer, hemostat, or Kelly clamp.
Pass the tendon deep to the median nerve, the FDP, the flexor carpi radialis, the flexor pollicis longus, and the radial artery and the nerve at the wrist with a blunt tendon passer, hemostat, or Kelly clamp.
![]() The transferred tendon sits on the radius using the bone as a pulley to enhance the effectiveness of the transfer.
The transferred tendon sits on the radius using the bone as a pulley to enhance the effectiveness of the transfer.
![]() If the FDS to the ring finger is too short to pass around the radial side of the wrist, an alternative route is beneath the FDP, flexor carpi ulnaris, and ulnar artery and nerve around the ulnar side of the forearm using the ulna as the pulley.
If the FDS to the ring finger is too short to pass around the radial side of the wrist, an alternative route is beneath the FDP, flexor carpi ulnaris, and ulnar artery and nerve around the ulnar side of the forearm using the ulna as the pulley.
![]() In general the radial path is preferred to minimize ulnar deviation of the digits.
In general the radial path is preferred to minimize ulnar deviation of the digits.
![]() Alternatively, the FDS tendon is passed volar to dorsal though an incision in the interosseous membrane just proximal to the DRUJ.
Alternatively, the FDS tendon is passed volar to dorsal though an incision in the interosseous membrane just proximal to the DRUJ.
![]() The membrane functions as the pulley.
The membrane functions as the pulley.
![]() Weave the smaller distal tendon stumps through the larger transferred FDS tendon in the manner described by Pulvertaft.
Weave the smaller distal tendon stumps through the larger transferred FDS tendon in the manner described by Pulvertaft.
![]() Adjust tension such that with slight wrist flexion, the fingers are maintained in full extension.
Adjust tension such that with slight wrist flexion, the fingers are maintained in full extension.
![]() Immobilize the hand and wrist with the wrist in 40 degrees of extension and the fingers flexed until tension is noted at the suture line (TECH FIG 2).
Immobilize the hand and wrist with the wrist in 40 degrees of extension and the fingers flexed until tension is noted at the suture line (TECH FIG 2).
![]() Ideally, this should be close to the “safe position” with slight MCP joint flexion and relative interphalangeal joint extension.
Ideally, this should be close to the “safe position” with slight MCP joint flexion and relative interphalangeal joint extension.

TECH FIG 2 • The ideal splint for transfer to the extensor tendons of the finger immobilizes the wrist in the so-called safe position. With wrist extension, tension at the site of transfer is usually minimal. Finger flexion at the metacarpophalangeal joint is ideal to prevent scarring of the collateral ligaments and secondary loss of finger flexion. The amount of flexion possible is judged in the operating room by passive flexion of the finger until a minimum amount of tension is seen at the repair site. (From Williams DP, Lubahn JD. Reconstruction of extensor tendons. Atlas Hand Clin 2005;10:209–222.)
EXTENSOR CARPI RADIALIS LONGUS OR BREVIS TRANSFER
![]() When all of the finger extensors have ruptured, wrist motion is severely limited (ie, after a partial or complete wrist fusion), and the radiocarpal joint is stable, the wrist extensors become potential muscles for use as transfers.
When all of the finger extensors have ruptured, wrist motion is severely limited (ie, after a partial or complete wrist fusion), and the radiocarpal joint is stable, the wrist extensors become potential muscles for use as transfers.
![]() The ECRL and the ECRB are located in the second dorsal compartment of the wrist adjacent to the fourth compartment and are separated only by the tubercle of Lister and the EPL.
The ECRL and the ECRB are located in the second dorsal compartment of the wrist adjacent to the fourth compartment and are separated only by the tubercle of Lister and the EPL.
![]() Expose the ECRL or ECRB using a straight dorsal incision or a limited transverse incision over the base of the index and long metacarpals, at their respective insertion sites.
Expose the ECRL or ECRB using a straight dorsal incision or a limited transverse incision over the base of the index and long metacarpals, at their respective insertion sites.
![]() Divide the tendon selected for transfer, usually the ECRL, at its insertion and transfer it ulnarward to the recipient tendon stump.
Divide the tendon selected for transfer, usually the ECRL, at its insertion and transfer it ulnarward to the recipient tendon stump.
BRACHIORADIALIS TENDON TRANSFER (RECONSTRUCTION OF MANNERFELT SYNDROME)
![]() Expose the forearm muscles and the brachioradialis tendon insertion on the distal radial aspect of the radius through a Henry-type incision.
Expose the forearm muscles and the brachioradialis tendon insertion on the distal radial aspect of the radius through a Henry-type incision.
![]() Confirm the tendon rupture by direct exposure of the slightly more distal and radial tendon of the flexor pollicis longus.
Confirm the tendon rupture by direct exposure of the slightly more distal and radial tendon of the flexor pollicis longus.
![]() Mobilize the distal tendon stump and perform a tenolysis to remove adhesions.
Mobilize the distal tendon stump and perform a tenolysis to remove adhesions.
![]() Weave the distal flexor pollicis longus through the brachioradialis in a Pulvertaft fashion. Sharp tendon passers facilitate this technique (TECH FIG 3).
Weave the distal flexor pollicis longus through the brachioradialis in a Pulvertaft fashion. Sharp tendon passers facilitate this technique (TECH FIG 3).
![]() Adjust tension such that with wrist flexion, the MCP and interphalangeal joints of the thumb extend fully, and with wrist extension, they flex 30 to 40 degrees.
Adjust tension such that with wrist flexion, the MCP and interphalangeal joints of the thumb extend fully, and with wrist extension, they flex 30 to 40 degrees.
![]() Secure the weaves with 3-0 or 4-0 braided nonabsorbable sutures.
Secure the weaves with 3-0 or 4-0 braided nonabsorbable sutures.
![]() If the index or long FDP tendons also are ruptured, isolate the distal tendon stumps and repair them end to side.
If the index or long FDP tendons also are ruptured, isolate the distal tendon stumps and repair them end to side.
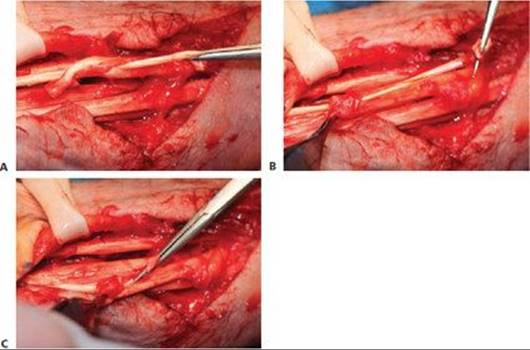
TECH FIG 3 • A, B. Pulvertaft weave shown sequentially as a sharp tendon passer is used to puncture the tendon through and through and then grasp the tendon being transferred and weave it through the recipient tendon. C.The transfer is secured at each weave with one or two nonabsorbable braided nylon sutures. (From Lubahn JD, Wolfe TL. Surgical treatment and rehabilitation and tendon ruptures in the rheumatoid hand. In: Mackin EJ, Callahan AD, Skirven TM, et al, eds. Rehabilitation of the Hand and Upper Extremity, ed 5. St. Louis: Mosby, 2002:1598–1607.)
EXTENSOR POLLICIS LONGUS TENDON TRANSFER (RECONSTRUCTION OF THUMB BOUTONNIÈRE DEFORMITY)
![]() Make a longitudinal incision to expose and identify the EPL tendon at its insertion onto the base of the distal phalanx.
Make a longitudinal incision to expose and identify the EPL tendon at its insertion onto the base of the distal phalanx.
![]() Incise the tendon at that level and mobilize it proximally (TECH FIG 4A).
Incise the tendon at that level and mobilize it proximally (TECH FIG 4A).
![]() Carefully protect the intrinsic tendon, which will now be the sole extensor for the thumb interphalangeal joint.
Carefully protect the intrinsic tendon, which will now be the sole extensor for the thumb interphalangeal joint.
![]() Expose the dorsal base of the proximal phalanx and weave the EPL tendon through the dorsal capsule, securing it using a 3-0 or 4-0 nonabsorbable braided suture (TECH FIG 4B).
Expose the dorsal base of the proximal phalanx and weave the EPL tendon through the dorsal capsule, securing it using a 3-0 or 4-0 nonabsorbable braided suture (TECH FIG 4B).
![]() Alternatively, secure the EPL tendon in place using drill holes or a suture anchor in the proximal phalanx (TECH FIG 4C,D).
Alternatively, secure the EPL tendon in place using drill holes or a suture anchor in the proximal phalanx (TECH FIG 4C,D).
![]() The thumb is splinted or casted for 4 weeks and a protective splint is worn for strenuous activities for 6 to 8 weeks.
The thumb is splinted or casted for 4 weeks and a protective splint is worn for strenuous activities for 6 to 8 weeks.
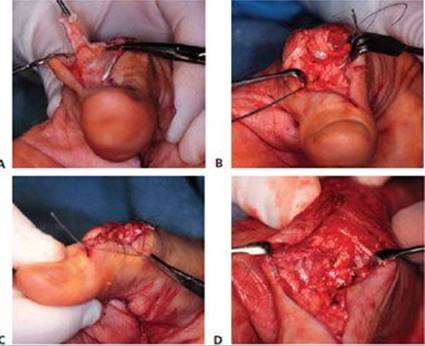
TECH FIG 4 • Extensor pollicis brevis rupture. A,B. Tendon transfer of the extensor pollicis longus proximally to the site of insertion of the extensor pollicis brevis, allowing the hyperextended interphalangeal joint to drop into a more flexed position and allowing active extension at the level of the metacarpophalangeal joint. C,D. Extensor pollicis longus is anchored through drill holes to the base of the proximal phalanx. (From Lubahn JD, Wolfe TL. Surgical treatment and rehabilitation and tendon ruptures in the rheumatoid hand. In: Mackin EJ, Callahan AD, Skirven TM, et al, eds. Rehabilitation of the Hand and Upper Extremity, ed 5. St. Louis: Mosby, 2002:1598–1607.)
POSTOPERATIVE CARE
![]() Postoperative care for each of these tendon transfers is similar.
Postoperative care for each of these tendon transfers is similar.
![]() In the case of tendon transfer to restore loss of finger extensors, the hand and wrist are immobilized with the wrist extended about 40 degrees. More may be desirable in certain instances, but too much extension could damage already fragile joints.
In the case of tendon transfer to restore loss of finger extensors, the hand and wrist are immobilized with the wrist extended about 40 degrees. More may be desirable in certain instances, but too much extension could damage already fragile joints.
![]() The MCP joints are brought into flexion until tension is noted at the suture line. Forty degrees or more is ideal to maintain the desired length of the collateral ligaments and prevent MCP joint extension contractures.
The MCP joints are brought into flexion until tension is noted at the suture line. Forty degrees or more is ideal to maintain the desired length of the collateral ligaments and prevent MCP joint extension contractures.
![]() Immobilization is continued for 3.5 to 4 weeks, and gentle active motion is begun, maintaining the hand in a splint for protection.
Immobilization is continued for 3.5 to 4 weeks, and gentle active motion is begun, maintaining the hand in a splint for protection.
![]() At 6 weeks, some resistive exercises may be added to the program. By 12 weeks, the patient should be able to resume normal activities.
At 6 weeks, some resistive exercises may be added to the program. By 12 weeks, the patient should be able to resume normal activities.
![]() In the case of flexor tendon rupture, the hand and wrist are immobilized with the wrist in 60 degrees of flexion, the MCP joints in 40 degrees of flexion, and the interphalangeal joints allowed to extend until tension is noted at the suture line. Immobilization is continued for 6 weeks, at which time a gentle active range-of-motion program is begun without resistance.
In the case of flexor tendon rupture, the hand and wrist are immobilized with the wrist in 60 degrees of flexion, the MCP joints in 40 degrees of flexion, and the interphalangeal joints allowed to extend until tension is noted at the suture line. Immobilization is continued for 6 weeks, at which time a gentle active range-of-motion program is begun without resistance.
![]() At 12 weeks resistive exercises are added and the patient is permitted to gradually resume normal activity.
At 12 weeks resistive exercises are added and the patient is permitted to gradually resume normal activity.
OUTCOMES
![]() Outcomes in tendon transfer surgery in rheumatoid arthritis are highly dependent on the patient's medical condition and ability to cooperate with the postoperative splinting and rehabilitation program. Most patients who are supervised by a therapist achieve a better result than those who try to make it on their own.
Outcomes in tendon transfer surgery in rheumatoid arthritis are highly dependent on the patient's medical condition and ability to cooperate with the postoperative splinting and rehabilitation program. Most patients who are supervised by a therapist achieve a better result than those who try to make it on their own.
![]() With good medical management of rheumatoid arthritis, when the disease is well controlled, and in cooperative patients who are motivated to improve, good results should be expected.
With good medical management of rheumatoid arthritis, when the disease is well controlled, and in cooperative patients who are motivated to improve, good results should be expected.
![]() Tendon transfer should always be delayed in patients with active disease as results will be poor.
Tendon transfer should always be delayed in patients with active disease as results will be poor.
![]() The only surgical procedure to be performed in poorly controlled patients is synovectomy, and with the caveat that success hinges on eventual good medical control of the disease.
The only surgical procedure to be performed in poorly controlled patients is synovectomy, and with the caveat that success hinges on eventual good medical control of the disease.
COMPLICATIONS
![]() Infection
Infection
![]() Skin or surgical wound breakdown
Skin or surgical wound breakdown
![]() Attenuation of the transferred tendon
Attenuation of the transferred tendon
![]() Rerupture of the tendons
Rerupture of the tendons
![]() Loss of motion due to improper tensioning of the transferred tendon
Loss of motion due to improper tensioning of the transferred tendon
![]() Joint stiffness
Joint stiffness
REFERENCES
1. Boyes JH, ed. In: Bunnell's Surgery of the Hand, 5th ed. Philadelphia: JB Lippincott, 1970.
2. Hamlin C, Littler JW. Restoration of the extensor pollicis longus tendon by an intercalated graft. J Bone Joint Surg Am 1977;59A: 412–414.
3. Mannerfelt L, Norman O. Attrition ruptures of flexor tendons in rheumatoid arthritis caused by bony spurs in the carpal tunnel: a clinical and radiological study. J Bone Joint Surg Br 1969;51B: 270–277.
4. Nalebuff EA. Diagnosis, classification and management of rheumatoid thumb deformities. Bull Hosp Joint Dis 1968;29:119–137.
5. Nalebuff EA, Millender LH. Surgical treatment of the boutonniere deformity in rheumatoid arthritis. Orthop Clin North Am 1975; 6:753–763.
6. Vaughan-Jackson OJ. Rupture of extensor tendons by attrition at the inferior radio-ulnar joint: report of two cases. J Bone Joint Surg Br 1948;30B:528–530.
7. Williamson SC, Feldon P. Extensor tendon ruptures in rheumatoid arthritis. Hand Clin 1995;11:449–459.