Harris Gellman and Patrick Owens
DEFINITION
![]() The site of compression must be identified to determine the appropriate treatment for symptoms of ulnar nerve dysfunction. Guyon's canal at the wrist is the second most common site of ulnar nerve entrapment.
The site of compression must be identified to determine the appropriate treatment for symptoms of ulnar nerve dysfunction. Guyon's canal at the wrist is the second most common site of ulnar nerve entrapment.
![]() Symptoms may be purely motor, purely sensory, or mixed, depending on the site and cause of compression.
Symptoms may be purely motor, purely sensory, or mixed, depending on the site and cause of compression.
ANATOMY
![]() In the distal half of the forearm, the ulnar nerve is joined on its lateral side by the ulnar artery. Proximal to the wrist, the nerve gives off a large dorsal sensory branch, which supplies sensation to the dorsum of the wrist and the ulnar side of the hand. The ulnar nerve continues into the hand through Guyon's canal.
In the distal half of the forearm, the ulnar nerve is joined on its lateral side by the ulnar artery. Proximal to the wrist, the nerve gives off a large dorsal sensory branch, which supplies sensation to the dorsum of the wrist and the ulnar side of the hand. The ulnar nerve continues into the hand through Guyon's canal.
![]() Guyon's canal is a triangular canal at the base of the ulnar side of the palm. It is 4 cm in length, extending from the proximal edge of the palmar carpal ligament to the fibrous edge of the hypothenar muscles.4 The space functions as a physiologic tunnel with discrete anatomic landmarks (FIG 1A).
Guyon's canal is a triangular canal at the base of the ulnar side of the palm. It is 4 cm in length, extending from the proximal edge of the palmar carpal ligament to the fibrous edge of the hypothenar muscles.4 The space functions as a physiologic tunnel with discrete anatomic landmarks (FIG 1A).
![]() Both the ulnar nerve and artery pass through the canal to enter the hand.
Both the ulnar nerve and artery pass through the canal to enter the hand.
![]() The dorsal cutaneous branch of the ulnar nerve usually branches before the nerve enters Guyon's canal.
The dorsal cutaneous branch of the ulnar nerve usually branches before the nerve enters Guyon's canal.
![]() It is bordered laterally by the hook of the hamate and the transverse carpal ligament. The medial wall is formed by the pisiform and the attachments of the pisohamate ligament.
It is bordered laterally by the hook of the hamate and the transverse carpal ligament. The medial wall is formed by the pisiform and the attachments of the pisohamate ligament.
![]() Dividing the tunnel into three zones helps in correlating the clinical symptoms with the specific pathologic cause4,13(FIG 1B).
Dividing the tunnel into three zones helps in correlating the clinical symptoms with the specific pathologic cause4,13(FIG 1B).
![]() Zone 1, about 3 cm in length, is the area proximal to the bifurcation of the ulnar nerve into motor and sensory branches. Compression in zone 1 results in combined motor and sensory loss. It is most commonly caused by a fracture of the hook of the hamate or a ganglion cyst.
Zone 1, about 3 cm in length, is the area proximal to the bifurcation of the ulnar nerve into motor and sensory branches. Compression in zone 1 results in combined motor and sensory loss. It is most commonly caused by a fracture of the hook of the hamate or a ganglion cyst.
![]() Zones 2 and 3 are located next to each other, from the point where the ulnar nerve divides into a superficial or sensory branch and a deep motor branch, to the region just beyond the fibrous arch of the hypothenar muscles.
Zones 2 and 3 are located next to each other, from the point where the ulnar nerve divides into a superficial or sensory branch and a deep motor branch, to the region just beyond the fibrous arch of the hypothenar muscles.
![]() Zone 2 encompasses the motor branch of the nerve, located in the dorsoradial portion of the tunnel. The deep motor branch, along with the deep branch of the ulnar artery, passes between the abductor digiti quinti and the flexor digiti quinti brevis, perforating the opponens digiti quinti. The motor branch then follows the deep volar arch across the palm to innervate the interossei.
Zone 2 encompasses the motor branch of the nerve, located in the dorsoradial portion of the tunnel. The deep motor branch, along with the deep branch of the ulnar artery, passes between the abductor digiti quinti and the flexor digiti quinti brevis, perforating the opponens digiti quinti. The motor branch then follows the deep volar arch across the palm to innervate the interossei.
![]() The nerve supplies the three intrinsic muscles of the small finger, the third and fourth lumbricales, the volar and dorsal interossei, the adductor pollicis, and the deep head of the flexor pollicis brevis.
The nerve supplies the three intrinsic muscles of the small finger, the third and fourth lumbricales, the volar and dorsal interossei, the adductor pollicis, and the deep head of the flexor pollicis brevis.
![]() Compression in this area causes pure motor loss to all of the ulnar-innervated muscles in the hand. Ganglions from the pisotriquetral joint and fractures of the hook of the hamate are the most common etiologic factors (FIG 1C). Due to the nerve's proximity to the hamate, it is unfortunately easy to damage the nerve while excising the hook of the hamate.
Compression in this area causes pure motor loss to all of the ulnar-innervated muscles in the hand. Ganglions from the pisotriquetral joint and fractures of the hook of the hamate are the most common etiologic factors (FIG 1C). Due to the nerve's proximity to the hamate, it is unfortunately easy to damage the nerve while excising the hook of the hamate.
![]() Zone 3, located ulnar to zone 2, encompasses the superficial or sensory branch of the bifurcated ulnar nerve. Compression here causes sensory loss to the hypothenar eminence, the small finger, and part of the ring finger, but does not usually cause motor deficits. Common causes are aneurysm of the ulnar artery, thrombosis, and synovial inflammation.
Zone 3, located ulnar to zone 2, encompasses the superficial or sensory branch of the bifurcated ulnar nerve. Compression here causes sensory loss to the hypothenar eminence, the small finger, and part of the ring finger, but does not usually cause motor deficits. Common causes are aneurysm of the ulnar artery, thrombosis, and synovial inflammation.
![]() The superficial branch of the ulnar nerve in Guyon's canal supplies the palmaris brevis and the skin of the hypothenar eminence and forms the digital nerves to the small and ulnar side of the ring finger.
The superficial branch of the ulnar nerve in Guyon's canal supplies the palmaris brevis and the skin of the hypothenar eminence and forms the digital nerves to the small and ulnar side of the ring finger.
![]() Two specific nerve anomalies can confuse the diagnosis.
Two specific nerve anomalies can confuse the diagnosis.
![]() Martin-Gruber anastomosis in the forearm: fibers that supply the intrinsic muscles are carried in the median nerve to the middle of the forearm, where they leave the median nerve to join the ulnar nerve. Functioning intrinsic muscles can be observed when the ulnar nerve is injured proximal to this anastomosis.
Martin-Gruber anastomosis in the forearm: fibers that supply the intrinsic muscles are carried in the median nerve to the middle of the forearm, where they leave the median nerve to join the ulnar nerve. Functioning intrinsic muscles can be observed when the ulnar nerve is injured proximal to this anastomosis.
![]() Riche-Cannieu anastomosis: the median and ulnar nerves are connected in the palm. Even with an injury at the wrist, some intrinsic function remains.
Riche-Cannieu anastomosis: the median and ulnar nerves are connected in the palm. Even with an injury at the wrist, some intrinsic function remains.
PATHOGENESIS
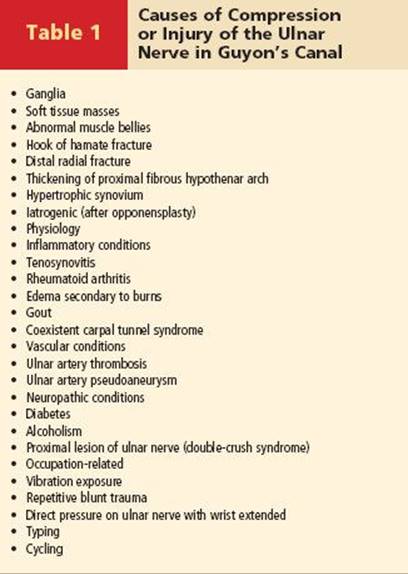
![]() Causative factors of compression or injury of the ulnar nerve in Guyon's canal include repeated blunt trauma from power tools and gripping or hammering with the palm of the hand, which may result in thrombosis or aneurysm of the ulnar artery compressing the nerve (hypothenar hammer syndrome)2,6,10 (FIG 2A,B, Table 1). Direct pressure on the ulnar nerve may occur during activities such as cycling.
Causative factors of compression or injury of the ulnar nerve in Guyon's canal include repeated blunt trauma from power tools and gripping or hammering with the palm of the hand, which may result in thrombosis or aneurysm of the ulnar artery compressing the nerve (hypothenar hammer syndrome)2,6,10 (FIG 2A,B, Table 1). Direct pressure on the ulnar nerve may occur during activities such as cycling.
![]() Fractures of the hook of the hamate can impinge on the nerve.
Fractures of the hook of the hamate can impinge on the nerve.
![]() Idiopathic compression may occur secondary to thickening of the proximal fibrous ligament at the entrance to the canal.
Idiopathic compression may occur secondary to thickening of the proximal fibrous ligament at the entrance to the canal.
![]() Compression also may occur as a result of swelling after distal radius fracture.
Compression also may occur as a result of swelling after distal radius fracture.
![]() Compression of the ulnar nerve at Guyon's canal also has been shown to occur in conjunction with carpal tunnel syndrome. It typically resolves after surgical decompression of the carpal canal.9,16
Compression of the ulnar nerve at Guyon's canal also has been shown to occur in conjunction with carpal tunnel syndrome. It typically resolves after surgical decompression of the carpal canal.9,16
![]() Other etiologies include tumors, such as ganglia or lipomas (FIG 2C,D), anomalous muscle bellies,8,15 or hypertrophy of the palmaris brevis.
Other etiologies include tumors, such as ganglia or lipomas (FIG 2C,D), anomalous muscle bellies,8,15 or hypertrophy of the palmaris brevis.
![]() Ganglia and other soft-tissue masses are responsible for 32% to 48% of cases of ulnar tunnel syndrome. Another 16% of cases are due to muscle anomalies.12
Ganglia and other soft-tissue masses are responsible for 32% to 48% of cases of ulnar tunnel syndrome. Another 16% of cases are due to muscle anomalies.12
![]() Synovitis secondary to rheumatoid arthritis may encroach upon the canal and the nerve.
Synovitis secondary to rheumatoid arthritis may encroach upon the canal and the nerve.
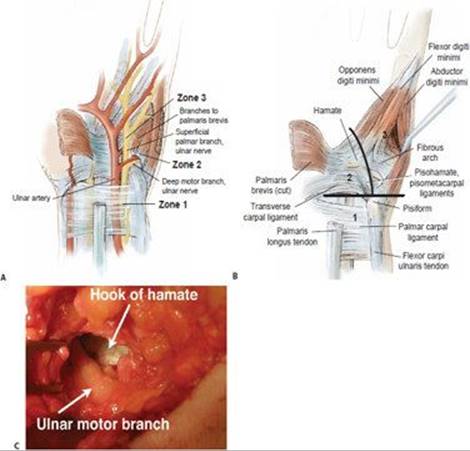
FIG 1 • A. Anatomic landmarks of the distal ulnar tunnel (Guyon's canal). Zone 1: Ulnar nerve in the region proximal to the bifurcation. Zone 2: Ulnar nerve motor segment, following bifurcation. Zone 3:Ulnar nerve sensory segment, distal to the bifurcation. B. Location of the three zones. Zone 1 is proximal to the bifurcation; zone 2 encompasses the motor branch; zone 3 is the region surrounding the sensory branch. C. The proximity of the motor branch of the ulnar nerve to the hook of the hamate as seen during excision of the hook.
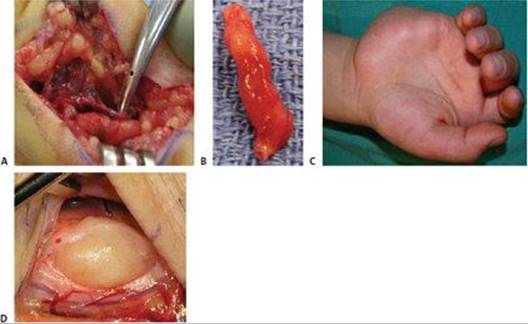
FIG 2 • A. Ulnar artery thrombosis. B. Resected thrombosed segment. C. Hypothenar mass as a cause of compression of the ulnar nerve at the wrist. D. Lipoma causing compression of the nerve.
![]() Metabolic or infectious diseases such as diabetes, thyroid disease, or leprosy may also mimic the symptoms of nerve compression.
Metabolic or infectious diseases such as diabetes, thyroid disease, or leprosy may also mimic the symptoms of nerve compression.
![]() Iatrogenic causes must also be recognized, such as compression by tendon or muscle transfer (Huber opponensplasty).11
Iatrogenic causes must also be recognized, such as compression by tendon or muscle transfer (Huber opponensplasty).11
NATURAL HISTORY
![]() Untreated compression may result in permanent dysfunction, weakness, and numbness.
Untreated compression may result in permanent dysfunction, weakness, and numbness.
PATIENT HISTORY AND PHYSICAL FINDINGS
Clinical History
![]() Presenting symptoms can vary from mild, transient paresthesias in the ring and small fingers to clawing of these digits and severe intrinsic muscle atrophy.
Presenting symptoms can vary from mild, transient paresthesias in the ring and small fingers to clawing of these digits and severe intrinsic muscle atrophy.
![]() The patient may report severe pain at the elbow or wrist with radiation into the hand or up into the shoulder and neck.
The patient may report severe pain at the elbow or wrist with radiation into the hand or up into the shoulder and neck.
![]() Patients may report difficulty or clumsiness when opening jars or turning doorknobs.
Patients may report difficulty or clumsiness when opening jars or turning doorknobs.
![]() Early fatigue or weakness may be noticed if work requires repetitive hand motions.
Early fatigue or weakness may be noticed if work requires repetitive hand motions.
![]() Depending on the climate and work conditions, cold intolerance in the ring and small fingers may be present.5
Depending on the climate and work conditions, cold intolerance in the ring and small fingers may be present.5
![]() A careful clinical history is imperative, noting the time of occurrence of symptoms. Determine whether symptoms are transient or continuous. Determine whether symptoms are related to work, sleep, or recreation. Elicit duration of symptoms and possible relation to trauma.
A careful clinical history is imperative, noting the time of occurrence of symptoms. Determine whether symptoms are transient or continuous. Determine whether symptoms are related to work, sleep, or recreation. Elicit duration of symptoms and possible relation to trauma.
Physical Examination7,17
![]() It is important to determine the level of pathology of the ulnar nerve, because compression commonly occurs at four points: the cervical spine, the thoracic outlet, the elbow (cubital tunnel syndrome), or the wrist (Guyon's canal).
It is important to determine the level of pathology of the ulnar nerve, because compression commonly occurs at four points: the cervical spine, the thoracic outlet, the elbow (cubital tunnel syndrome), or the wrist (Guyon's canal).
![]() Begin the clinical examination at the neck and shoulder and move down the affected extremity to the elbow.
Begin the clinical examination at the neck and shoulder and move down the affected extremity to the elbow.
![]() Pain on neck movement mimicking the patient's symptoms could indicate cervical disc disease.
Pain on neck movement mimicking the patient's symptoms could indicate cervical disc disease.
![]() Pain on palpation of the plexus or with shoulder motion could indicate a pathologic condition in the brachial plexus or lung. Results of provocative maneuvers for thoracic outlet syndrome should be assessed.
Pain on palpation of the plexus or with shoulder motion could indicate a pathologic condition in the brachial plexus or lung. Results of provocative maneuvers for thoracic outlet syndrome should be assessed.
![]() Masses on the medial side of the arm could indicate a soft tissue tumor or hemorrhage compressing the nerve.
Masses on the medial side of the arm could indicate a soft tissue tumor or hemorrhage compressing the nerve.
![]() At the elbow, note any deformity, palpate the nerve, and determine whether abnormal mobility is present.
At the elbow, note any deformity, palpate the nerve, and determine whether abnormal mobility is present.
![]() The course of the nerve is palpated in the forearm all the way to the wrist.
The course of the nerve is palpated in the forearm all the way to the wrist.
![]() A positive Tinel or Phalen's sign often is found at the wrist over the ulnar nerve.
A positive Tinel or Phalen's sign often is found at the wrist over the ulnar nerve.
![]() Tenderness over the hook of the hamate is particularly important.
Tenderness over the hook of the hamate is particularly important.
![]() Sensory function is assessed.
Sensory function is assessed.
![]() Semmes-Weinstein monofilament testing may be abnormal, but often is normal early in the course of the compression.
Semmes-Weinstein monofilament testing may be abnormal, but often is normal early in the course of the compression.
![]() Two-point discrimination of the ring and small fingers usually becomes abnormal only late in the course of the disease.
Two-point discrimination of the ring and small fingers usually becomes abnormal only late in the course of the disease.
![]() To help differentiate cubital tunnel syndrome from compression of the ulnar nerve at the wrist, assess flexor carpi ulnaris and flexor digitorum profundus strength.
To help differentiate cubital tunnel syndrome from compression of the ulnar nerve at the wrist, assess flexor carpi ulnaris and flexor digitorum profundus strength.
![]() Intrinsic muscle function is tested by asking the patient to cross the long finger over the index finger (ie, crossed finger test).
Intrinsic muscle function is tested by asking the patient to cross the long finger over the index finger (ie, crossed finger test).
![]() Only two muscles can be tested accurately in the hand—the abductor digiti quinti and the first dorsal interosseous. The tendons or bellies of these muscles can be palpated or visualized.
Only two muscles can be tested accurately in the hand—the abductor digiti quinti and the first dorsal interosseous. The tendons or bellies of these muscles can be palpated or visualized.
![]() Weakness of thumb pinch may be elicited by the Froment sign. Froment's sign is ruled positive if the person must flex the thumb interphalangeal joint to maintain grasp.
Weakness of thumb pinch may be elicited by the Froment sign. Froment's sign is ruled positive if the person must flex the thumb interphalangeal joint to maintain grasp.
IMAGING AND OTHER DIAGNOSTIC STUDIES
![]() Radiographs of the elbow and wrist are mandatory in ulnar nerve compression, because entrapment of the ulnar nerve may occur at more than one level.
Radiographs of the elbow and wrist are mandatory in ulnar nerve compression, because entrapment of the ulnar nerve may occur at more than one level.
![]() Radiographs of the hand and wrist should include carpal tunnel views as well as standard anteroposterior (AP), lateral, and oblique views. Radiographs of the wrist may reveal fractures of the hook of the hamate, dislocations of the carpal bones, or, less commonly, soft tissue masses and calcifications.
Radiographs of the hand and wrist should include carpal tunnel views as well as standard anteroposterior (AP), lateral, and oblique views. Radiographs of the wrist may reveal fractures of the hook of the hamate, dislocations of the carpal bones, or, less commonly, soft tissue masses and calcifications.
![]() Radiographs of the elbow may reveal abnormal anatomy, such as a valgus deformity, bone spurs or bone fragments, a shallow olecranon groove, osteochondromas, or destructive lesions (eg, tumors, infections, abnormal calcifications).
Radiographs of the elbow may reveal abnormal anatomy, such as a valgus deformity, bone spurs or bone fragments, a shallow olecranon groove, osteochondromas, or destructive lesions (eg, tumors, infections, abnormal calcifications).
![]() Radiographs of the neck should be obtained if cervical disc disease is suspected and to rule out cervical ribs.
Radiographs of the neck should be obtained if cervical disc disease is suspected and to rule out cervical ribs.
![]() Obtain radiographs of the chest if a Pancoast tumor or tuberculosis is suspected.
Obtain radiographs of the chest if a Pancoast tumor or tuberculosis is suspected.
![]() MRI is not usually necessary unless further delineation of soft tissue masses such as lipomas or ganglions11 or visualization of fractures, aneurysms, congenital abnormality, or other abnormalities in the nerve is required. MRI also may detect structural abnormalities along the course of the ulnar nerve accounting for compression (eg, fibrous bands).
MRI is not usually necessary unless further delineation of soft tissue masses such as lipomas or ganglions11 or visualization of fractures, aneurysms, congenital abnormality, or other abnormalities in the nerve is required. MRI also may detect structural abnormalities along the course of the ulnar nerve accounting for compression (eg, fibrous bands).
![]() Ultrasonography may be used to detect cysts or masses in Guyon's canal and to assess ulnar nerve diameter at the elbow.
Ultrasonography may be used to detect cysts or masses in Guyon's canal and to assess ulnar nerve diameter at the elbow.
![]() Electromyography (EMG) and nerve conduction studies are helpful to confirm the specific area(s) of entrapment as well as document the extent of the pathology.
Electromyography (EMG) and nerve conduction studies are helpful to confirm the specific area(s) of entrapment as well as document the extent of the pathology.
![]() Motor and sensory conduction velocities are more useful in a recent entrapment, whereas conduction velocities and EMG are useful in chronic neuropathies (EMG shows axonal degeneration).
Motor and sensory conduction velocities are more useful in a recent entrapment, whereas conduction velocities and EMG are useful in chronic neuropathies (EMG shows axonal degeneration).
![]() Conduction velocity short-segment stimulation (also known as the inching technique) can increase the sensitivity of this method and can improve localization by helping the examiner determine exactly where a blockage is occurring.
Conduction velocity short-segment stimulation (also known as the inching technique) can increase the sensitivity of this method and can improve localization by helping the examiner determine exactly where a blockage is occurring.
![]() EMG evaluation of motor unit morphology and recruitment patterns ascertains ongoing loss of muscle fibers via detection of abnormal spontaneous activity (eg, fibrillation potentials and fasciculations). It also checks the integrity of the muscle membrane to expand differential diagnosis (eg, myotonia, paramyotonia, periodic paralysis) as manifested by increased insertional activity such as complex repetitive discharges, myokymia, and (para)myotonic discharges.1
EMG evaluation of motor unit morphology and recruitment patterns ascertains ongoing loss of muscle fibers via detection of abnormal spontaneous activity (eg, fibrillation potentials and fasciculations). It also checks the integrity of the muscle membrane to expand differential diagnosis (eg, myotonia, paramyotonia, periodic paralysis) as manifested by increased insertional activity such as complex repetitive discharges, myokymia, and (para)myotonic discharges.1
DIFFERENTIAL DIAGNOSIS 17
![]() Cervical disc disease
Cervical disc disease
![]() Brachial plexus abnormalities, thoracic outlet syndrome, Pancoast tumor
Brachial plexus abnormalities, thoracic outlet syndrome, Pancoast tumor
![]() Elbow abnormalities, epicondylitis
Elbow abnormalities, epicondylitis
![]() Infections, tumors, diabetes mellitus, hypothyroidism, rheumatoid diseases, alcoholism
Infections, tumors, diabetes mellitus, hypothyroidism, rheumatoid diseases, alcoholism
![]() Wrist fractures
Wrist fractures
![]() Ulnar artery aneurysms or thrombosis at the wrist
Ulnar artery aneurysms or thrombosis at the wrist
NONOPERATIVE MANAGEMENT
![]() Conservative treatment of ulnar nerve compression is most successful when paresthesias are transient. Patient education and insight are important.
Conservative treatment of ulnar nerve compression is most successful when paresthesias are transient. Patient education and insight are important.
![]() Flexing the wrist at work while typing for long periods, or resting the wrist on the handlebars of a bicycle or motorcycle while driving, are causes of paresthesia that can be corrected without surgical treatment.
Flexing the wrist at work while typing for long periods, or resting the wrist on the handlebars of a bicycle or motorcycle while driving, are causes of paresthesia that can be corrected without surgical treatment.
![]() Avoiding the use of vibrating or power tools, wrist splinting in a neutral position, and correction of ergonomics at work should help alleviate transient palsies.
Avoiding the use of vibrating or power tools, wrist splinting in a neutral position, and correction of ergonomics at work should help alleviate transient palsies.
![]() Nonsteroidal anti-inflammatory medications also are useful adjuncts to relieve nerve irritation.
Nonsteroidal anti-inflammatory medications also are useful adjuncts to relieve nerve irritation.
![]() Oral vitamin B 6 supplements may be helpful for mild symptoms. This treatment should be carried out for 6 to 12 weeks, depending on patient response.
Oral vitamin B 6 supplements may be helpful for mild symptoms. This treatment should be carried out for 6 to 12 weeks, depending on patient response.
SURGICAL MANAGEMENT
![]() Surgical intervention is indicated if paresthesia increases despite adequate conservative treatment combined with abnormal nerve conduction studies or EMGs, and at the first sign of motor changes.
Surgical intervention is indicated if paresthesia increases despite adequate conservative treatment combined with abnormal nerve conduction studies or EMGs, and at the first sign of motor changes.
![]() In a patient who sustains an immediate complete ulnar nerve injury as a result of a fracture of the wrist, the fracture should be reduced as soon as possible.
In a patient who sustains an immediate complete ulnar nerve injury as a result of a fracture of the wrist, the fracture should be reduced as soon as possible.
![]() Elimination of any dorsal displacement of the distal radius or ulna should be achieved.
Elimination of any dorsal displacement of the distal radius or ulna should be achieved.
![]() If ulnar nerve function does not improve within 24 to 36 hours following satisfactory reduction, the nerve should be explored and decompression carried out.3,12
If ulnar nerve function does not improve within 24 to 36 hours following satisfactory reduction, the nerve should be explored and decompression carried out.3,12
Preoperative Planning
![]() The diagnosis should be confirmed with EMG and nerve conduction velocity or imaging studies (eg, MRI) before planning surgery.
The diagnosis should be confirmed with EMG and nerve conduction velocity or imaging studies (eg, MRI) before planning surgery.
Positioning
![]() Patients are operated on in the supine position with the arm extended on an armboard.
Patients are operated on in the supine position with the arm extended on an armboard.
![]() A tourniquet is placed above the elbow and inflated to 250 to 265 mm Hg before the incision is made.
A tourniquet is placed above the elbow and inflated to 250 to 265 mm Hg before the incision is made.
Approach
![]() Operative treatment is aimed at exploring and decompressing the nerve from the distal forearm into the hand throughout all three zones.
Operative treatment is aimed at exploring and decompressing the nerve from the distal forearm into the hand throughout all three zones.
TECHNIQUES
ULNAR NERVE EXPLORATION AND DECOMPRESSION OF GUYON'S CANAL
![]() Palpate and mark the pisiform.
Palpate and mark the pisiform.
![]() The hook of the hamate can be found 1 cm distal and lateral to the pisiform.
The hook of the hamate can be found 1 cm distal and lateral to the pisiform.
![]() Make a curvilinear incision beginning distally in the interval between the pisiform and the hook of the hamate. Cross the wrist, extending proximal to the distal wrist flexion crease, along the radial border of the flexor carpi ulnaris (TECH FIG 1A).
Make a curvilinear incision beginning distally in the interval between the pisiform and the hook of the hamate. Cross the wrist, extending proximal to the distal wrist flexion crease, along the radial border of the flexor carpi ulnaris (TECH FIG 1A).
![]() The wrist should be crossed in a zigzag fashion to prevent longitudinal contracture of the scar.
The wrist should be crossed in a zigzag fashion to prevent longitudinal contracture of the scar.
![]() Perform the dissection proximal to distal. Identify the ulnar nerve proximal to the distal wrist flexor retinaculum and follow it distally through Guyon's canal by reflecting the flexor carpi ulnaris and the pisohamate ligament.
Perform the dissection proximal to distal. Identify the ulnar nerve proximal to the distal wrist flexor retinaculum and follow it distally through Guyon's canal by reflecting the flexor carpi ulnaris and the pisohamate ligament.
![]() The neurovascular bundle is traced distally to the point at which it enters Guyon's canal beneath the palmar carpal ligament.
The neurovascular bundle is traced distally to the point at which it enters Guyon's canal beneath the palmar carpal ligament.
![]() Incise the ligament, palmaris brevis muscle, and fibrous tissue, decompressing the nerve along its entire course through the canal.
Incise the ligament, palmaris brevis muscle, and fibrous tissue, decompressing the nerve along its entire course through the canal.
![]() The branches of the ulnar nerve to the hypothenar muscles and palmaris brevis, as well as the deep branch of the nerve, can be identified and protected with this approach.
The branches of the ulnar nerve to the hypothenar muscles and palmaris brevis, as well as the deep branch of the nerve, can be identified and protected with this approach.
![]() The incision should not be carried ulnarly over the hypothenar eminence, to avoid injury to the palmar cutaneous branch of the ulnar nerve.
The incision should not be carried ulnarly over the hypothenar eminence, to avoid injury to the palmar cutaneous branch of the ulnar nerve.
![]() The ulnar artery should be examined for areas of thickening or thrombosis, and the ulnar nerve should be examined along its course for intra- or extraneural tumors (eg, schwannoma, neurolemmoma).
The ulnar artery should be examined for areas of thickening or thrombosis, and the ulnar nerve should be examined along its course for intra- or extraneural tumors (eg, schwannoma, neurolemmoma).
![]() Further exploration of the floor of the canal should be done to identify masses, ganglions, anomalous muscles, fibrous bands, osteophytes, or fracture fragments.
Further exploration of the floor of the canal should be done to identify masses, ganglions, anomalous muscles, fibrous bands, osteophytes, or fracture fragments.
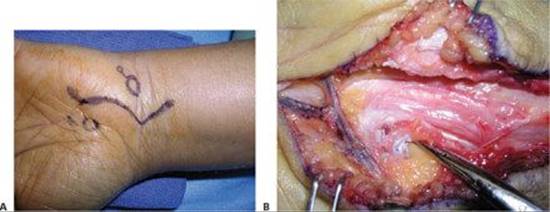
TECH FIG 1 • A. The skin incision is marked crossing the wrist at an angle to prevent scar contracture. B. The motor branch is followed into the interval between the flexor digiti minimi and abductor digiti minimi muscles.
![]() The motor branch is followed into the interval between the flexor digiti minimi and abductor digiti minimi muscles and through the origin of the opponens digiti minimi (TECH FIG 1B).
The motor branch is followed into the interval between the flexor digiti minimi and abductor digiti minimi muscles and through the origin of the opponens digiti minimi (TECH FIG 1B).
![]() After exploration and decompression, release the tourniquet and coagulate all bleeders with a bipolar cautery before the wound is closed.
After exploration and decompression, release the tourniquet and coagulate all bleeders with a bipolar cautery before the wound is closed.
![]() Hematoma in this area could potentially compress the nerve and artery.
Hematoma in this area could potentially compress the nerve and artery.

POSTOPERATIVE CARE
![]() Postoperatively, patients are placed into a protective splint for about 2 weeks to prevent excessive wrist flexion and extension.
Postoperatively, patients are placed into a protective splint for about 2 weeks to prevent excessive wrist flexion and extension.
![]() Sutures are removed at 10 to 14 days after surgery, at which time gentle active range of motion is started, as well as scar care.
Sutures are removed at 10 to 14 days after surgery, at which time gentle active range of motion is started, as well as scar care.
![]() The wrist splint should be continued for 2 to 3 more weeks to prevent scar thickening, which is common in this area.
The wrist splint should be continued for 2 to 3 more weeks to prevent scar thickening, which is common in this area.
![]() Silicone or otoform is helpful to prevent hard, firm scars.
Silicone or otoform is helpful to prevent hard, firm scars.
OUTCOMES
![]() Symptoms can be expected to improve in all cases, with fewer than 20% of patients complaining of slight persistent numbness after the surgery.14
Symptoms can be expected to improve in all cases, with fewer than 20% of patients complaining of slight persistent numbness after the surgery.14
![]() The most common cause of failure of surgery is failure in diagnosis, followed by inadequate decompression of all of the branches of the ulnar nerve.
The most common cause of failure of surgery is failure in diagnosis, followed by inadequate decompression of all of the branches of the ulnar nerve.
COMPLICATIONS
![]() Laceration of the ulnar nerve or artery (or both)
Laceration of the ulnar nerve or artery (or both)
![]() Inadequate decompression
Inadequate decompression
![]() Injury to the ulnar artery
Injury to the ulnar artery
REFERENCES
1. Agarwal SK, Schneider LB, Ahmad BK. Clinical usefulness of ulnar motor responses recording from first dorsal interosseous. Muscle Nerve 1995;18:1043.
2. Aguiar PH, Bor-Seng-Shu E, Gomes-Pinto F, et al. Surgical management of Guyon's canal syndrome, an ulnar nerve entrapment at the wrist: Report of two cases. Arq Neuropsiquiatr 2001;59:106–111.
3. Bartels RH, Grotenhuis JA, Kauer JM. The arcade of Struthers: An anatomical study. Acta Neurochir (Wien) 2003;145:295–300.
4. Beekman R, Wokke JH, Schoemaker MC, et al. Ulnar neuropathy at the elbow: Follow-up and prognostic factors determining outcome. Neurology 2004;63:1675–1680.
5. Beekman R, Schoemaker MC, Van Der Plas JP, et al. Diagnostic value of high-resolution sonography in ulnar neuropathy at the elbow. Neurology 2004;62:767–773.
6. Beekman R, Van Der Plas JP, Uitdehaag BM, et al. Clinical, electrodiagnostic, and sonographic studies in ulnar neuropathy at the elbow. Muscle Nerve 2004;30:202–208.
7. Bradshaw DY, Shefner JM. Ulnar neuropathy at the elbow. Neurol Clin 1999;17:447–461.
8. Buzzard EF. Some varieties of toxic and traumatic ulnar neuritis. Lancet 1922;1:317.
9. Campbell WW. Ulnar neuropathy at the elbow. Muscle Nerve 2000;23:450–452.
10. Cooke RA. Hypothenar hammer syndrome: A discrete syndrome to be distinguished from hand–arm vibration syndrome. Occup Med (Lond) 2003;53:320–324.
11. Feindel W, J Stratford J. Cubital tunnel compression in tardy ulnar palsy. Can Med Assoc J 1958;78:351–353.
12. Gelberman RH. Ulnar tunnel syndrome. In: Gelberman RH, ed. Operative Nerve Repair and Reconstruction. Philadelphia: JB Lippincott, 1991:1131–1143.
13. Gross MS, Gelberman RH. The anatomy of the distal ulnar tunnel. Clin Orthop Relat Res 1985;196:238–247.
14. Murata K, Shih JT, Tsai TM. Causes of ulnar tunnel syndrome: a retrospective study of 31 subjects. J Hand Surg Am 2003;28:647–651.
15. Pribyl CR, Moneim MS. Anomalous hand muscle found in Guyon's canal at exploration for ulnar artery thrombosis: a case report. Clin Orthop Relat Res 1994;306:120–123.
16. Silver MA, Gelberman RH, Gellman H, et al. Carpal tunnel syndrome: Associated abnormalities in ulnar nerve function and the effect of carpal tunnel release on these abnormalities. J Hand Surg Am 1985;10:710–713.
17. Szabo RM, Steinberg DR. Nerve entrapment syndromes in the wrist. J Am Acad Orthop Surg 1994;2:115–123.