Jason P. Glover, Christopher F. Hyer, and Gregory C. Berlet
DEFINITION
![]() Hallux valgus is a static subluxation of the first metatarsophalangeal (MTP) joint with medial deviation of the first metatarsal and lateral or valgus rotation of the hallux. A medial or dorsomedial prominence is present and usually called a bunion.
Hallux valgus is a static subluxation of the first metatarsophalangeal (MTP) joint with medial deviation of the first metatarsal and lateral or valgus rotation of the hallux. A medial or dorsomedial prominence is present and usually called a bunion.
![]() The development of hallux valgus is debated but occurs almost exclusively in shod populations.11,15,18 Other causes that may contribute to a hallux valgus deformity include heredity,4,6,14,25 pes planus,9,10,12,19,21metatarsus primus varus,10,23 systemic arthritis,16,20,24 neuromuscular disorders, excessive roundness of the metatarsal head,2 and abnormal obliquity of the first metacarpal joint.13 Hypermobility may also be another causative factor in the formation of a bunion, and a first metatarsal–cuneiform joint fusion may be an appropriate alternative procedure.
The development of hallux valgus is debated but occurs almost exclusively in shod populations.11,15,18 Other causes that may contribute to a hallux valgus deformity include heredity,4,6,14,25 pes planus,9,10,12,19,21metatarsus primus varus,10,23 systemic arthritis,16,20,24 neuromuscular disorders, excessive roundness of the metatarsal head,2 and abnormal obliquity of the first metacarpal joint.13 Hypermobility may also be another causative factor in the formation of a bunion, and a first metatarsal–cuneiform joint fusion may be an appropriate alternative procedure.
![]() Hallux valgus can lead to painful motion of the joint or difficulty with footwear.
Hallux valgus can lead to painful motion of the joint or difficulty with footwear.
![]() Surgical correction of bunion deformity is a common procedure. For larger deformities a proximal osteotomy of the first metatarsal is required. The Mau proximal osteotomy technique is an accepted and proven technique. This osteotomy has the advantage over other proximal osteotomies of being inherently stable, having a reproducible surgical technique, and minimizing the common complications of other proximal osteotomies.
Surgical correction of bunion deformity is a common procedure. For larger deformities a proximal osteotomy of the first metatarsal is required. The Mau proximal osteotomy technique is an accepted and proven technique. This osteotomy has the advantage over other proximal osteotomies of being inherently stable, having a reproducible surgical technique, and minimizing the common complications of other proximal osteotomies.
ANATOMY
![]() The first MTP joint is two joints with a ball-and-socket type of joint between the first metatarsal and proximal phalanx. The second portion is a groove on the plantar first metatarsal that articulates with the dorsal surface of two sesamoids. These joints share a common capsule and interrelated muscles.
The first MTP joint is two joints with a ball-and-socket type of joint between the first metatarsal and proximal phalanx. The second portion is a groove on the plantar first metatarsal that articulates with the dorsal surface of two sesamoids. These joints share a common capsule and interrelated muscles.
![]() Collateral ligaments are fan-shaped ligaments that originate from the medial and lateral epicondyles of the first metatarsal head. These ligaments run vertical, horizontal, and oblique from the first metatarsal head, proximal phalanx, and sesamoids.
Collateral ligaments are fan-shaped ligaments that originate from the medial and lateral epicondyles of the first metatarsal head. These ligaments run vertical, horizontal, and oblique from the first metatarsal head, proximal phalanx, and sesamoids.
![]() The sesamoids (medial and lateral) are separated by a rounded ridge (crista) and are connected by the intersesamoidal ligament. The lateral sesamoid is also connected to the plantar plate of the second metatarsal head by the transverse intermetatarsal ligament. In addition to collateral ligament attachments, each sesamoid is contained by a separated tendon of the flexor hallucis brevis muscle.
The sesamoids (medial and lateral) are separated by a rounded ridge (crista) and are connected by the intersesamoidal ligament. The lateral sesamoid is also connected to the plantar plate of the second metatarsal head by the transverse intermetatarsal ligament. In addition to collateral ligament attachments, each sesamoid is contained by a separated tendon of the flexor hallucis brevis muscle.
![]() Intrinsic muscles that insert on the proximal phalanx are the abductor hallucis (plantar medial) and the oblique–transverse head of the adductor hallucis (plantar lateral phalanx). Both of these tendons also blend in with the flexor hallucis brevis to invest each corresponding sesamoid. These intrinsic muscles act to maintain alignment of the hallux and balance the forces of each other.
Intrinsic muscles that insert on the proximal phalanx are the abductor hallucis (plantar medial) and the oblique–transverse head of the adductor hallucis (plantar lateral phalanx). Both of these tendons also blend in with the flexor hallucis brevis to invest each corresponding sesamoid. These intrinsic muscles act to maintain alignment of the hallux and balance the forces of each other.
![]() Extrinsic muscles include the flexor hallucis longus (FHL) and extensor hallucis longus (EHL). The FHL lies within a groove plantar to the intersesamoidal ligament. It proceeds distally to insert into the base of the distal phalanx. The EHL runs over the dorsal surface of the proximal phalanx and inserts into the base of the distal phalanx. Over the first MTP the EHL is anchored to the sesamoids by the extensor sling.
Extrinsic muscles include the flexor hallucis longus (FHL) and extensor hallucis longus (EHL). The FHL lies within a groove plantar to the intersesamoidal ligament. It proceeds distally to insert into the base of the distal phalanx. The EHL runs over the dorsal surface of the proximal phalanx and inserts into the base of the distal phalanx. Over the first MTP the EHL is anchored to the sesamoids by the extensor sling.
PATHOGENESIS
![]() The development of hallux valgus varies depending on the causative factor.
The development of hallux valgus varies depending on the causative factor.
![]() The function of the abductor hallucis muscle is to plantarflex, adduct, and invert the proximal phalanx. The reverse is true for the adductor hallucis muscle. When these muscles act together, a straight plantarflexion force is produced and the transverse–frontal plane forces are neutralized.
The function of the abductor hallucis muscle is to plantarflex, adduct, and invert the proximal phalanx. The reverse is true for the adductor hallucis muscle. When these muscles act together, a straight plantarflexion force is produced and the transverse–frontal plane forces are neutralized.
![]() When the adductor hallucis muscle gains the mechanical advantage, such as in removing the tibial sesamoid or pronation, a hallux valgus deformity may ensue. The sesamoids are pulled laterally, thus eroding the crista. The metatarsal head is pushed medially, stretching the medial ligaments, and the abductor hallucis slides beneath the metatarsal head, pronating the hallux.
When the adductor hallucis muscle gains the mechanical advantage, such as in removing the tibial sesamoid or pronation, a hallux valgus deformity may ensue. The sesamoids are pulled laterally, thus eroding the crista. The metatarsal head is pushed medially, stretching the medial ligaments, and the abductor hallucis slides beneath the metatarsal head, pronating the hallux.
![]() As the deformity progresses, the EHL and FHL have been shown to become a dynamic deforming force.
As the deformity progresses, the EHL and FHL have been shown to become a dynamic deforming force.
NATURAL HISTORY
![]() The progression of a hallux valgus deformity is usually gradual, but when multiple causative factors are present, progression can be more rapid. As the deformity progresses, the hallux drifts laterally and either over or under a stable second digit. Over time the second MTP joint can dislocate. As the hallux drifts laterally, it assumes less weight bearing and a diffuse callus may occur underneath the second metatarsal head.
The progression of a hallux valgus deformity is usually gradual, but when multiple causative factors are present, progression can be more rapid. As the deformity progresses, the hallux drifts laterally and either over or under a stable second digit. Over time the second MTP joint can dislocate. As the hallux drifts laterally, it assumes less weight bearing and a diffuse callus may occur underneath the second metatarsal head.
PATIENT HISTORY AND PHYSICAL FINDINGS
![]() The chief compliant of a bunion deformity is usually pain. Pain can be located over several areas in a bunion deformity: median eminence, dorsal first MTP joint, medial or lateral sesamoids, or impingement on the second digit.
The chief compliant of a bunion deformity is usually pain. Pain can be located over several areas in a bunion deformity: median eminence, dorsal first MTP joint, medial or lateral sesamoids, or impingement on the second digit.
![]() A thorough general medical history may include gout, osteoarthritis, rheumatoid arthritis, diabetes, or peripheral vascular disease.
A thorough general medical history may include gout, osteoarthritis, rheumatoid arthritis, diabetes, or peripheral vascular disease.
![]() Other important factors include style of shoes and if any shoe gear modification has been attempted, physical activity of the patient, and occupational demands.
Other important factors include style of shoes and if any shoe gear modification has been attempted, physical activity of the patient, and occupational demands.
![]() Patient expectations are also very important. Goals of surgery should include increasing activity and decreasing pain. Forewarning the patient of limitations after surgery is necessary, such as the possibility of not returning to tight fashionable shoes.
Patient expectations are also very important. Goals of surgery should include increasing activity and decreasing pain. Forewarning the patient of limitations after surgery is necessary, such as the possibility of not returning to tight fashionable shoes.
![]() The physical examination should start with the patient weight bearing to assess the bunion and lesser toe deformities and compare them to the other foot.
The physical examination should start with the patient weight bearing to assess the bunion and lesser toe deformities and compare them to the other foot.
![]() Evaluation of the vascular status is important. The perfusion is determined by palpating the posterior tibial and dorsal pedis arteries. Perfusion of a digit can be assessed by the capillary refill. Appropriate vascular studies such as transcutaneous oxygen, ankle–brachial index, digital pressures, and segmental pressures are useful when perfusion to the foot is in doubt.
Evaluation of the vascular status is important. The perfusion is determined by palpating the posterior tibial and dorsal pedis arteries. Perfusion of a digit can be assessed by the capillary refill. Appropriate vascular studies such as transcutaneous oxygen, ankle–brachial index, digital pressures, and segmental pressures are useful when perfusion to the foot is in doubt.
![]() The first MTP joint range of motion is assessed for crepitus, pain, or impingement if a dorsal spur is present. Motion is also assessed with the hallux in a corrected position to determine the degree of associated contracture of the soft tissues. Normal range of motion is 70 to 90 degrees of dorsiflexion. Joint range of motion is compared to that of the opposite foot.
The first MTP joint range of motion is assessed for crepitus, pain, or impingement if a dorsal spur is present. Motion is also assessed with the hallux in a corrected position to determine the degree of associated contracture of the soft tissues. Normal range of motion is 70 to 90 degrees of dorsiflexion. Joint range of motion is compared to that of the opposite foot.
![]() Transverse plane mobility is assessed by distracting the hallux while the metatarsal head is pushed laterally to see clinical reduction of the intermetatarsal angle.
Transverse plane mobility is assessed by distracting the hallux while the metatarsal head is pushed laterally to see clinical reduction of the intermetatarsal angle.
![]() The median eminence is assessed for its prominence and underlying bursa. Neuritic pain can be elicited from the nearby dorsal or plantar cutaneous nerves.
The median eminence is assessed for its prominence and underlying bursa. Neuritic pain can be elicited from the nearby dorsal or plantar cutaneous nerves.
![]() The tibial and fibular sesamoids are directly palpated while putting the joint through a range of motion to indicate intraarticular derangement.
The tibial and fibular sesamoids are directly palpated while putting the joint through a range of motion to indicate intraarticular derangement.
![]() The first tarsometatarsal joint excursion is assessed by grasping proximal to this joint and moving the first metatarsal and comparing it to the opposite foot. Normal range of motion is 10 mm of excursion. A hypermobile first ray is more than 15 mm of excursion.
The first tarsometatarsal joint excursion is assessed by grasping proximal to this joint and moving the first metatarsal and comparing it to the opposite foot. Normal range of motion is 10 mm of excursion. A hypermobile first ray is more than 15 mm of excursion.
![]() Range of motion of the hallux interphalangeal joint is evaluated in the transverse and sagittal plane, as well as joint quality.
Range of motion of the hallux interphalangeal joint is evaluated in the transverse and sagittal plane, as well as joint quality.
![]() Pain may also occur from lesser toe deformities or transfer lesions that may accompany the bunion deformity. A symptomatic intractable plantar keratoma beneath the second metatarsal head is present in the majority of patients.17Other associated problems include neuromas, corns, and tailor's bunion.
Pain may also occur from lesser toe deformities or transfer lesions that may accompany the bunion deformity. A symptomatic intractable plantar keratoma beneath the second metatarsal head is present in the majority of patients.17Other associated problems include neuromas, corns, and tailor's bunion.
IMAGING AND OTHER DIAGNOSTIC STUDIES
![]() The radiologic examination should include weight-bearing lateral, AP, and oblique views.
The radiologic examination should include weight-bearing lateral, AP, and oblique views.
![]() Several measurements are obtained using these radiographs to determine the severity of the bunion deformity, including the intermetatarsal 1–2 angle (IM1–2), hallux valgus angle (HVA), tibial sesamoid position, distal metatarsal articular angle (DMAA), and congruency of the first MTP joint.
Several measurements are obtained using these radiographs to determine the severity of the bunion deformity, including the intermetatarsal 1–2 angle (IM1–2), hallux valgus angle (HVA), tibial sesamoid position, distal metatarsal articular angle (DMAA), and congruency of the first MTP joint.
![]() The IM1–2 angle is determined by measuring the angle subtended by the lines bisecting the longitudinal axis of the first and second metatarsals.
The IM1–2 angle is determined by measuring the angle subtended by the lines bisecting the longitudinal axis of the first and second metatarsals.
![]() Normal is less than 9 degrees (FIG 1).
Normal is less than 9 degrees (FIG 1).
![]() The HVA is determined by measuring the angle subtended by the lines bisecting the first metatarsal and proximal phalanx of the hallux.
The HVA is determined by measuring the angle subtended by the lines bisecting the first metatarsal and proximal phalanx of the hallux.
![]() Normal is 15 degrees or less (FIG 2).
Normal is 15 degrees or less (FIG 2).
![]() Tibial sesamoid position describes the relationship of the tibial sesamoid to the bisection of the first metatarsal.
Tibial sesamoid position describes the relationship of the tibial sesamoid to the bisection of the first metatarsal.
![]() The position of the sesamoid is determined by a numerical sequence of one to seven with increasing deformity.
The position of the sesamoid is determined by a numerical sequence of one to seven with increasing deformity.
![]() Normal is a position of 1 to 3 (FIG 3).
Normal is a position of 1 to 3 (FIG 3).
![]() The DMAA is the angle subtended by a line representing the articular cartilage of the first metatarsal head and a perpendicular line to the bisection of the shaft of the first metatarsal.
The DMAA is the angle subtended by a line representing the articular cartilage of the first metatarsal head and a perpendicular line to the bisection of the shaft of the first metatarsal.
![]() Normal measures less than 8 degrees (FIG 4).
Normal measures less than 8 degrees (FIG 4).

FIG 1 • The intermetatarsal (IM) angle measures the splay between the first and second metatarsals.
![]() An increase in the DMAA may demonstrate a structural deformity in the head of the metatarsal.
An increase in the DMAA may demonstrate a structural deformity in the head of the metatarsal.
![]() The first MTP joint may be described as congruent, deviated, or subluxed.
The first MTP joint may be described as congruent, deviated, or subluxed.
![]() A congruent joint is one in which the cartilage surfaces of the first metatarsal head and proximal phalanx are parallel.
A congruent joint is one in which the cartilage surfaces of the first metatarsal head and proximal phalanx are parallel.
![]() A deviated joint is one in which the cartilage lines intersect at a point outside of the joint.
A deviated joint is one in which the cartilage lines intersect at a point outside of the joint.

FIG 2 • The hallux valgus angle (HVA) measures the angle formed between the proximal phalanx and first metatarsal.

FIG 3 • The tibial sesamoid position describes the position of the tibial sesamoid relative to the bisection of the first metatarsal.
![]() In a subluxed joint, the cartilage lines intersect within the joint (FIG 5).
In a subluxed joint, the cartilage lines intersect within the joint (FIG 5).
![]() Degenerative arthritis at the first MTP joint can be evaluated on each weight-bearing radiograph.
Degenerative arthritis at the first MTP joint can be evaluated on each weight-bearing radiograph.
DIFFERENTIAL DIAGNOSIS
![]() Metatarsus primus varus
Metatarsus primus varus
![]() Hallux varus
Hallux varus
![]() Gout
Gout
![]() Hallux rigidus
Hallux rigidus

FIG 4 • The distal metatarsal articular angle (DMAA) measures the relationship of the articular surface of the first metatarsal head to the bisection of the first metatarsal.

FIG 5 • A deviated joint in which the articular surfaces are not parallel with each other.
NONOPERATIVE MANAGEMENT
![]() Conservative treatment options for hallux valgus deformities are limited.
Conservative treatment options for hallux valgus deformities are limited.
![]() Shoe wear modifications such as an extra-wide and deep toebox can help accommodate the deformity. Also a soft upper leather can be stretched over the bunion to provide accommodation.
Shoe wear modifications such as an extra-wide and deep toebox can help accommodate the deformity. Also a soft upper leather can be stretched over the bunion to provide accommodation.
![]() Custom-made shoes may help individuals reluctant or unable to undergo a surgical procedure.
Custom-made shoes may help individuals reluctant or unable to undergo a surgical procedure.
![]() Bunion pads, night splints, and toe spacers tend to be of little use.
Bunion pads, night splints, and toe spacers tend to be of little use.
![]() A custom-made orthosis may be beneficial if an associated flatfoot deformity is present. The use of an orthosis has not been demonstrated to prevent a hallux valgus deformity or slow its progression. Others have proposed using orthoses postoperatively to prevent recurrence.
A custom-made orthosis may be beneficial if an associated flatfoot deformity is present. The use of an orthosis has not been demonstrated to prevent a hallux valgus deformity or slow its progression. Others have proposed using orthoses postoperatively to prevent recurrence.
SURGICAL MANAGEMENT
![]() Bunions can be classified by their severity. This classification is used to facilitate the decision-making process of how to treat the deformity.
Bunions can be classified by their severity. This classification is used to facilitate the decision-making process of how to treat the deformity.
![]() Mild bunion: HVA less than 20 degrees, congruent joint, IM angle less than 11 degrees. Pain is usually due to a medial eminence.
Mild bunion: HVA less than 20 degrees, congruent joint, IM angle less than 11 degrees. Pain is usually due to a medial eminence.
![]() Moderate bunion: HVA 20 to 40 degrees, incongruent joint, IM angle 11 to 18 degrees. The hallux is usually pronated and presses against the second digit.
Moderate bunion: HVA 20 to 40 degrees, incongruent joint, IM angle 11 to 18 degrees. The hallux is usually pronated and presses against the second digit.
![]() Severe bunion: HVA more than 40 degrees, subluxed joint, IM angle more than 18 degrees. Hallux is often overriding or underlapping the second digit; painful transfer lesion underneath the second metatarsal head; possible arthritic changes to the first MTP joint.
Severe bunion: HVA more than 40 degrees, subluxed joint, IM angle more than 18 degrees. Hallux is often overriding or underlapping the second digit; painful transfer lesion underneath the second metatarsal head; possible arthritic changes to the first MTP joint.
![]() The indications for hallux valgus surgery using the Mau osteotomy include:
The indications for hallux valgus surgery using the Mau osteotomy include:
![]() Painful moderate to severe bunion deformity
Painful moderate to severe bunion deformity
![]() Deformity unresponsive to conservative treatment
Deformity unresponsive to conservative treatment

FIG 6 • A well-padded thigh tourniquet set to 300 mm Hg.
Preoperative Planning
![]() Routine preoperative clearance is obtained via history and physical. This may include an electrocardiogram, chest radiograph, and laboratory workup.
Routine preoperative clearance is obtained via history and physical. This may include an electrocardiogram, chest radiograph, and laboratory workup.
![]() A prophylactic antibiotic of choice is given 30 minutes before the procedure. Also, one tablet of 200 mg celecoxib (Celebrex) is given.
A prophylactic antibiotic of choice is given 30 minutes before the procedure. Also, one tablet of 200 mg celecoxib (Celebrex) is given.
Positioning
![]() The patient is placed supine on the operating table with a bump placed under the contralateral hip.
The patient is placed supine on the operating table with a bump placed under the contralateral hip.
![]() A well-padded pneumatic thigh tourniquet is used and set to 300 mm Hg (FIG 6).
A well-padded pneumatic thigh tourniquet is used and set to 300 mm Hg (FIG 6).
Approach
![]() Typically two incisions are used to provide adequate exposure.
Typically two incisions are used to provide adequate exposure.
![]() The first incision is placed over the first web space and the second is placed on the medial aspect of the first metatarsal.
The first incision is placed over the first web space and the second is placed on the medial aspect of the first metatarsal.
![]() The second incision starts at the first tarsometatarsal joint and courses distal and medially over the first MTP joint for the distal soft tissue procedure (FIGS 7 AND 8).
The second incision starts at the first tarsometatarsal joint and courses distal and medially over the first MTP joint for the distal soft tissue procedure (FIGS 7 AND 8).

FIG 7 • Incision placed over the first web space for lateral joint release.

FIG 8 • Medial incision starts at the first tarsometatarsal joint and courses distal and medially for the distal soft tissue procedure.
TECHNIQUES
LATERAL RELEASE OF THE FIRST METATARSOPHALANGEAL JOINT
![]() Using an incision in the first web space (TECH FIG 1), perform the lateral release first. Carry dissection through the subcutaneous layer.
Using an incision in the first web space (TECH FIG 1), perform the lateral release first. Carry dissection through the subcutaneous layer.
![]() Typically the first structure incised is the superficial portion of the transverse ligament.
Typically the first structure incised is the superficial portion of the transverse ligament.
![]() Use blunt dissection to view the lateral first MTP joint and fibular sesamoid.
Use blunt dissection to view the lateral first MTP joint and fibular sesamoid.
![]() Release the adductor tendon from the plantar–lateral base of the proximal phalanx and fibular sesamoid (TECH FIG 2).
Release the adductor tendon from the plantar–lateral base of the proximal phalanx and fibular sesamoid (TECH FIG 2).
![]() Incise the deep portion of the transverse ligament. The lateral capsule of the first MTP joint is “pie crusted” and a varus stress is placed on the joint.
Incise the deep portion of the transverse ligament. The lateral capsule of the first MTP joint is “pie crusted” and a varus stress is placed on the joint.
TECH FIG 1 • The first structure identified in a lateral release is the superficial portion of the deep transverse metatarsal ligament.

TECH FIG 2 • Blunt dissection is carried deep to identify and release the adductor hallucis tendon.
MEDIAL CAPSULORRHAPHY
![]() Using a standard medial approach, perform an inverted-L capsulotomy. The alternative dorsal–medial skin incision, which is placed over the first dorsal metatarsal artery and nerve, can cause nerve irritation and entrapment.
Using a standard medial approach, perform an inverted-L capsulotomy. The alternative dorsal–medial skin incision, which is placed over the first dorsal metatarsal artery and nerve, can cause nerve irritation and entrapment.
![]() This allows exposure of the enlarged medial eminence and release of the stretched medial sesamoid suspensory ligament (TECH FIG 3). Remove the periosteum from the metatarsal head medially and dorsally but keep it intact at the neck plantarly to preserve the nutrient artery.
This allows exposure of the enlarged medial eminence and release of the stretched medial sesamoid suspensory ligament (TECH FIG 3). Remove the periosteum from the metatarsal head medially and dorsally but keep it intact at the neck plantarly to preserve the nutrient artery.

TECH FIG 3 • Release of the stretched medial sesamoid suspensory ligament.
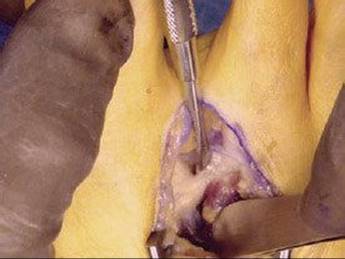
![]() Resect the medial eminence using a sagittal saw (TECH FIG 4).
Resect the medial eminence using a sagittal saw (TECH FIG 4).
![]() Take the eminence from dorsolateral to plantar–medial. Remove the eminence in this orientation to prevent staking of the metatarsal head and loss of the sagittal groove, which can lead to medial subluxation of the tibial sesamoid and promote hallux varus.
Take the eminence from dorsolateral to plantar–medial. Remove the eminence in this orientation to prevent staking of the metatarsal head and loss of the sagittal groove, which can lead to medial subluxation of the tibial sesamoid and promote hallux varus.

TECH FIG 4 • Minimal exostectomy of the medial eminence.
MAU OSTEOTOMY
![]() Carry the dissection deep to the first metatarsal shaft. The skin incision can be placed slightly plantar to the first metatarsal to avoid surrounding neurovascular structures such as the first dorsal metatarsal artery and nerve. With this incision, a potentially nonpainful scar results as the incision is not placed directly over bone. The extensor hallucis longus tendon is not encountered with this incision and is retracted safely.
Carry the dissection deep to the first metatarsal shaft. The skin incision can be placed slightly plantar to the first metatarsal to avoid surrounding neurovascular structures such as the first dorsal metatarsal artery and nerve. With this incision, a potentially nonpainful scar results as the incision is not placed directly over bone. The extensor hallucis longus tendon is not encountered with this incision and is retracted safely.
![]() Identify the first tarsometatarsal joint but do not disturb the capsule. An 18-gauge needle can be placed in the joint for reference.
Identify the first tarsometatarsal joint but do not disturb the capsule. An 18-gauge needle can be placed in the joint for reference.
![]() Starting 1 cm from the first tarsometatarsal joint, reflect the periosteum plantar-proximal to dorsal-distal only in line with the osteotomy, thereby preserving the rest of the periosteum (TECH FIG 5). Much of the periosteum is retained to promote adequate bone healing.
Starting 1 cm from the first tarsometatarsal joint, reflect the periosteum plantar-proximal to dorsal-distal only in line with the osteotomy, thereby preserving the rest of the periosteum (TECH FIG 5). Much of the periosteum is retained to promote adequate bone healing.
![]() The osteotomy does not incorporate the entire metatarsal shaft as does the traditional Mau osteotomy. The osteotomy ends in the midshaft of the first metatarsal.
The osteotomy does not incorporate the entire metatarsal shaft as does the traditional Mau osteotomy. The osteotomy ends in the midshaft of the first metatarsal.
![]() Complete the osteotomy with a sagittal saw parallel to the weight-bearing surface to prevent unwanted dorsal angulation of the first metatarsal. The Mau is started proximal-plantar and ends distal-dorsal (TECH FIG 6). A self-retaining retractor is useful to protect the surrounding neurovascular and tendinous structures. Using the straight medial incision avoids tendinous structures and allows excellent visualization of the medial metatarsal shaft to complete the osteotomy. To maintain complete control while completing the osteotomy, a smooth guide pin for the selected cannulated screw can be placed perpendicular across the completed proximal portion of the osteotomy. Then the osteotomy can be completed without fear of losing the orientation.
Complete the osteotomy with a sagittal saw parallel to the weight-bearing surface to prevent unwanted dorsal angulation of the first metatarsal. The Mau is started proximal-plantar and ends distal-dorsal (TECH FIG 6). A self-retaining retractor is useful to protect the surrounding neurovascular and tendinous structures. Using the straight medial incision avoids tendinous structures and allows excellent visualization of the medial metatarsal shaft to complete the osteotomy. To maintain complete control while completing the osteotomy, a smooth guide pin for the selected cannulated screw can be placed perpendicular across the completed proximal portion of the osteotomy. Then the osteotomy can be completed without fear of losing the orientation.
![]() After completing the osteotomy, rotate the distal fragment. Optimal rotation of the osteotomy may be facilitated by placing a large reduction bone clamp on the first metatarsal head and neck of the second metatarsal to help reduce the IM1–2 angle (TECH FIG 7).
After completing the osteotomy, rotate the distal fragment. Optimal rotation of the osteotomy may be facilitated by placing a large reduction bone clamp on the first metatarsal head and neck of the second metatarsal to help reduce the IM1–2 angle (TECH FIG 7).

TECH FIG 5 • Identification of the first tarsometatarsal joint (pick-ups) and line of the osteotomy 1 cm distal to the joint.
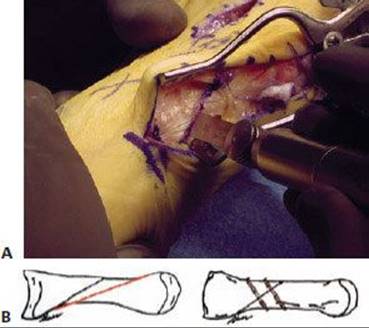
TECH FIG 6 • A. Sagittal saw is placed parallel to the weightbearing surface of the foot and the osteotomy is completed from proximal-plantar to distal-dorsal. B. The traditional Mau osteotomy (red line) and the slight modification (black line). The modified Mau does not incorporate the entire metatarsal shaft as does the traditional Mau osteotomy. The modified Mau osteotomy with two-screw fixation.
![]() Place two temporary Kirschner wires (0.025 inch) from dorsal to plantar perpendicular to the osteotomy site (TECH FIG 8).
Place two temporary Kirschner wires (0.025 inch) from dorsal to plantar perpendicular to the osteotomy site (TECH FIG 8).
![]() Reduction of the IM1–2 angle is mostly obtained by rotation of the distal fragment. It is acceptable to allow slight lateral translation of the distal fragment relative to the proximal fragment to further correct the IM angle.
Reduction of the IM1–2 angle is mostly obtained by rotation of the distal fragment. It is acceptable to allow slight lateral translation of the distal fragment relative to the proximal fragment to further correct the IM angle.
![]() We recommend using intraoperative fluoroscopy to confirm proper position of the first metatarsal head over the tibial sesamoids, congruent joint alignment, and satisfactory orientation of the osteotomy. We use a towel clip to provisionally advance the capsule into the desired position to assess sesamoid alignment (TECH FIG 9). Redundant capsular tissue is excised and optimal correction is obtained with a tibial sesamoid position less than 2 and an IM1–2 angle less than 9 degrees. About 4 mm of redundant capsule is removed from the inverted-L portion of the capsulotomy to help reduce and advance the sesamoids upon closure. With larger deformities, more capsule may need to be removed to reduce the tibial sesamoid position adequately. To correct pronation of the hallux, the towel clip can be rotated to correct the deformity, and a double simple suture is placed to maintain the correction.
We recommend using intraoperative fluoroscopy to confirm proper position of the first metatarsal head over the tibial sesamoids, congruent joint alignment, and satisfactory orientation of the osteotomy. We use a towel clip to provisionally advance the capsule into the desired position to assess sesamoid alignment (TECH FIG 9). Redundant capsular tissue is excised and optimal correction is obtained with a tibial sesamoid position less than 2 and an IM1–2 angle less than 9 degrees. About 4 mm of redundant capsule is removed from the inverted-L portion of the capsulotomy to help reduce and advance the sesamoids upon closure. With larger deformities, more capsule may need to be removed to reduce the tibial sesamoid position adequately. To correct pronation of the hallux, the towel clip can be rotated to correct the deformity, and a double simple suture is placed to maintain the correction.

TECH FIG 7 • Operative and fluoroscopy images showing reduction of IM1–2 angle with large reduction bone clamps. The clamp is placed medially at the first metatarsal head and laterally around the second metatarsal head.

TECH FIG 8 • Temporary fixation of the osteotomy with two parallel Kirschner wires from dorsal to plantar.
![]() We use two 2.5- or 3.0-mm headless cannulated screws for final fixation.
We use two 2.5- or 3.0-mm headless cannulated screws for final fixation.
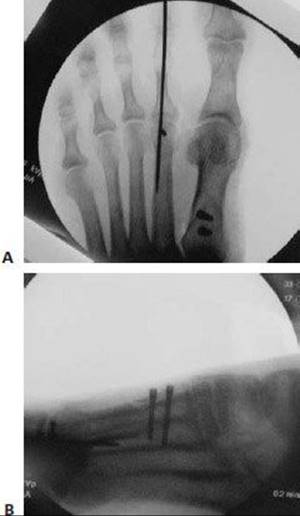
TECH FIG 9 • Intraoperative fluoroscopy of AP and lateral foot, showing final fixation and excellent reduction of the IM1–2 angle.
CLOSURE
![]() To complete the medial capsulorrhaphy, close the capsule using a double simple suture technique with 0-0 absorbable suture (TECH FIG 10).
To complete the medial capsulorrhaphy, close the capsule using a double simple suture technique with 0-0 absorbable suture (TECH FIG 10).
![]() Placing a sponge in the first interspace while closing the capsule will splint the toe in the corrected position.
Placing a sponge in the first interspace while closing the capsule will splint the toe in the corrected position.
![]() Close the subcutaneous layer with 2-0 absorbable suture. The skin is closed based on the surgeon's preference, with either a running subcuticular closure with 5-0 absorbable suture or simple interrupted sutures with 3-0 nylon.
Close the subcutaneous layer with 2-0 absorbable suture. The skin is closed based on the surgeon's preference, with either a running subcuticular closure with 5-0 absorbable suture or simple interrupted sutures with 3-0 nylon.
![]() Place a soft toe spica dressing by dividing a sponge in thirds and wrapping lateral to medial around the hallux to maintain correction. Use caution to prevent aggressive splinting, which can cause overcorrection and potential hallux varus.
Place a soft toe spica dressing by dividing a sponge in thirds and wrapping lateral to medial around the hallux to maintain correction. Use caution to prevent aggressive splinting, which can cause overcorrection and potential hallux varus.
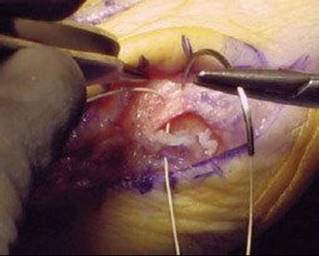
TECH FIG 10 • Completion of the medial capsulorrhaphy with capsule repaired in a double simple suture technique with 0-0 absorbable suture.
POSTOPERATIVE CARE
![]() The patient is placed in a soft toe spica dressing after surgery and instructed to remain partially weight bearing on the heel in a surgical shoe.
The patient is placed in a soft toe spica dressing after surgery and instructed to remain partially weight bearing on the heel in a surgical shoe.
![]() Two weeks after surgery the sutures are removed and the patient is fully weight bearing in a surgical shoe.
Two weeks after surgery the sutures are removed and the patient is fully weight bearing in a surgical shoe.
![]() Three weight-bearing radiographs (AP, lateral, oblique) are obtained at each visit until bony healing of the osteotomy site is seen.
Three weight-bearing radiographs (AP, lateral, oblique) are obtained at each visit until bony healing of the osteotomy site is seen.
OUTCOMES
![]() After a proximal osteotomy and distal soft tissue release, 90% to 95% patient satisfaction rates have been reported.3,5,17
After a proximal osteotomy and distal soft tissue release, 90% to 95% patient satisfaction rates have been reported.3,5,17
![]() One study reviewed retrospective results of the Mau osteotomy and found excellent correction of a moderate to severe bunion deformity in 24 patients.8
One study reviewed retrospective results of the Mau osteotomy and found excellent correction of a moderate to severe bunion deformity in 24 patients.8
![]() Biomechanical studies using sawbones and fresh frozen cadaver models showed superior stability with the Mau in terms of fatigue, strength, and stiffness compared to other proximal osteotomies.1,22 The Mau osteotomy is an inherently stable osteotomy that allows early postoperative weight bearing without the need for cast immobilization as required for other proximal osteotomies due to complications such as dorsal malunion and nonunion. The Mau is a stable osteotomy due to the dorsal shelf to help reduce dorsal displacement forces and broad bony apposition to facilitate twoscrew fixation.
Biomechanical studies using sawbones and fresh frozen cadaver models showed superior stability with the Mau in terms of fatigue, strength, and stiffness compared to other proximal osteotomies.1,22 The Mau osteotomy is an inherently stable osteotomy that allows early postoperative weight bearing without the need for cast immobilization as required for other proximal osteotomies due to complications such as dorsal malunion and nonunion. The Mau is a stable osteotomy due to the dorsal shelf to help reduce dorsal displacement forces and broad bony apposition to facilitate twoscrew fixation.
FIG 9 • Preoperative weight-bearing appearance of the bunion deformity.
![]() The authors performed a follow-up study comparing the Mau and crescentic osteotomies. Both osteotomies showed comparable correction of the moderate to severe bunion deformity, but significantly more complications were associated with the crescentic osteotomy. Complications included dorsal malunion, placement of screws within the tarsometatarsal joint, and nonunion.7
The authors performed a follow-up study comparing the Mau and crescentic osteotomies. Both osteotomies showed comparable correction of the moderate to severe bunion deformity, but significantly more complications were associated with the crescentic osteotomy. Complications included dorsal malunion, placement of screws within the tarsometatarsal joint, and nonunion.7

FIG 10 • Final postoperative appearance and closure with 3-0 suture.

FIG 11 • Preoperative weight-bearing AP and lateral foot radiographs.
![]() The Mau osteotomy is technically easier to perform than other proximal osteotomies with fewer complications, as seen in two studies, and excellent correction of a bunion deformity (FIGS 9–12).
The Mau osteotomy is technically easier to perform than other proximal osteotomies with fewer complications, as seen in two studies, and excellent correction of a bunion deformity (FIGS 9–12).
COMPLICATIONS
![]() One of the most common complications after bunion surgery is recurrence. This may be due to selection of the inappropriate procedure to correct the moderate to severe bunion deformity or intraoperative failure to obtain an adequate alignment to correct the deformity.
One of the most common complications after bunion surgery is recurrence. This may be due to selection of the inappropriate procedure to correct the moderate to severe bunion deformity or intraoperative failure to obtain an adequate alignment to correct the deformity.
![]() Hallux varus is a complication that occurs less often than recurrence. It occurs as a result of overcorrection of the deformity and is much more difficult to correct.
Hallux varus is a complication that occurs less often than recurrence. It occurs as a result of overcorrection of the deformity and is much more difficult to correct.
![]() Other complications include shortening, dorsal malunion, and transfer lesions, which can occur with all proximal osteotomies.
Other complications include shortening, dorsal malunion, and transfer lesions, which can occur with all proximal osteotomies.

FIG 12 • Postoperative weight-bearing AP and lateral foot radiographs showing excellent reduction of the IM1–2 angle.
REFERENCES
· Acevedo JI, Sammarco VJ, Boucher HR, et al. Mechanical comparison of cyclic loading in five different first metatarsal shaft osteotomies. Foot Ankle Int 2002;23:711–716.
· Brahm SM. Shape of the first metatarsal head in hallux rigidus and hallux valgus. J Am Podiatr Med Assoc 1988;78:300.
· Chiodo C, Schon L, Myerson MS, et al. Clinical results with the Ludloff osteotomy for correction of adult hallux valgus. Foot Ankle Int 2004;25:532–536.
· Coughlin MJ. Juvenile hallux valgus: etiology and treatment. Foot Ankle Int 1995;16:682–697.
· Easley ME, Kiebzak GM, Davis WH, et al. Prospective, randomized comparison of proximal crescentic and proximal chevron osteotomies for correction of hallux valgus deformity. Foot Ankle Int 1996;17:307–316.
· Ellis VH. A method of correcting metatarsus primus varus. J Bone Joint Surg Br 1951;33B:415.
· Glover JP, Hyer CF, Berlet GC, et al. A comparison of crescentic and Mau osteotomies for correction of hallux valgus. J Foot Ankle Surg 2008;47:103–111.
· Glover JP, Hyer CF, Berlet GC, et al. Early results of the Mau osteotomy for correction of moderate to severe hallux valgus. J Foot Ankle Surg 2008;47:237–242.
· Greenburg GS. Relationship of hallux abductus angle and first metatarsal angle to severity of pronation. J Am Podiatr Assoc 1979;69:29.
· Hardy RH, Clapham JR. Observations on hallux valgus. J Bone Joint Surg Br 1951;33B:376.
· Hoffman P. Conclusions drawn from a comparative study of the feet of barefooted and shoe-wearing peoples. Am J Orthop Surg 1905;3:105.
· Hohmann G. Der hallux valgus und die uebrigen Zchenverkruemmungen. Ergeb Chir Orthop 1925;18:308–348.
· Hyer CF, Philbin TM. The obliquity of the first metatarsal base. Foot Ankle Int 2004;25:728–732.
· Johnston O. Further studies of the inheritance of hand and foot anomalies. Clin Orthop 1956;8:146.
· Kato T, Watanabe S. The etiology of hallux valgus in Japan. Clin Orthop Relat Res 1981;157:78.
· Kirkup JR, Vidigal E, Jacoby RK, et al. The hallux and rheumatoid arthritis. Acta Orthop Scand 1977;48:527.
· Mann RA, Rudicel S, Graves SC, et al. Hallux valgus repair utilizing a distal soft tissue procedure and proximal metatarsal osteotomy: a long-term follow-up. J Bone Joint Surg Am 1992;74A:124–129.
· Meyer M. A comparison of hallux abducto valgus in two ancient populations. J Am Podiatr Assoc 1979;69:65.
· Ross FD. The relationship of abnormal foot pronation to hallux abducto valgus, a pilot study. Prosthet Orthotics Int 1986;10:72.
· Rubin LM. Rheumatoid arthritis with hallux valgus. J Am Podiatr Assoc 1968;58:481.
· Stevenson MR. A study of the correlation between neutral calcaneal stance position and relaxed calcaneal stance position in the development of hallux abducto valgus. Master's thesis, 1991.
· Trnka HJ, Parks BG, Ivanic G, et al. Six first metatarsal shaft osteotomies: mechanical and immobilization comparisons. Clin Orthop Relat Res 2000;381:256–265.
· Truslow W. Metatarsus primus varus or hallux valgus? J Bone Joint Surg Am 1925;7A:98.
· Vidigal EC, Kirkup JR, Jacoby RK, et al. The rheumatoid foot: pathomechanics of hallux deformities. Rev Assoc Med Bras 1980;26:23.
· Wallace WA. Predicting hallux abducto valgus. J Am Podiatr Med Assoc 1990;80:509.