Michael M. Stephens and Ronan McKeown
DEFINITION
![]() Arthrosis of the first metatarsophalangeal (MTP) joint is commonly seen in osteoarthritis (hallux rigidus), rheumatoid disease, and gout.
Arthrosis of the first metatarsophalangeal (MTP) joint is commonly seen in osteoarthritis (hallux rigidus), rheumatoid disease, and gout.
![]() The indication for surgical treatment of the first MTP joint is pain where conservative treatment has failed.
The indication for surgical treatment of the first MTP joint is pain where conservative treatment has failed.
![]() Arthrodesis of the first MTP joint is the surgical treatment of choice in rheumatoid disease and is indicated in hallux rigidus when the disease is advanced.
Arthrodesis of the first MTP joint is the surgical treatment of choice in rheumatoid disease and is indicated in hallux rigidus when the disease is advanced.
![]() Many techniques in preparation of the joint exist to provide good cancellous apposition:
Many techniques in preparation of the joint exist to provide good cancellous apposition:
![]() Flat cuts: these make accurate positioning of the toe difficult
Flat cuts: these make accurate positioning of the toe difficult
![]() Cone or peg socket: this leads to excessive shortening
Cone or peg socket: this leads to excessive shortening
![]() Ball and socket: this results in minimal shortening and has the additional benefit of ease of adjustment in positioning the toe
Ball and socket: this results in minimal shortening and has the additional benefit of ease of adjustment in positioning the toe
![]() Various methods of fixation have been described. The most biomechanically advantageous method of fixation has been shown to be a dorsal plate and compression screw.2,3
Various methods of fixation have been described. The most biomechanically advantageous method of fixation has been shown to be a dorsal plate and compression screw.2,3
ANATOMY
![]() The first MTP joint is a ball-and-socket joint.
The first MTP joint is a ball-and-socket joint.
![]() The normal hallux valgus angle is less than 15 degrees.
The normal hallux valgus angle is less than 15 degrees.
![]() The metatarsal inclination angle relative to weight bearing is usually 25 to 30 degrees but varies with foot type (greater for cavus, less for planus) (FIG 1).
The metatarsal inclination angle relative to weight bearing is usually 25 to 30 degrees but varies with foot type (greater for cavus, less for planus) (FIG 1).
![]() The final position of the arthrodesed first MTP joint must allow for heel rise during the late stance phase of gait.
The final position of the arthrodesed first MTP joint must allow for heel rise during the late stance phase of gait.
![]() The position can be checked by applying a flat surface to the sole of the foot. The tip of the toe should clear the surface with the interphalangeal joint in full extension and should touch the surface with the interphalangeal joint in 45 to 60 degrees of flexion.
The position can be checked by applying a flat surface to the sole of the foot. The tip of the toe should clear the surface with the interphalangeal joint in full extension and should touch the surface with the interphalangeal joint in 45 to 60 degrees of flexion.
PATHOGENESIS
![]() Primary osteoarthritis (hallux rigidus) and the inflammatory arthritides (rheumatoid, gout, psoriatic arthritis) account for the majority of causative factors.
Primary osteoarthritis (hallux rigidus) and the inflammatory arthritides (rheumatoid, gout, psoriatic arthritis) account for the majority of causative factors.
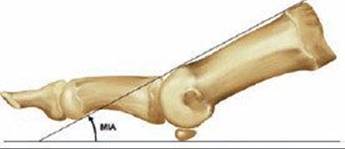
FIG 1 • Metatarsal inclination angle.
![]() Secondary osteoarthritis arises from mechanical abnormalities (hallux valgus and varus) and trauma resulting in joint incongruity and excessive cartilage wear.
Secondary osteoarthritis arises from mechanical abnormalities (hallux valgus and varus) and trauma resulting in joint incongruity and excessive cartilage wear.
NATURAL HISTORY
![]() The natural history of first MTP joint arthrosis is related to its cause.
The natural history of first MTP joint arthrosis is related to its cause.
![]() Hallux rigidus is a progressive disease process and the joint will deteriorate with time, but the patient's symptoms may not show the same deterioration.
Hallux rigidus is a progressive disease process and the joint will deteriorate with time, but the patient's symptoms may not show the same deterioration.
![]() Progression of arthrosis secondary to the inflammatory arthritides will be related to the activity of the disease.
Progression of arthrosis secondary to the inflammatory arthritides will be related to the activity of the disease.
PATIENT HISTORY AND PHYSICAL FINDINGS
![]() In true hallux rigidus, patients experience an insidious onset of pain, swelling, and stiffness in the first MTP joint that is aggravated by activity (eg, walking, running).
In true hallux rigidus, patients experience an insidious onset of pain, swelling, and stiffness in the first MTP joint that is aggravated by activity (eg, walking, running).
![]() Lateral forefoot pain due to overload may develop as the foot supinates to avoid dorsiflexion of the first ray just before and immediately after heel rise.
Lateral forefoot pain due to overload may develop as the foot supinates to avoid dorsiflexion of the first ray just before and immediately after heel rise.
![]() A comprehensive physical examination is required to enable diagnosis and selection of correct surgical procedure.
A comprehensive physical examination is required to enable diagnosis and selection of correct surgical procedure.
![]() The physician should palpate the MTP joint for tenderness; dorsal or dorsolateral osteophytes (cheilus) may be palpable and tender.
The physician should palpate the MTP joint for tenderness; dorsal or dorsolateral osteophytes (cheilus) may be palpable and tender.
![]() The physician should examine the range of motion of the MTP and interphalangeal joints. Restriction in dorsiflexion but full plantarflexion may indicate that dorsiflexion osteotomy of proximal phalanx may improve the dorsiflexion arc.
The physician should examine the range of motion of the MTP and interphalangeal joints. Restriction in dorsiflexion but full plantarflexion may indicate that dorsiflexion osteotomy of proximal phalanx may improve the dorsiflexion arc.
![]() The grind test is not normally painful unless an osteochondral defect is present or degeneration is advanced. If painful, then arthrodesis is indicated.
The grind test is not normally painful unless an osteochondral defect is present or degeneration is advanced. If painful, then arthrodesis is indicated.
![]() The physician should observe the patient's walking gait. Avoidance of weight bearing on the hallux implies pain. Callus may be present under the lesser metatarsals.
The physician should observe the patient's walking gait. Avoidance of weight bearing on the hallux implies pain. Callus may be present under the lesser metatarsals.
![]() The physician should palpate for posterior tibial and dorsalis pedis pulses. Peripheral vascular disease is a contraindication to surgery. If suspected, vascular assessment and treatment is required first.
The physician should palpate for posterior tibial and dorsalis pedis pulses. Peripheral vascular disease is a contraindication to surgery. If suspected, vascular assessment and treatment is required first.
![]() The physician should palpate and move the tarsometatarsal joint. Arthrosis of the tarsometatarsal joint is a relative contraindication to arthrodesis of the first MTP joint. The examiner should also palpate and move the interphalangeal joint. Arthrosis of the interphalangeal joint is a contraindication to arthrodesis of the first MTP joint.
The physician should palpate and move the tarsometatarsal joint. Arthrosis of the tarsometatarsal joint is a relative contraindication to arthrodesis of the first MTP joint. The examiner should also palpate and move the interphalangeal joint. Arthrosis of the interphalangeal joint is a contraindication to arthrodesis of the first MTP joint.
IMAGING AND OTHER DIAGNOSTIC STUDIES
![]() Weight-bearing anteroposterior and lateral radiographs should be obtained before surgery.
Weight-bearing anteroposterior and lateral radiographs should be obtained before surgery.
![]() The severity of the arthrosis can be assessed and any coexisting forefoot pathology identified and addressed at the time of surgery.
The severity of the arthrosis can be assessed and any coexisting forefoot pathology identified and addressed at the time of surgery.
![]() The hallux valgus angle and the metatarsal inclination angle should be measured accurately.
The hallux valgus angle and the metatarsal inclination angle should be measured accurately.
![]() The lateral radiograph shows the cheilus and any narrowing of the joint space (either dorsally or throughout).
The lateral radiograph shows the cheilus and any narrowing of the joint space (either dorsally or throughout).
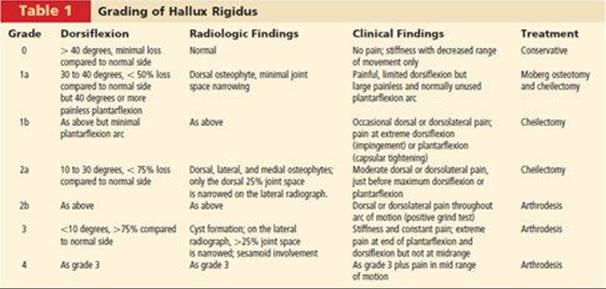
![]() Hallux rigidus can be graded using the clinical and radiologic information obtained.
Hallux rigidus can be graded using the clinical and radiologic information obtained.
![]() We have created a seven-point clinicoradiologic grading system (adapted from Coughlin and Shurnas1) that correlates the severity of the disease (symptoms, clinical examination, and radiologic findings) with the appropriate surgical procedure (Table 1).
We have created a seven-point clinicoradiologic grading system (adapted from Coughlin and Shurnas1) that correlates the severity of the disease (symptoms, clinical examination, and radiologic findings) with the appropriate surgical procedure (Table 1).
NONOPERATIVE MANAGEMENT
![]() Nonoperative management encompasses activity modification, weight loss, analgesic and anti-inflammatory medication (oral and intra-articular), physiotherapy (tendo Achilles and hamstring stretching), and shoe modification.
Nonoperative management encompasses activity modification, weight loss, analgesic and anti-inflammatory medication (oral and intra-articular), physiotherapy (tendo Achilles and hamstring stretching), and shoe modification.
![]() Shoe modification can involve a carbon fiber extended insole with cutouts for the lesser toes, metal stiffeners in the last, and a forefoot rocker sole.
Shoe modification can involve a carbon fiber extended insole with cutouts for the lesser toes, metal stiffeners in the last, and a forefoot rocker sole.
SURGICAL MANAGEMENT
![]() Arthrodesis of the first MTP joint does not restore normal anatomy or gait pattern. The patient should be counseled as to the surgical goals and optimal outcome in order to have realistic expectations of the surgery.
Arthrodesis of the first MTP joint does not restore normal anatomy or gait pattern. The patient should be counseled as to the surgical goals and optimal outcome in order to have realistic expectations of the surgery.
![]() Absolute contraindications to first MTP joint fusion include active infection, peripheral vascular disease, and arthrosis of the interphalangeal joint.
Absolute contraindications to first MTP joint fusion include active infection, peripheral vascular disease, and arthrosis of the interphalangeal joint.
![]() Relative contraindications to first MTP joint fusion include degeneration of the first tarsometatarsal joint and peripheral neuropathy.
Relative contraindications to first MTP joint fusion include degeneration of the first tarsometatarsal joint and peripheral neuropathy.
Preoperative Planning
![]() Initial assessment should include examination of circulation, sensation, the first tarsometatarsal joint, the interphalangeal joint, and any previous surgical incisions about the foot.
Initial assessment should include examination of circulation, sensation, the first tarsometatarsal joint, the interphalangeal joint, and any previous surgical incisions about the foot.
![]() It may be necessary to consult with the patient's rheumatologist to reduce or stop immunosuppressant drugs before surgery.
It may be necessary to consult with the patient's rheumatologist to reduce or stop immunosuppressant drugs before surgery.
![]() Preoperative weight-bearing AP and lateral radiographs should be obtained.
Preoperative weight-bearing AP and lateral radiographs should be obtained.
Positioning
![]() We prefer to position the patient supine with the heels at the end of the operating table. A thigh tourniquet is inflated to 350 mm Hg after prophylactic intravenous antibiotics have been given and the limb has been exsanguinated. The foot and leg are then prepared and draped above the knee in a routine manner.
We prefer to position the patient supine with the heels at the end of the operating table. A thigh tourniquet is inflated to 350 mm Hg after prophylactic intravenous antibiotics have been given and the limb has been exsanguinated. The foot and leg are then prepared and draped above the knee in a routine manner.
![]() The end of the table is dropped 20 to 30 degrees. The surgeon sits at the end of the table.
The end of the table is dropped 20 to 30 degrees. The surgeon sits at the end of the table.
Approach
![]() A dorsal approach is recommended regardless of previous scars. Care should be taken to avoid the dorsal cutaneous nerve and extensor hallucis longus. The former is retracted medially and the latter laterally, so they are protected.
A dorsal approach is recommended regardless of previous scars. Care should be taken to avoid the dorsal cutaneous nerve and extensor hallucis longus. The former is retracted medially and the latter laterally, so they are protected.
TECHNIQUES
ARTHRODESIS OF THE FIRST METATARSOPHALANGEAL JOINT USING A DORSAL TITANIUM CONTOURED PLATE (HALLU-S PLATE)
Exposure
![]() Make a dorsal slightly curved incision just medial to the extensor hallucis longus tendon and lateral to the dorsal cutaneous nerve, extending from the middle of the shaft of the first metatarsal to the interphalangeal joint.
Make a dorsal slightly curved incision just medial to the extensor hallucis longus tendon and lateral to the dorsal cutaneous nerve, extending from the middle of the shaft of the first metatarsal to the interphalangeal joint.
![]() Retract the extensor hallucis longus tendon laterally.
Retract the extensor hallucis longus tendon laterally.
![]() Make a capsulotomy in the same plane and expose the joint.
Make a capsulotomy in the same plane and expose the joint.
![]() Perform a synovectomy.
Perform a synovectomy.
![]() Release the medial and lateral soft tissues to allow maximum plantarflexion of the proximal phalanx, exposing both articular surfaces.
Release the medial and lateral soft tissues to allow maximum plantarflexion of the proximal phalanx, exposing both articular surfaces.
Joint Preparation
![]() Excise any large medial eminence or osteophyte with an oscillating saw.
Excise any large medial eminence or osteophyte with an oscillating saw.
![]() Excise osteophytes on the proximal phalanx to find the true center and size of the articular surface.
Excise osteophytes on the proximal phalanx to find the true center and size of the articular surface.
![]() Size the articular surface of the proximal phalanx to determine the correct convex reamer required.
Size the articular surface of the proximal phalanx to determine the correct convex reamer required.
![]() Insert a 1.6-mm Kirschner wire through the center of the articular surface of the proximal phalanx and pass it in line with its long axis. In osteoporotic bone the wire should cross the interphalangeal joint into the distal phalanx to prevent toggling of the wire, leading to eccentric reaming.
Insert a 1.6-mm Kirschner wire through the center of the articular surface of the proximal phalanx and pass it in line with its long axis. In osteoporotic bone the wire should cross the interphalangeal joint into the distal phalanx to prevent toggling of the wire, leading to eccentric reaming.
![]() Guide the sized convex reamer over the Kirschner wire and ream the surface sparingly to expose subchondral cancellous bone (TECH FIG 1).
Guide the sized convex reamer over the Kirschner wire and ream the surface sparingly to expose subchondral cancellous bone (TECH FIG 1).
![]() Remove the Kirschner wire. Remove any fine collar of cartilage remaining around the wire entry hole. Insert the wire into the center of the articular surface of the first metatarsal and advance it along its long axis. If the bone is osteoporotic then the wire should cross the tarsometatarsal joint.
Remove the Kirschner wire. Remove any fine collar of cartilage remaining around the wire entry hole. Insert the wire into the center of the articular surface of the first metatarsal and advance it along its long axis. If the bone is osteoporotic then the wire should cross the tarsometatarsal joint.
![]() Use the matched-sized concave reamer in a similar fashion to expose the subchondral cancellous bone of the metatarsal head (TECH FIG 2). Remove the wire and retain all fragments of bone in the reamer.
Use the matched-sized concave reamer in a similar fashion to expose the subchondral cancellous bone of the metatarsal head (TECH FIG 2). Remove the wire and retain all fragments of bone in the reamer.

TECH FIG 1 • Reaming the articular surface of the proximal phalanx.

TECH FIG 2 • Reaming the articular surface of the metatarsal head.
Positioning
![]() Approximate the position of the hallux in relation to the first metatarsal and fix the position temporarily with an obliquely directed Kirschner wire. The ideal position is 20 to 25 degrees of dorsiflexion of the proximal phalanx in relation to the first metatarsal axis. The valgus angle should be 10 to 15 degrees. However, a gap of 3 to 5 mm must be left between the hallux and the second toe. The rotation of the hallux should be neutral so that the arc of rotation of the interphalangeal joint is at 90 degrees to the weight-bearing surface.
Approximate the position of the hallux in relation to the first metatarsal and fix the position temporarily with an obliquely directed Kirschner wire. The ideal position is 20 to 25 degrees of dorsiflexion of the proximal phalanx in relation to the first metatarsal axis. The valgus angle should be 10 to 15 degrees. However, a gap of 3 to 5 mm must be left between the hallux and the second toe. The rotation of the hallux should be neutral so that the arc of rotation of the interphalangeal joint is at 90 degrees to the weight-bearing surface.
![]() Confirm the correct position of the hallux by placing a flat surface against the sole of the foot and bringing the ankle to 90 degrees. In this position, with the interphalangeal joint in full extension, the tip of the hallux lies about 1 cm from the flat surface. When the interphalangeal joint is flexed to 45 to 60 degrees, its tip comes in contact with the plantar surface. This enables the foot to rock at the MTP joint on heel rise (TECH FIG 3).
Confirm the correct position of the hallux by placing a flat surface against the sole of the foot and bringing the ankle to 90 degrees. In this position, with the interphalangeal joint in full extension, the tip of the hallux lies about 1 cm from the flat surface. When the interphalangeal joint is flexed to 45 to 60 degrees, its tip comes in contact with the plantar surface. This enables the foot to rock at the MTP joint on heel rise (TECH FIG 3).

TECH FIG 3 • Foot plate to check arthrodesis position
Fixation
![]() Insert an oblique 2.7-mm compression screw of appropriate length from distal medial to proximal lateral across the MTP joint.
Insert an oblique 2.7-mm compression screw of appropriate length from distal medial to proximal lateral across the MTP joint.
![]() Size and secure the plate on the dorsal aspect of the joint with a Kirschner wire and fix it with six 2.7-mm self-tapping screws (TECH FIGS 4 AND 5). The plate is available in three side-specific (left and right) sizes (small for a small hallux, medium for a larger hallux, large for revision arthrodesis).
Size and secure the plate on the dorsal aspect of the joint with a Kirschner wire and fix it with six 2.7-mm self-tapping screws (TECH FIGS 4 AND 5). The plate is available in three side-specific (left and right) sizes (small for a small hallux, medium for a larger hallux, large for revision arthrodesis).

TECH FIG 4 • Plate secured with temporary Kirschner wire.
![]() Close the wound in layers over a drain.
Close the wound in layers over a drain.
![]() Apply a compression dressing.
Apply a compression dressing.

TECH FIG 5 • Screw fixation of plate.
POSTOPERATIVE CARE
![]() If this technique is performed as an isolated procedure we do not use a cast but a compressive dressing and a postoperative stiff-soled shoe to allow early mobilization.
If this technique is performed as an isolated procedure we do not use a cast but a compressive dressing and a postoperative stiff-soled shoe to allow early mobilization.
![]() Patients are kept non–weight-bearing for 2 weeks and then encouraged to bear weight by heel walking for 2 weeks.
Patients are kept non–weight-bearing for 2 weeks and then encouraged to bear weight by heel walking for 2 weeks.
![]() Four weeks after surgery a radiograph is taken (FIG 2). If there is evidence of consolidation, forefoot weight bearing is commenced in the postoperative shoe. Progression to full forefoot loading, assisted by crutches, follows over the next 4 weeks.
Four weeks after surgery a radiograph is taken (FIG 2). If there is evidence of consolidation, forefoot weight bearing is commenced in the postoperative shoe. Progression to full forefoot loading, assisted by crutches, follows over the next 4 weeks.
![]() Radiographs taken 8 weeks after surgery usually confirm consolidation. At this stage flat shoes with cushioned, shockabsorbing soles are worn.
Radiographs taken 8 weeks after surgery usually confirm consolidation. At this stage flat shoes with cushioned, shockabsorbing soles are worn.
OUTCOMES
![]() Union rates for arthrodesis are quoted in the literature ranging from 80% upward. Using this technique, we have achieved 100% union. The average time for union to be visible radiologically is 6 weeks. All patients experienced significant increases in their outcome scores.3
Union rates for arthrodesis are quoted in the literature ranging from 80% upward. Using this technique, we have achieved 100% union. The average time for union to be visible radiologically is 6 weeks. All patients experienced significant increases in their outcome scores.3

FIG 2 • Radiograph taken 4 weeks after surgery.
COMPLICATIONS
![]() Potential complications of first MTP joint arthrodesis include malunion, infection, delayed union, interphalangeal joint stiffness, extensor hallucis longus tenodesis (secondary to scarring), dorsal cutaneous nerve damage, and hardware problems.
Potential complications of first MTP joint arthrodesis include malunion, infection, delayed union, interphalangeal joint stiffness, extensor hallucis longus tenodesis (secondary to scarring), dorsal cutaneous nerve damage, and hardware problems.
![]() The incision described in this technique minimizes the risk to the extensor hallucis longus and dorsal cutaneous nerve while facilitating maximal plantarflexion to allow reaming.
The incision described in this technique minimizes the risk to the extensor hallucis longus and dorsal cutaneous nerve while facilitating maximal plantarflexion to allow reaming.
![]() The ball-and-socket bone-end preparation minimizes shortening and provides a large congruent cancellous area of contact, enabling easy positioning of the hallux and reducing consolidation time. Temporary Kirschner wire fixation facilitates correct alignment.
The ball-and-socket bone-end preparation minimizes shortening and provides a large congruent cancellous area of contact, enabling easy positioning of the hallux and reducing consolidation time. Temporary Kirschner wire fixation facilitates correct alignment.
![]() Use of the compression screw and dorsal plate ensures maximum stability.
Use of the compression screw and dorsal plate ensures maximum stability.
![]() The low-profile precontoured titanium plate has inbuilt dorsiflexion and hallux valgus angles and is contoured to the specific shapes of the proximal phalanx and the first metatarsal. It acts as a neutralization plate and facilitates correct positioning. The differing screw axes increase pullout strength.
The low-profile precontoured titanium plate has inbuilt dorsiflexion and hallux valgus angles and is contoured to the specific shapes of the proximal phalanx and the first metatarsal. It acts as a neutralization plate and facilitates correct positioning. The differing screw axes increase pullout strength.
![]() These mechanical factors significantly reduce the risk of delayed union and nonunion.
These mechanical factors significantly reduce the risk of delayed union and nonunion.
REFERENCES
· Coughlin M, Shurnas P. Hallux rigidus: grading and long-term results of operative treatment. J Bone Joint Surg Am 2003;85A:2072–2088.
· Politi J, Hayes J, Njus G, et al. First metatarsal-phalangeal joint arthrodesis; a biomechanical assessment of stability. Foot Ankle Int 2003;24:332–337.
· Stephens MM, Flavin R. Arthrodesis of the first metatarsophalangeal joint using a dorsal titanium contoured plate. Foot Ankle Int 2004;25:783–787.