Francis C. Nichols
![]() INDICATIONS/CONTRAINDICATIONS
INDICATIONS/CONTRAINDICATIONS
Indications
Aspergillus encompasses over 350 known species including Aspergillus fumigatus, Aspergillus flavus, Aspergillus niger, and Aspergillus terreus which are the most common pathogenic species. With increasing frequency, Aspergillusspecies are being recognized as an important cause of life-threatening infections in immunocompromised patients. The ever expanding population of immunocompromised patients includes patients with prolonged neutropenia, advanced human immunodeficiency virus (HIV) infection, and inherited immunodeficiency; patients having undergone hematopoietic stem cell transplantation and lung transplantation. Aspergillosis is now the third most common systemic fungal infection requiring hospitalization in the United States. Pulmonary aspergillosis was classified into allergic, invasive, and saprophytic infections in 1952 by Hinson et al. Clinical manifestations of pulmonary Aspergillus infection include:
1. A localized form, aspergilloma, which is an opportunistic infection most commonly found in individuals with pre-existing lung disease
2. Allergic bronchopulmonary aspergillosis, which is secondary to a complex immunologic response to exposure to noninvasive Aspergillus species
3. Disseminated aspergillosis, which occurs in immunosuppressed individuals
Pulmonary aspergilloma is the most common form of Aspergillus infection. Aspergilloma occurs when a pre-existing pulmonary cavity is colonized by the fungus producing a complex mass of septate hyphae, blood elements, and debris commonly referred to as a mycetoma or fungus ball. While the true incidence of aspergilloma is unknown, various cavitary lung diseases including bullous emphysema, fibrotic lung disease, histoplasmosis, sarcoidosis, and tuberculosis can be a predisposing factor in their formation.
It is generally believed that systemic antifungal agents are ineffective for aspergilloma. Surgical intervention for aspergillosis occurs in two distinct circumstances: Lung biopsy for the diagnosis of invasive aspergillosis in an immunocompromised patient and resection for complications of aspergilloma. There are no randomized controlled trials addressing the best treatment of aspergilloma. Literature focusing on aspergilloma treatment consists primarily of isolated case reports and retrospective case series. The major surgical indication for patients with aspergilloma is severe or recurring hemoptysis. Thirty percent of patients with even minor hemoptysis can progress to massive life-threatening hemoptysis with an associated 25% mortality. Daly et al. from our group in 1986 reported on the results of surgical treatment for pulmonary aspergilloma. Underlying chronic lung disease or immunologic risk factors were present in 92% of patients. The most common indication for operation was an indeterminate mass, hemoptysis, or chronic cough. In Daly’s series, all aspergillomas were classified as either simple or complex. Simple aspergillomas had thin-walled cysts with little surrounding lung disease. Complex aspergillomas had thick-walled cavities usually greater than 3 mm, with substantial surrounding lung disease and/or associated infiltrates. While in our series, the most common procedures performed were lobectomy (45%), pneumonectomy (17%), wedge excision (15%), and segmentectomy (11%); cavernostomy with muscle transposition was performed in six patients (11%). Postoperative complications were more common in patients with complex aspergilloma than among those with simple. It was noted that to reduce operative complications in some of our patients with complex aspergillomas, six were treated with cavernostomy and obliteration of the cavity with intrathoracic transposition of extrathoracic skeletal muscle. Others too have advocated cavernostomy with or without muscle flap transposition in patients with limited respiratory function or poor general condition as a safe method to effectively treat aspergilloma and prevent recurrence of hemoptysis.
Contraindications
The goal of aspergilloma surgery is limited resection resulting in removal of all diseased tissue sparing more normal lung parenchyma. For simple aspergilloma in patients with reasonable performance status and adequate pulmonary reserve, resection (e.g., wedge, segmental, lobectomy, rarely pneumonectomy) of the aspergilloma is the procedure of choice. Cavernostomy is an option for the management of peripheral complex aspergilloma in high-risk patients. The principal contraindications to cavernostomy are technical and relate to the location of the aspergilloma or the amount of afflicted lung. For example, very medially situated aspergillomas or those central within the lung far removed from the visceral pleural surface are not good candidates for cavernostomy.
![]() PREOPERATIVE PLANNING
PREOPERATIVE PLANNING
The natural history of aspergilloma may be highly variable; therefore, the initial management of a patient depends on the clinical presentation. While surgical resection is the preferred curative treatment for aspergilloma, cavernostomy with muscle transposition may be the best option for the most challenging higher-risk patients. Among these patients are those with severe hemoptysis and severe lung destruction with a high risk of morbidity. Cavernostomy may also be the most reasonable alternative in patients with more isolated peripheral aspergilloma but poor performance status and limited pulmonary reserve. Depending on the patient’s presentation, appropriate resuscitation is undertaken and respiratory support provided as needed. When a patient presents with mild non–life-threatening hemoptysis or cough, initial management can be conservative including humidified oxygen, cough suppression, and postural drainage. These patients require close follow-up. Flexible bronchoscopy should be performed to rule out more serious causes of airway bleeding or cough. In cases of severe hemoptysis, bronchoscopy should quickly be performed to identify the bleeding site. Intrabronchial instillation of iced saline with or without epinephrine may temporarily stop the bleeding. If the bleeding is massive, balloon occlusion of the bleeding airway may be helpful. Alternatively, double-lumen endotracheal tube intubation may be necessary for isolation of the bleeding lung and to protect the contralateral lung from aspiration of blood. Bronchial artery embolization may be helpful in initially stopping most bleeding. We often consider embolization a temporizing measure. Bleeding can recur in greater than 50% of cases due to the existence of an extensive array of collateral vessels. Embolization, however, may obviate the need for emergent surgical intervention in this high-risk population.
Mandatory prerequisites to successful cavernostomy command adequate lung debridement, closure of all bronchial openings, avoidance of contamination of the surrounding pleural space, and the ability to dependably transpose extraskeletal muscle intrathoracically. It is our strong belief that these essential items are most safely accomplished by the collaborative efforts of a thoracic and plastic surgeon. Intrathoracic muscle transposition requires the consideration of several factors: Location and size of the exposed cavity, general condition of the patient, condition of the transposed muscle (e.g., previous radiation or surgery), patient’s lifestyle, and type of work. The serratus anterior, latissimus dorsi, and pectoralis major muscles are all ideally suited for intrathoracic transposition. These muscles all have one major dominant vascular pedicle high in the thoracic inlet and of sufficient length to reach most intrathoracic locations. Furthermore, these muscles are of sufficient size to obliterate most pleural spaces. While not common, pectoralis minor and trapezius have also been utilized. Knowing which chest wall muscles are available at the time of cavernostomy and appropriately protecting these muscles during cavernostomy is important.
Nutritional status is important in this group of patients who are often debilitated and malnourished from chronic infection. If necessary, nutritional supplementation including liberal use of enteral feedings should be considered in all of these patients.
![]() SURGERY
SURGERY
There are four basic principles for cavernostomy: (1) adequate lung debridement, (2) avoidance of contamination of the remaining pleural cavity, (3) closure of all bronchial openings, and (4) obliteration of the residual pleural space. Our most common approach is two-staged. The first stage consists of limited chest wall resection, cavernostomy and removal of the fungus ball, suture closure of any bronchial openings followed by a series of wound pack changes. Only after successful completion of the first stage is the second stage undertaken, which specifically includes transposition of a muscle flap to obliterate the exposed cavity, an additional series of pack changes, and eventual definitive closure of the chest wall. Gebitekin et al. have reported on a small series of patients with complex aspergilloma successfully treated with single-stage cavernostomy and myoplasty.
All procedures begin with a team briefing. Surgeons, anesthesiologists, and operating room personnel are in attendance. Details of the airway management individualized for each specific patient are a major focus of the briefing. Patient identification, site marking, procedure verification, and final anesthetic evaluation are completed. Appropriate intravenous access is established. Epidural catheters are not utilized because of the risk of contamination. Instead, postoperative pain management most commonly is via a patient-controlled analgesia (PCA) pump. At least for the initial procedure isolation of the lungs is achieved by using a double-lumen endotracheal tube. Following intubation, a urinary catheter and lower extremity sequential compression devices are placed. Subcutaneous injection of 5,000 units of unfractionated heparin is administered to reduce the risk of deep venous thrombosis (DVT) and pulmonary embolism. All procedures are done in an open fashion, in a lateral decubitus position with the affected lung’s side up.
First Stage
Rib Resection, Cavernostomy, Closure of Bronchial Fistulae, Wound Packing
![]() The patient is positioned keeping in mind both the location of the aspergilloma and the extraskeletal muscle that will be transposed to eventually obliterate the cavernostomy (Figs. 9.1 and 9.2A,B).
The patient is positioned keeping in mind both the location of the aspergilloma and the extraskeletal muscle that will be transposed to eventually obliterate the cavernostomy (Figs. 9.1 and 9.2A,B).

Figure 9.1 Chest CT scan of peripheral right upper lobe complex aspergilloma in patient with diffuse emphysematous lung disease.

Figure 9.2 A,B: The three most common extrathoracic muscles transposed intrathoracically are the latissimus dorsi, serratus anterior, and pectoralis major muscles. All are ideally suited for intrathoracic transposition. A: The latissimus dorsi and serratus anterior muscles are transposed based on arterial branches arising from the common thoracodorsal pedicle. These muscles can be used separately or combined on their common vascular pedicle if greater soft tissue volume is necessary to obliterate the cavity. B: The pectoralis major muscle can be transposed laterally based on the thoracoacromial artery or more medially when based on perforators from the ipsilateral internal mammary artery.
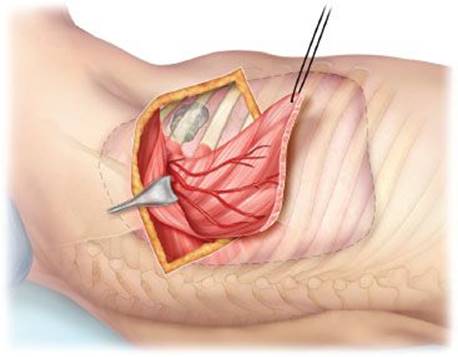
Figure 9.3 The latissimus dorsi muscle has been divided. The serratus anterior muscle injected with 100 units of botulinum toxin and then mobilized with the muscle’s blood supply based on the crossing branch of the thoracodorsal artery. Note the cavity with aspergilloma immediately beneath the second and third ribs.
![]() The ipsilateral hemithorax is prepared and draped.
The ipsilateral hemithorax is prepared and draped.
![]() Most commonly a transverse incision is utilized. Hundred units of botulinum toxin is reconstituted with 20 cc of normal saline. In this case the serratus anterior muscle will be transposed. The latissimus dorsi muscle has been divided low in the incision. The serratus anterior muscle is injected with 20 cc of botulinum toxin, which temporarily paralyzes the muscle keeping it flaccid for several weeks. The serratus anterior is mobilized (Fig. 9.3).
Most commonly a transverse incision is utilized. Hundred units of botulinum toxin is reconstituted with 20 cc of normal saline. In this case the serratus anterior muscle will be transposed. The latissimus dorsi muscle has been divided low in the incision. The serratus anterior muscle is injected with 20 cc of botulinum toxin, which temporarily paralyzes the muscle keeping it flaccid for several weeks. The serratus anterior is mobilized (Fig. 9.3).
![]() The rib over the aspergilloma resected. The cavernostomy performed and the fungus ball and other debris removed. Appropriate specimens are sent for microbiologic and histopathologic testing. The length of rib resected must be sufficient for debridement of the aspergilloma cavity, adequate visualization of the cavity, and wide enough for eventual muscle transposition. The visceral and parietal pleura around the perimeter of the cavernostomy site are often tightly fused. Care is taken to avoid separating them thus preventing contamination of the adjacent pleural cavity. To further aid in visualization and debridement, an additional segment of rib either immediately above or below can be removed; nevertheless, avoidance of contamination of the adjacent pleural cavity is essential (Fig. 9.4).
The rib over the aspergilloma resected. The cavernostomy performed and the fungus ball and other debris removed. Appropriate specimens are sent for microbiologic and histopathologic testing. The length of rib resected must be sufficient for debridement of the aspergilloma cavity, adequate visualization of the cavity, and wide enough for eventual muscle transposition. The visceral and parietal pleura around the perimeter of the cavernostomy site are often tightly fused. Care is taken to avoid separating them thus preventing contamination of the adjacent pleural cavity. To further aid in visualization and debridement, an additional segment of rib either immediately above or below can be removed; nevertheless, avoidance of contamination of the adjacent pleural cavity is essential (Fig. 9.4).
![]() Any visible vessels are oversewn with 4-0 nonabsorbable monofilament suture. Due to the often fragile tissue surrounding the vessels, small pieces of extraskeletal muscle or biologic mesh may be used as pledgets to buttress the vessel closures.
Any visible vessels are oversewn with 4-0 nonabsorbable monofilament suture. Due to the often fragile tissue surrounding the vessels, small pieces of extraskeletal muscle or biologic mesh may be used as pledgets to buttress the vessel closures.
![]() Small bronchial fistulas are looked for by filling the cavernostomy site with saline, applying positive pressure ventilation, and observing for escape of air bubbles from the surrounding lung parenchyma. This testing requires appropriate adjustment of the double-lumen tube.
Small bronchial fistulas are looked for by filling the cavernostomy site with saline, applying positive pressure ventilation, and observing for escape of air bubbles from the surrounding lung parenchyma. This testing requires appropriate adjustment of the double-lumen tube.
![]() All bronchial fistulas are closed using interrupted 3-0 or 4-0 nonabsorbable monofilament sutures. Due to the often fragile tissue surrounding the fistula, small pieces of extraskeletal muscle or biologic mesh may be used as pledgets to buttress the fistula closures (Fig. 9.4).
All bronchial fistulas are closed using interrupted 3-0 or 4-0 nonabsorbable monofilament sutures. Due to the often fragile tissue surrounding the fistula, small pieces of extraskeletal muscle or biologic mesh may be used as pledgets to buttress the fistula closures (Fig. 9.4).

Figure 9.4 Portions of the second and third ribs have been resected and the aspergilloma cavity immediately beneath those ribs opened. The fungus ball and debris removed and the cavity sharply debrided. Several small bronchial openings are seen, which need to be closed with 4-0 nonabsorbable monofilament suture. The cavity is then gently pulse irrigated with normal saline and then irrigated with amphotericin B. If a two-stage approach is being utilized, the wound is packed with DABS and amphotericin B–dampened gauze. If a single-stage cavernostomy and myoplasty is done, the serratus muscle is placed into the cavity at this time obliterating the space.
![]() The cavernostomy site is gently pulsatile irrigated with normal saline followed by irrigation with amphotericin B. It is important that all bronchial fistulas are closed before irrigating with amphotericin B, which is a sclerosant. After assuring hemostasis, the cavernostomy cavity is then packed with gauze rolls damply moistened with debridement antibiotic solution (DABS) (20 mg gentamicin and 500,000 units of polymixin B per liter of 0.9% sodium chloride solution) and amphotericin B. The mobilized serratus anterior muscle is placed back into its anatomic position and loosely covered with additional antibiotic-soaked gauze.
The cavernostomy site is gently pulsatile irrigated with normal saline followed by irrigation with amphotericin B. It is important that all bronchial fistulas are closed before irrigating with amphotericin B, which is a sclerosant. After assuring hemostasis, the cavernostomy cavity is then packed with gauze rolls damply moistened with debridement antibiotic solution (DABS) (20 mg gentamicin and 500,000 units of polymixin B per liter of 0.9% sodium chloride solution) and amphotericin B. The mobilized serratus anterior muscle is placed back into its anatomic position and loosely covered with additional antibiotic-soaked gauze.
![]() The patient is returned to the operating room in 48 hours. The cavernostomy cavity again assessed for open bronchial fistulas, which if found are further repaired, sharply debrided, and hand-held pulse irrigated. The site is again assessed for open bronchial fistulas, which if found are repaired. The cavernostomy site is oftentimes clean enough for muscle transposition at this point. If the site is not adequately clean, it is again packed with gauze rolls lightly saturated with DABS and amphotericin B. The ultimate goal for this first stage is a clean cavernostomy site, with closed bronchial fistulas, and granulation tissue beginning to form.
The patient is returned to the operating room in 48 hours. The cavernostomy cavity again assessed for open bronchial fistulas, which if found are further repaired, sharply debrided, and hand-held pulse irrigated. The site is again assessed for open bronchial fistulas, which if found are repaired. The cavernostomy site is oftentimes clean enough for muscle transposition at this point. If the site is not adequately clean, it is again packed with gauze rolls lightly saturated with DABS and amphotericin B. The ultimate goal for this first stage is a clean cavernostomy site, with closed bronchial fistulas, and granulation tissue beginning to form.
Second Stage
Obliteration of the Cavernostomy and Closure of the Chest Wound
![]() Once the cavernostomy site appears clean enough, the previously mobilized muscle flap is placed into the cavernostomy cavity effectively obliterating that space. To prevent displacement, the muscle flap may be secured to the surrounding ribs and soft tissue with interrupted 3-0 nonabsorbable monofilament (Fig. 9.5).
Once the cavernostomy site appears clean enough, the previously mobilized muscle flap is placed into the cavernostomy cavity effectively obliterating that space. To prevent displacement, the muscle flap may be secured to the surrounding ribs and soft tissue with interrupted 3-0 nonabsorbable monofilament (Fig. 9.5).
![]() The patient then undergoes over a period of 1 to 1.5 weeks a series of sharp wound debridements, hand-held pulsatile irrigations, and dressing changes with gauze rolls lightly saturated in DABS and amphotericin B.
The patient then undergoes over a period of 1 to 1.5 weeks a series of sharp wound debridements, hand-held pulsatile irrigations, and dressing changes with gauze rolls lightly saturated in DABS and amphotericin B.
![]() The debridements and dressing changes take place in the operating room every 48 hours until the transposed muscle is sufficiently adherent after which the pack changes can often take place in the patient’s hospital room utilizing if necessary monitored conscious sedation.
The debridements and dressing changes take place in the operating room every 48 hours until the transposed muscle is sufficiently adherent after which the pack changes can often take place in the patient’s hospital room utilizing if necessary monitored conscious sedation.
![]() The wound is ready for definitive closure when there is no evidence of bronchial air leakage, the muscle flap is adherent and growing into place, and the wound is clean and covered with healthy granulation tissue. Final wound tissue cultures are not used to determine the timing of wound closure, but may be obtained to guide postclosure systemic antibiotic therapy.
The wound is ready for definitive closure when there is no evidence of bronchial air leakage, the muscle flap is adherent and growing into place, and the wound is clean and covered with healthy granulation tissue. Final wound tissue cultures are not used to determine the timing of wound closure, but may be obtained to guide postclosure systemic antibiotic therapy.
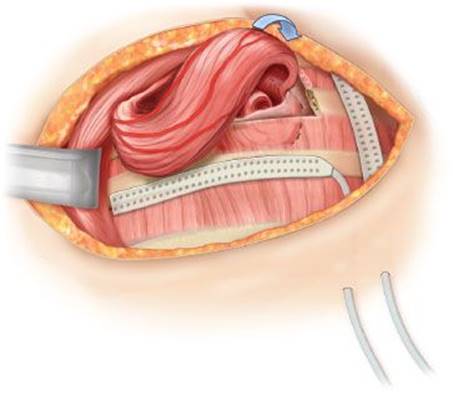
Figure 9.5 The serratus anterior has been placed into the cavity effectively obliterating the space. If a two-stage approach is being utilized the wound is packed with DABS and amphotericin B–dampened gauze. If a single-stage cavernostomy and myoplasty is being done, a large drain placed and the skin closed.

Figure 9.6 The wound is closed over a large drain utilizing interrupted 3-0 or 4-0 nonabsorbable monofilament vertical mattress sutures evenly spaced along the wound.
![]() The wound is closed over a large drain utilizing interrupted 3-0 or 4-0 nonabsorbable monofilament vertical mattress sutures evenly spaced along the wound (Fig. 9.6).
The wound is closed over a large drain utilizing interrupted 3-0 or 4-0 nonabsorbable monofilament vertical mattress sutures evenly spaced along the wound (Fig. 9.6).
![]() The wound is then covered with large gauze pads held loosely in place with paper tape, and finally with a long wide elastic wrap, which keeps the dressings atraumatically in place.
The wound is then covered with large gauze pads held loosely in place with paper tape, and finally with a long wide elastic wrap, which keeps the dressings atraumatically in place.
Single-Stage Cavernostomy and Myoplasty
Cavernostomy, Muscle Transposition, and Wound Closure in One Procedure
![]() The patient is positioned keeping in mind both the location of the aspergilloma and the extraskeletal muscle, that will be transposed to eventually obliterate the cavernostomy (Figs. 9.1 and 9.2A,B).
The patient is positioned keeping in mind both the location of the aspergilloma and the extraskeletal muscle, that will be transposed to eventually obliterate the cavernostomy (Figs. 9.1 and 9.2A,B).
![]() The ipsilateral hemithorax is prepared and draped.
The ipsilateral hemithorax is prepared and draped.
![]() Most commonly a transverse incision is utilized. 100 units of botulinum toxin is reconstituted with 20 cc of normal saline. In this case the serratus anterior muscle will be transposed. The latissimus dorsi muscle has been divided low in the incision. The serratus anterior muscle is injected with 20 cc of botulinum toxin, which temporarily paralyzes the muscle keeping it flaccid for several weeks. The serratus anterior is mobilized (Fig. 9.3).
Most commonly a transverse incision is utilized. 100 units of botulinum toxin is reconstituted with 20 cc of normal saline. In this case the serratus anterior muscle will be transposed. The latissimus dorsi muscle has been divided low in the incision. The serratus anterior muscle is injected with 20 cc of botulinum toxin, which temporarily paralyzes the muscle keeping it flaccid for several weeks. The serratus anterior is mobilized (Fig. 9.3).
![]() The rib over the aspergilloma is resected. The cavernostomy is performed and the fungus ball and other debris removed. Appropriate specimens are sent for microbiologic and histopathologic testing. The length of rib resected must be sufficient for debridement of the aspergilloma cavity, adequate visualization of the cavity, and wide enough for eventual muscle transposition. The visceral and parietal pleura around the perimeter of the cavernostomy site are often tightly fused. Care is taken to avoid separating them thus preventing contamination of the adjacent pleural cavity. To further aid in visualization and debridement, an additional segment of rib either immediately above or below can be removed; however, avoidance of contamination of the adjacent pleural cavity is essential (Fig. 9.4).
The rib over the aspergilloma is resected. The cavernostomy is performed and the fungus ball and other debris removed. Appropriate specimens are sent for microbiologic and histopathologic testing. The length of rib resected must be sufficient for debridement of the aspergilloma cavity, adequate visualization of the cavity, and wide enough for eventual muscle transposition. The visceral and parietal pleura around the perimeter of the cavernostomy site are often tightly fused. Care is taken to avoid separating them thus preventing contamination of the adjacent pleural cavity. To further aid in visualization and debridement, an additional segment of rib either immediately above or below can be removed; however, avoidance of contamination of the adjacent pleural cavity is essential (Fig. 9.4).
![]() Any visible vessels are oversewn with 4-0 nonabsorbable monofilament suture. Due to the often fragile tissue surrounding the vessels, small pieces of extraskeletal muscle or biologic mesh may be used as pledgets to buttress the vessel closures.
Any visible vessels are oversewn with 4-0 nonabsorbable monofilament suture. Due to the often fragile tissue surrounding the vessels, small pieces of extraskeletal muscle or biologic mesh may be used as pledgets to buttress the vessel closures.
![]() Small bronchial fistulas are looked for by filling the cavernostomy site with saline, applying positive pressure ventilation, and observing for escape of air bubbles from the surrounding lung parenchyma. This testing requires appropriate adjustment of the double-lumen tube.
Small bronchial fistulas are looked for by filling the cavernostomy site with saline, applying positive pressure ventilation, and observing for escape of air bubbles from the surrounding lung parenchyma. This testing requires appropriate adjustment of the double-lumen tube.
![]() All bronchial fistulas are closed using interrupted 3-0 or 4-0 nonabsorbable monofilament sutures. Due to the often fragile tissue surrounding the fistula, small pieces of extraskeletal muscle or biologic mesh may be used as pledgets to buttress the fistula closures (Fig. 9.4).
All bronchial fistulas are closed using interrupted 3-0 or 4-0 nonabsorbable monofilament sutures. Due to the often fragile tissue surrounding the fistula, small pieces of extraskeletal muscle or biologic mesh may be used as pledgets to buttress the fistula closures (Fig. 9.4).
![]() The cavernostomy site is gently pulsatile irrigated with at least 3 L of normal saline followed by irrigation with amphotericin B. It is important that all bronchial fistulas are closed before irrigating with amphotericin B, which is a sclerosant.
The cavernostomy site is gently pulsatile irrigated with at least 3 L of normal saline followed by irrigation with amphotericin B. It is important that all bronchial fistulas are closed before irrigating with amphotericin B, which is a sclerosant.
![]() The previously mobilized muscle flap is placed into the cavernostomy cavity effectively obliterating that space. To prevent displacement, the muscle flap may be secured to the surrounding ribs and soft tissue with interrupted 3-0 nonabsorbable monofilament (Fig. 9.5).
The previously mobilized muscle flap is placed into the cavernostomy cavity effectively obliterating that space. To prevent displacement, the muscle flap may be secured to the surrounding ribs and soft tissue with interrupted 3-0 nonabsorbable monofilament (Fig. 9.5).
![]() The wound is closed over a large drain utilizing interrupted 3-0 or 4-0 nonabsorbable monofilament vertical mattress sutures evenly spaced along the wound (Fig. 9.6).
The wound is closed over a large drain utilizing interrupted 3-0 or 4-0 nonabsorbable monofilament vertical mattress sutures evenly spaced along the wound (Fig. 9.6).
![]() The wound is then covered with large gauze pads held loosely in place with paper tape, and finally with a long wide elastic wrap, which keeps the dressings atraumatically in place.
The wound is then covered with large gauze pads held loosely in place with paper tape, and finally with a long wide elastic wrap, which keeps the dressings atraumatically in place.
![]() POSTOPERATIVE MANAGEMENT
POSTOPERATIVE MANAGEMENT
Cavernostomy patients should go to a unit skilled in the management of patients who have undergone complex general thoracic surgery. Following the initial procedure, the majority of these patients are successfully extubated. Most of our patients following the initial first-stage procedure are successfully managed in our general thoracic surgical progressive care unit (PCU). Only rarely are these patients kept intubated and managed in our general thoracic surgical intensive care unit (ICU). Following subsequent first-stage procedures, depending on patient-specific circumstances, the patients are managed in the PCU or on the general thoracic surgical floor. Standard orders should not be routinely implemented without consideration of specific individualized patient needs; nevertheless, we strive to follow unit specific care pathways. These pathways routinely contain patient monitoring, supplemental oxygen therapy, intravenous fluids, medications including appropriate pain management, wound care, chest physiotherapy by trained respiratory therapists, physical therapy, diet, patient and family education, social services, and when appropriate discharge planning.
Following second-stage definitive chest closure, the care pathway is continued and adjusted accordingly. Wound care most commonly involves daily drain care and adjustments to the elastic wrap. The large gauze pads are changed every 24 to 48 hours and along with the elastic wrap continued for several weeks. The patient may shower starting in 5 days. Removal of the monofilament sutures is individualized to the patient’s wound status and they routinely remain for several weeks. The large drain is removed when there is no evidence of air leakage and drainage is less than 20 cc per day for 2 consecutive days. In general, the 3-0 sutures remain for at least 2 to 3 weeks and the 4-0 sutures are removed after 4 to 5 weeks.
Oral antifungal agents are begun in the perioperative period and commonly continued for 3 to 6 months. Over the past decade there has been a considerable expansion in the number of antifungal medications available for clinical use. Specific antifungal medications and use of other antimicrobial agents may be influenced by intraoperative cultures and consultation with infectious disease specialists for these oftentimes immunocompromised and debilitated patients.
![]() COMPLICATIONS
COMPLICATIONS
Literature focusing on cavernostomy as treatment for aspergilloma consists primarily of isolated case reports and retrospective case series often reported as subsets of more encompassing retrospective reviews on the surgical management of aspergilloma. Specific data related to complications is sparse and one must keep in mind that cavernostomy is reserved for patients with poor overall performance. Nonetheless, it seems that intraoperative complications during cavernostomy are rare. Regnard et al. reported on 17 patients having cavernostomy. Complications included postoperative significant hemorrhage and prolonged ventilation (>48 hours) in one patient (5.8%) each. There were no deaths in the cavernostomy patients. Babatasi et al., in eight cavernostomy patients, reported postoperative hemorrhage and prolonged air leakage in 12% and 50% of patients, respectively. Perioperative mortality occurred in one patient (12.5%). Finally Daly from our institution reported no deaths in six cavernostomy patients. Gebitekin et al. reported on nine patients with complex aspergilloma treated with single-stage cavernostomy and muscle transposition, and found two patients who required re-exploration for massive air leak from occult bronchial fistulas. They reported no perioperative deaths.
![]() RESULTS
RESULTS
Daly et al. from our institution in 1986 reported on 53 patients having surgery for aspergilloma. Twenty-one patients (31%) had simple aspergilloma and thirty-two (47%) complex aspergilloma. Complications occurred in 78% of patients with complex aspergilloma and in 33% with simple aspergilloma (p = 0.002). Operative mortality was 5% (1 death) in patients with simple aspergilloma and 34% (11 deaths) in patients with complex aspergilloma. In an effort to reduce complications in patients with complex aspergilloma, cavernostomy with obliteration of the cavity and intrathoracic extraskeletal muscle transposition was utilized in six patients. There were no deaths in the cavernostomy patients and long-term results were reported as good. Similar results have been reported by others.
Cesar et al. reported on 208 patients with surgically treated aspergilloma over a 32-year period. One hundred and eleven patients had cavernostomy and 97 pulmonary resections. For cavernostomy, the cavity was initially packed with gauze containing no antifungal substance. The cavity was left to spontaneously close and muscle transposition was only performed if the cavity failed to close after 90 days. The number of muscle transpositions was not reported. Ten patients (9%) with cavernostomy ultimately required pulmonary resection because of recurrence. Ten patients (10.3%) with pulmonary resection had a residual space. Infectious complications were more frequent in pulmonary resection patients 25% versus cavernostomy patients 7.2%. Recurrence, however, was only seen in cavernostomy patients 8.1%. Hemorrhagic complications were more common in cavernostomy patients 45% versus pulmonary resection patients 12%, but hemoptysis was far more frequent preoperatively in cavernostomy patients 96% compared with 59% of pulmonary resection patients. Patient progression, which was defined as death and cure were similar between the two groups. Cesar et al. concluded that older patients with severe preoperative respiratory insufficiency and peripheral aspergilloma are best served by cavernostomy and the remaining patients best treated by pulmonary resection.
The results of Gebitekin and colleagues single-stage cavernostomy and myoplasty for complex aspergilloma are intriguing. There were no perioperative deaths and median hospital stay was 9 days (range 6 to 15). Eight patients were alive and well without symptoms or recurrence at mean follow-up of 57.2 months (range: 18 to 83 months). However, this report only included 9 patients over a 7.5-year timeframe. Worrisome is that two patients (22%) required re-exploration for massive air leakage.
![]() CONCLUSIONS
CONCLUSIONS
Cavernostomy with extraskeletal muscle transposition (most commonly latissimus dorsi, pectoralis major, and serratus anterior) is an alternative treatment to pulmonary resection for patients with aspergilloma. Patients whose overall medical condition and pulmonary function are poor with peripheral complex pulmonary aspergilloma may be best treated with cavernostomy and muscle transposition. Morbidity and mortality of this procedure are low and long-term results are good.
Recommended References and Readings
Babatasi G, Massetti M, Chapelier A, et al. Surgical treatment of pulmonary aspergilloma: Current outcome. J Thorac Cardiovasc Surg. 2000;119:906–912.
Cesar JM, Resende JS, Amaral NF, et al. Cavernostomy x resection for pulmonary aspergilloma: A 32-year history. J Cardiothorac Surg. 2011;6:129.
Daly RC, Pairolero PC, Piehler JM, et al. Pulmonary aspergilloma. Results of surgical treatment. J Thorac Cardiovasc Surg. 1986;92:981–988.
Gebitekin C, Sami Bayram A, Akin S. Complex pulmonary aspergilloma treated with single stage cavernostomy and myoplasty. Eur J Cardiothorac Surg. 2005;27:737–740.
Meland NB, Arnold PG, Pairolero PC, et al. Refinements in intrathoracic use of muscle flaps. Clin Plast Surg. 1990;17:697–703.
Regnard JF, Icard P, Nicolosi M, et al. Aspergilloma: A series of 89 surgical cases. Ann Thorac Surg. 2000;69:898–903.
Rergkliang C, Chetpaophan A, Chittithavorn V, et al. Surgical management of pulmonary cavity associated with fungus ball. Asian Cardiovasc Thorac Ann. 2004;12:246–249.
Walsh TJ, Anaissie EJ, Denning DW, et al. Treatment of aspergillosis: Clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis. 2008;46:327–360.