P. Brandon Bookstaver and April D. Miller
LEARNING OBJECTIVES
Upon completion of the chapter, the reader will be able to:
1. Discuss the pathophysiology of CNS infections and the impact on antimicrobial treatment regimens (such as dosing and CNS penetration).
2. Describe the signs, symptoms, and clinical presentation of CNS infections.
3. List the most common pathogens causing CNS infections and identify risk factors for infection with each pathogen.
4. State the goals of therapy for CNS infections.
5. Design appropriate empirical antimicrobial regimens for patients suspected of having CNS infections caused by each of the following pathogens (taking age, vaccine history, and other patient-specific information into account), and analyze the impact of antimicrobial resistance on both empirical and definitive therapy: Neisseria meningitidis meningitis, meningitis, Haemophilus influenzae meningitis, Listeria meningitis, group B Streptococcusmeningitis, gram-negative bacillary meningitis, postneurosurgical infection, CNS shunt infection, herpes simplex encephalitis.
6. Modify empirical antimicrobial regimens based on laboratory data and other diagnostic criteria.
7. Discuss the management of close contacts of patients diagnosed with CNS infections.
8. Identify candidates for vaccines and other prophylactic therapies to prevent CNS infections.
9. Describe the role of adjunctive agents (such as dexamethasone) in the management of CNS infections.
10. Formulate a monitoring plan to assess efficacy and adverse effects of therapy for CNS infections.
KEY CONCEPTS
![]() Meningitis is a neurologic emergency that requires prompt recognition, diagnosis, and management to prevent death and residual neurologic defects. Patients with fever, headache, and neck stiffness should be evaluated for meningitis.
Meningitis is a neurologic emergency that requires prompt recognition, diagnosis, and management to prevent death and residual neurologic defects. Patients with fever, headache, and neck stiffness should be evaluated for meningitis.
![]() Ideally, lumbar puncture (LP) to obtain cerebrospinal fluid (CSF) for direct examination and laboratory analysis, as well as blood cultures and other relevant cultures, should be obtained before initiation of antimicrobial therapy. However, initiation of antimicrobial therapy should not be delayed if a pretreatment LP cannot be performed.
Ideally, lumbar puncture (LP) to obtain cerebrospinal fluid (CSF) for direct examination and laboratory analysis, as well as blood cultures and other relevant cultures, should be obtained before initiation of antimicrobial therapy. However, initiation of antimicrobial therapy should not be delayed if a pretreatment LP cannot be performed.
![]() The treatment goals for CNS infections are to prevent death and residual neurologic deficits, eradicate or control causative microorganisms, ameliorate clinical signs and symptoms, and identify measures (such as vaccination and suppressive therapy) to prevent future infections.
The treatment goals for CNS infections are to prevent death and residual neurologic deficits, eradicate or control causative microorganisms, ameliorate clinical signs and symptoms, and identify measures (such as vaccination and suppressive therapy) to prevent future infections.
![]() Prompt initiation of IV high-dose bactericidal antimicrobial therapy directed at the most likely pathogen(s) is essential due to the high morbidity and mortality associated with CNS infections.
Prompt initiation of IV high-dose bactericidal antimicrobial therapy directed at the most likely pathogen(s) is essential due to the high morbidity and mortality associated with CNS infections.
![]() IV therapy is administered for the full course of therapy for CNS infections to ensure adequate CSF penetration throughout the course of treatment.
IV therapy is administered for the full course of therapy for CNS infections to ensure adequate CSF penetration throughout the course of treatment.
![]() Empirical therapy should be directed at the most likely pathogen(s) for a specific patient, taking into account age, risk factors for infection (including underlying disease and immune dysfunction, vaccine history, and recent exposures), CSF Gram stain results, CSF antibiotic penetration, and local antimicrobial resistance patterns.
Empirical therapy should be directed at the most likely pathogen(s) for a specific patient, taking into account age, risk factors for infection (including underlying disease and immune dysfunction, vaccine history, and recent exposures), CSF Gram stain results, CSF antibiotic penetration, and local antimicrobial resistance patterns.
![]() Empirical antimicrobial therapy should be modified on the basis of laboratory data and clinical response.
Empirical antimicrobial therapy should be modified on the basis of laboratory data and clinical response.
![]() Close contacts of patients with CNS infections should be evaluated for possible antimicrobial prophylaxis.
Close contacts of patients with CNS infections should be evaluated for possible antimicrobial prophylaxis.
![]() Components of a monitoring plan to assess the efficacy and safety of antimicrobial therapy of CNS infections include clinical signs and symptoms and laboratory data (e.g., CSF findings, culture, and sensitivity data).
Components of a monitoring plan to assess the efficacy and safety of antimicrobial therapy of CNS infections include clinical signs and symptoms and laboratory data (e.g., CSF findings, culture, and sensitivity data).
The term CNS infections describes a variety of infections involving the brain and spinal cord and associated tissues, fluids, and membranes, including meningitis, encephalitis, brain abscess, shunt infections, and postoperative infections (see Glossary). ![]() CNS infections, such as meningitis, are considered neurologic emergencies that require prompt recognition, diagnosis, and management to prevent death and residual neurologic deficits. Improperly treated, CNS infections are associated with high rates of morbidity and mortality. Despite advances in care, the overall mortality of bacterial meningitis remains greater than 20%, and at least 10% to 30% of survivors are afflicted with neurologic impairment, including hearing loss, hemiparesis, and learning disabilities.1–3 Antimicrobial therapy and preventive vaccines have revolutionized management and improved outcomes of bacterial meningitis and other CNS infections dramatically.
CNS infections, such as meningitis, are considered neurologic emergencies that require prompt recognition, diagnosis, and management to prevent death and residual neurologic deficits. Improperly treated, CNS infections are associated with high rates of morbidity and mortality. Despite advances in care, the overall mortality of bacterial meningitis remains greater than 20%, and at least 10% to 30% of survivors are afflicted with neurologic impairment, including hearing loss, hemiparesis, and learning disabilities.1–3 Antimicrobial therapy and preventive vaccines have revolutionized management and improved outcomes of bacterial meningitis and other CNS infections dramatically.
EPIDEMIOLOGY AND ETIOLOGY
CNS infections are uncommon, with four to six cases of meningitis reported per 100,000 adults annually.4 However, the severity of these infections demands prompt medical intervention and treatment. CNS infections can be caused by bacteria, fungi, mycobacteria, viruses, and spirochetes.
Bacterial meningitis is the most common cause of CNS infections. Streptococcus pneumoniae (pneumococcus) was the most common pathogen for bacterial meningitis (47%), followed by Neisseria meningitidis (meningococcus, 25%), group B Streptococcus (12%), Listeria monocytogenes (8%), and Haemophilus influenzae (7%).5 Vaccines directed against bacteria causing meningitis and related infections (such as pneumonia and ear infections) have reduced the risk of infections due to S. pneumoniae, N. meningitidis, and H. influenzae type b (HIb) dramatically. Prior to the availability of Hib conjugate vaccines, Hib meningitis or other invasive disease was documented in one in 200 children by the age of 5 years.5 Widespread use of the Hib vaccine has reduced the incidence of invasive Hib disease by 99% and has shifted the age distribution of bacterial meningitis to older age groups (from 15 months in 1986 to 25 years in 1995).1,6 The routine use of the 7-valent conjugate pneumococcal vaccine (PCV7) in children has not only reduced the incidence of invasive pneumococcal disease in children but has also reduced invasive pneumococcal disease in adults 50 years of age and older by 28%.7 Despite introduction of the PCV7, S. pneumoniae remains the most common pathogen for pediatric bacterial meningitis with nearly 50% of cases due to nonvaccine serotypes.8
Encephalitis may result from a number of viral, bacterial, parasitic, and other noninfectious causes. Herpes simplex virus (HSV) is the most common cause of encephalitis in the United States, accounting for 10% of all cases.9The annual incidence of viral encephalitis is estimated to be 3.5 to 7.4 infections per 100,000 persons.9 Other pathogens include common bacterial meningitis causes, Ricksettsia species, enteroviruses, arboviruses, varicella-zoster virus, rotavirus, coronavirus, influenza viruses A and B, West Nile virus, and Epstein-Barr virus may be associated with a meningo-encephalopathic presentation.10Approximately 20,000 hospitalizations each year are secondary to encephalitis accounting for $650 million in health care costs.11 Over the past 10 to 20 years, mortality secondary to encephalitis has remained constant correlating well with the increased number of people living with HIV and AIDS. HIV infection is concurrent in nearly 20% of patients dying from encephalitis.12
Neurosurgical procedures may place patients at risk for meningitis due to bacteria (such as Staphylococcus aureus, coagulase-negative staphylococci, and gram-negative bacilli) acquired at the time of surgery or in the postoperative period. In addition to bacteria, other pathogens may cause meningitis in at-risk patients. Immunocompromised patients, such as solid-organ transplant patients and patients living with HIV infection, are at risk for fungal meningitis with Cryptococcus neoformans and encephalitis secondary to Toxoplasma gondii and JC virus (see Chap. 84). Tuberculosis can spread from pulmonary sites to cause clinical disease in the CNS. Life-threatening viral encephalitis and meningitis can occur in otherwise healthy, young individuals, as well as in patients immunocompromised by age or other factors. Because the treatments for different types of CNS infections are often different, it is important to pay close attention to patients’ risk factors when choosing empirical antimicrobial therapy. Patients at extremes of age, those living in close contact with others, and those with immune defects are most susceptible to meningitis. Risk factors for CNS infections can be classified as follows:
• Environmental—recent exposures (such as close contact with meningitis or respiratory tract infection, contaminated foods), active or passive exposure to cigarette smoke, close living conditions
• Recent infection in the patient—respiratory infection, otitis media, sinusitis, mastoiditis
• Immunosuppression—anatomic or functional asplenia, sickle cell disease, alcoholism, cirrhosis, immunoglobulin or complement deficiency, cancer, HIV/AIDS, uncontrolled diabetes mellitus, debilitated state of health
• Surgery, trauma—neurosurgery, head trauma, CSF shunt, cochlear implant
• Noninfectious causes of meningitis include malignancy, medications (such as sulfonamides, nonsteroidal anti-inflamatory drugs [NSAIDs], IV Immunoglobulin), autoimmune disease (such as lupus), and trauma.8,9
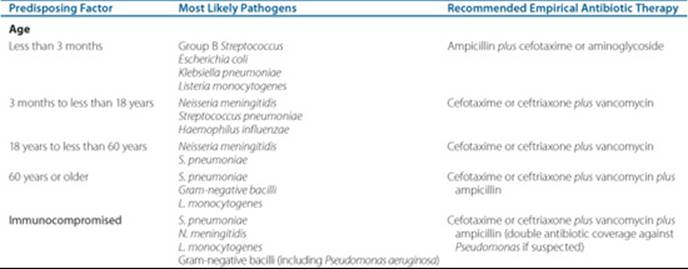
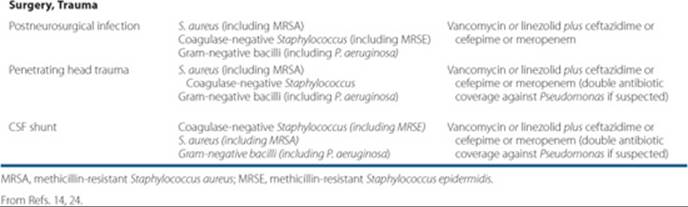
• The most common pathogens causing bacterial meningitis, by age group and other risk factors, are found in Table 70–1.
PATHOPHYSIOLOGY
Meningitis is an inflammation of the membranes of the brain and spinal cord (meninges) and the CSF in contact with these membranes, whereas encephalitis is an inflammation of the brain tissue. CSF flows through the subarachnoid space, insulating and protecting delicate CNS tissue. CSF is produced within the ventricles of the brain and flows downward through the spinal cord, serving as a continuous flushing mechanism for the CNS.
Table 70–1 Most Likely Pathogens and Recommended Empirical Therapy, by Risk Factor, for Bacterial Meningitis
Patient Encounter 1, Part 1
JD is a 17-year-old high school senior who visited her sister at her college dormitory for 1 week prior to her sister leaving for winter break. JD now presents to the emergency department with a 2-day history of headache and fever. Physical findings and laboratory values include temperature of 38.3°C (101°F) and WBC of 14.4 × 103/mm3 (14.4 × 109/L), with 90% polymorphonuclear cells. Examination reveals nuchal rigidity and a petechial truncal rash. JD reports light sensitivity and nausea with vomiting. She has tried nonprescription analgesics and antipyretics with no relief from her headache or fever.
What signs and symptoms consistent with meningitis are present in JD?
What clues to causative pathogen are present in JD?
What empiric antibiotics should be started?
The blood–brain barrier and blood–CSF barrier are made of specialized tissue capillaries that isolate the brain from substances circulating in the bloodstream or colonizing nearby tissues. To initiate a CNS infection, pathogens must gain entry into the CNS by contiguous spread, hematogenous seeding, direct inoculation, or reactivation of latent infection. Contiguous spread occurs when infections in adjacent structures (such as sinus cavities or the middle ear) invade directly through the blood–brain barrier (such as Hib). Hematogenous seeding occurs when a more remote infection causes bacteremia that seeds the CSF (such as pneumococcal pneumonia). Reactivation of latent infection results from dormant viral, fungal, or mycobacterial pathogens in the spine, brain, or nerve tracts. Direct inoculation of bacteria into the CNS is the result of trauma, congenital malformations, or complications of neurosurgery.
Once through the blood–brain barrier, pathogens thrive and replicate due to limited host defenses in the CNS. Figure 70–1 depicts the pathophysiologic changes associated with meningitis. Neurologic tissue damage is the result of the host’s immune reaction to bacterial cellular components (such as lipopolysaccharide, teichoic acid, and peptidoglycan) that triggers cytokine production, particularly tumor necrosis factor alpha (TNF-α) and interleukin 1 (IL-1), as well as other mediators of inflammation.14 Bacteriolysis resulting from antibiotic therapy further contributes to the inflammatory process. Cytokines increase permeability of the blood–brain barrier, allowing influx of neutrophils and other host defense cells that contribute to the development of cerebral edema and increased intracranial pressure characteristic of meningitis.15 The increase in intracranial pressure is responsible for the hallmark clinical signs and symptoms of meningitis: headache, neck stiffness, altered mental status, photophobia, and seizures. Unaltered, these pathophysiologic changes may result in cerebral ischemia and death.
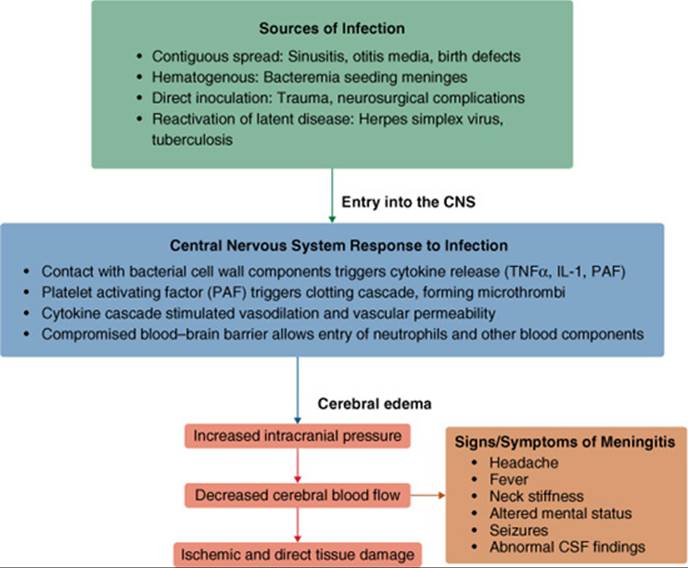
FIGURE 70–1. Pathophysiology of bacterial meningitis.
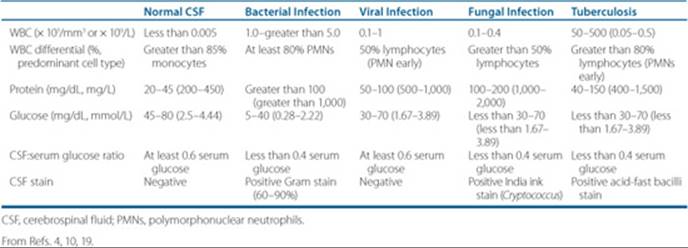
Table 70–2 CNS Response to Infection (CSF Findings)
The CNS response to infection is evident by demonstrable changes in the CSF. ![]() Ideally, LP to obtain CSF for direct examination and laboratory analysis, as well as blood cultures and other relevant cultures, should be obtained before initiation of antimicrobial therapy. However, initiation of antimicrobial therapy should not be delayed if a pretreatment LP cannot be performed.
Ideally, LP to obtain CSF for direct examination and laboratory analysis, as well as blood cultures and other relevant cultures, should be obtained before initiation of antimicrobial therapy. However, initiation of antimicrobial therapy should not be delayed if a pretreatment LP cannot be performed.
Normal CSF has a characteristic composition in terms of protein and glucose content, as well as cell count. Table 70–2 lists CSF findings observed in the absence of infection, as well as in patients with bacterial, viral, fungal, and tuberculous meningitis.
CLINICAL PRESENTATION AND DIAGNOSIS
A high index of suspicion should be maintained for patients at risk for CNS infections. Prompt recognition and diagnosis are essential so that antimicrobial therapy can be initiated as quickly as possible. A medical history (including risk factors for infection and history of possible recent exposures) and physical examination yield important information to help guide the diagnosis and treatment of meningitis. Common signs and symptoms include fever, headache, nuchal rigidity (stiff neck), and photophobia. As common meningeal signs are not typically present in infants, nonspecific signs and symptoms including excessive irritability or crying, vomiting or diarrhea, tachypnea, altered sleep pattern, and poor eating should be noted. Depending on involved pathogens and disease severity, patients may also present with altered mental status, stupor, and seizures.
Clinical Presentation and Diagnosis of CNS Infections
General
• Evaluate patient risk factors and recent exposures
• Evaluate other possible causes: space-occupying lesion (which may or may not be malignant), drug-induced CNS disease, autoimmune disease, and trauma1213
Signs and Symptoms2
• 95% of patients with bacterial meningitis have two of the following: headache, fever, neck stiffness, and altered mental status
• Headache (87%)
• Nuchal rigidity (stiff neck) (83%)
• Fever (77%)
• Nausea (74%)
• Altered mental status (i.e., confusion, lethargy, and obtundation) (69%)
• Focal neurologic defects (including positive Brudzinski’s sign and Kernig’s sign) (33%)
• Seizures
• Malaise, restlessness
• Photophobia
• Skin lesions (diffuse petechial rash observed in 50% of patients with meningococcal meningitis)
• Signs and symptoms in neonates, infants, and young children: nonspecific findings, such as altered feeding and sleep patterns, vomiting, irritability, lethargy, bulging fontanel, seizures, respiratory distress, and petechial/purpuric rash16
• Predictors of an unfavorable outcome: seizures, focal neurologic findings, altered mental status, papilledema, hypotension, septic shock, and pneumococcal meningitis3
Laboratory Tests 4,17,18
• CSF examination via lumbar puncture (LP, spinal tap); contraindicated in patients with cardiorespiratory compromise, increased intracranial pressure and papilledema, focal neurologic signs, seizures, bleeding disorders, abnormal level of consciousness, and possible brain herniation (a CT scan should be performed before LP if there is a question of a CNS mass to avoid potential for brain herniation) (see Table 70–2 for specific CSF findings)
• Elevated opening pressure (may be decreased in neonates, infants, and children)
• Cloudy CSF
• Decreased glucose
• Elevated protein
• Elevated WBC (differential provides clues to offending pathogen)
• Gram stain (adequate for diagnosis in 60-90% of patients with bacterial meningitis)
• Culture and sensitivity (positive in 70-85% without prior antibiotic therapy, positive in less than 20% who have had prior therapy)
• If CSF Gram stain and/or culture is negative, rapid diagnostic tests (such as latex agglutination) may be useful; these tests are positive even if bacteria are dead
• Polymerase chain reaction (PCR; DNA amplification of the most common bacterial meningitis pathogens) may be useful to help exclude bacterial meningitis
• Elevated CSF lactate and C-reactive protein
• Blood cultures (at least two cultures, one “set”; positive in 66%)
• Scraping of skin lesions (such as rash) for direct microscopic examination and culture
• Other cultures should be obtained as clinically indicated (such as sputum)
• WBC with differential
• Fungal meningitis: CSF culture, CSF and serum cryptococcal antigen titers, microscopic examination of CSF specimens
• Tuberculous meningitis: CSF culture, PCR evaluation (preferred), and acid-fast stain
Patient Encounter 1, Part 2
The 17-year-old patient with signs and symptoms of meningitis underwent lumbar puncture. Initial results from CSF studies are WBC 2.2 × 103/mm3 (2.2 × 109/L) with 87% PMNs, protein 320 mg/dL (3,200 mg/L), glucose 10 mg/dL (0.56 mmol/L). Gram stain shows gram-negative diplococci and culture results confirm N. meningitidis infection. While in the ED, her clinical status deteriorated and her BP dropped to 85/60 mm Hg. She was transferred to the ICU for close monitoring.
Given this patient’s clinical deterioration and identification of this pathogen, what complications should she be monitored for?
How can her antibiotic regimen be streamlined at this time?
How long should the antibiotics be continued?
TREATMENT
Goals of Therapy
The introduction of antibiotic therapy and vaccines has reduced dramatically the mortality associated with bacterial meningitis.19 Prior to these advances, bacterial meningitis was almost universally fatal, and those few patients who survived often suffered from debilitating residual neurologic deficits, such as permanent hearing loss. Although significant improvements have been made, the fatality rate of pneumococcal meningitis remains above 20% likely due to its occurrence in debilitated patient populations.
![]() The treatment goals for CNS infections are to prevent death and residual neurologic deficits, eradicate or control causative micro-organisms, ameliorate clinical signs and symptoms, and identify measures to prevent future infections (such as vaccination and suppressive therapy). These goals should be accomplished with minimal adverse drug reactions and interactions. Surgical debridement should be employed, if appropriate (as in postneurosurgical infections and brain abscess). Supportive care, consisting of hydration, electrolyte replacement, antipyretics, antiemetics, analgesics, antiepileptic drugs, and wound care (for surgical wounds), is an important adjunct to antimicrobial therapy, particularly early in the treatment course.
The treatment goals for CNS infections are to prevent death and residual neurologic deficits, eradicate or control causative micro-organisms, ameliorate clinical signs and symptoms, and identify measures to prevent future infections (such as vaccination and suppressive therapy). These goals should be accomplished with minimal adverse drug reactions and interactions. Surgical debridement should be employed, if appropriate (as in postneurosurgical infections and brain abscess). Supportive care, consisting of hydration, electrolyte replacement, antipyretics, antiemetics, analgesics, antiepileptic drugs, and wound care (for surgical wounds), is an important adjunct to antimicrobial therapy, particularly early in the treatment course.
Patient Encounter 1, Part 3
The parents and classmates at the high school of the 17-year-old patient with N. meningitidis call the hospital and are concerned about getting sick. They wonder about medications and vaccinations to prevent the disease.
Who should receive antimicrobial prophylaxis for N. meningitidis?
What antimicrobial regimens are effective for prophylaxis?
Who should receive vaccination against meningococcal disease?
Treatment Principles
![]() Prompt initiation of IV high-dose cidal antimicrobial therapy directed at the most likely pathogen(s) is essential due to the high morbidity and mortality associated with CNS infections. Although there are no prospective studies that relate timing of antibiotic administration to clinical outcome in bacterial meningitis, a longer duration of symptoms and more advanced disease before treatment initiation increase the risk of a poor outcome.3,17,20 Initiation of antibiotic therapy as soon as possible after bacterial meningitis is suspected or proven (even before hospitalization) reduces mortality and neurologic sequelae, as long as antibiotics were started before patients deteriorate to a score of 10 on the Glasgow Coma Scale.21,22 Rapid sterilization of CSF is important; delayed CSF sterilization after approximately 24 hours of antibiotic therapy increases the risk of neurologic sequelae, including moderate to profound hearing loss.23,24
Prompt initiation of IV high-dose cidal antimicrobial therapy directed at the most likely pathogen(s) is essential due to the high morbidity and mortality associated with CNS infections. Although there are no prospective studies that relate timing of antibiotic administration to clinical outcome in bacterial meningitis, a longer duration of symptoms and more advanced disease before treatment initiation increase the risk of a poor outcome.3,17,20 Initiation of antibiotic therapy as soon as possible after bacterial meningitis is suspected or proven (even before hospitalization) reduces mortality and neurologic sequelae, as long as antibiotics were started before patients deteriorate to a score of 10 on the Glasgow Coma Scale.21,22 Rapid sterilization of CSF is important; delayed CSF sterilization after approximately 24 hours of antibiotic therapy increases the risk of neurologic sequelae, including moderate to profound hearing loss.23,24
Meningitis occurs in a tissue with limited host defenses. Bacterial replication occurs rapidly in the absence of complement and specific antibodies directed toward common bacterial pathogens.25 High-dose parenteral bactericidal antibiotic therapy is required to treat meningitis effectively. Data from animal studies and patients demonstrate better outcomes when bactericidal antibiotic therapy (versus bacteriostatic therapy) is used to sterilize the CSF.26However, successful treatment of meningitis has been reported with bacteriostatic agents. High doses of parenteral therapy are required to achieve CSF antibiotic concentrations adequate to rapidly sterilize the CSF and reduce the risk of complications. The presence of infection in the CSF reduces the activity of some classes of antibiotics. For example, the decreased pH of CSF associated with meningitis significantly reduces the activity of aminoglycoside antibiotics.27
Antimicrobial pharmacokinetics and pharmacodynamics must be considered when designing treatment regimens for CNS infections. Ability of antibiotics to reach and achieve effective concentrations at the infection site is the key to treatment success. In experimental models of meningitis, maximum bactericidal activity is achieved when CSF concentrations exceed the minimum bactericidal concentration (MBC) of the infecting pathogen by 10- to 30-fold.16 In general, low-molecular-weight lipophilic antibiotics that are un-ionized at physiologic pH and not highly protein bound penetrate best into CSF and other body tissues and fluids.25,27 In addition to drug characteristics, integrity of the blood–brain barrier determines antibiotic penetration into CSF. The CSF penetration of most, but not all, antibiotics is enhanced by the presence of infection and inflammation. Sulfonamides, trimethoprim, chloramphenicol, rifampin, and most antitubercular drugs achieve therapeutic CSF levels even without meningeal inflammation.10 Most β-lactams and related antibiotics (i.e., carbapenems and monobactams), vancomycin, quinolones, acyclovir, linezolid, daptomycin, and colistin achieve therapeutic CSF levels in the presence of meningeal inflammation.10 Aminoglycosides, first-generation cephalosporins, second-generation cephalosporins (except cefuroxime), clindamycin, and amphotericin do not achieve therapeutic CSF levels, even with inflammation, but clindamycin does achieve therapeutic brain tissue levels.10
An adequate duration of therapy is required to treat meningitis successfully (Table 70–3). ![]() Parenteral (IV) therapy is administered for the full course of therapy for CNS infections to ensure adequate CSF penetration throughout the course of treatment. Antibiotic treatment (and dexamethasone, if used as a treatment adjunct) reduces the inflammation associated with meningitis, which, in turn, reduces the penetration of some antibiotics into the CSF. To ensure adequate antibiotic concentrations throughout the treatment course, parenteral administration is continued for the full treatment course. Carefully selected patients who have close medical monitoring and follow-up may be able to receive a portion of their parenteral meningitis treatment on an outpatient basis.17,28 A management algorithm for adults with suspected bacterial meningitis, as recommended by the Infectious Diseases Society of America (IDSA), is summarized in Figure 70–2.
Parenteral (IV) therapy is administered for the full course of therapy for CNS infections to ensure adequate CSF penetration throughout the course of treatment. Antibiotic treatment (and dexamethasone, if used as a treatment adjunct) reduces the inflammation associated with meningitis, which, in turn, reduces the penetration of some antibiotics into the CSF. To ensure adequate antibiotic concentrations throughout the treatment course, parenteral administration is continued for the full treatment course. Carefully selected patients who have close medical monitoring and follow-up may be able to receive a portion of their parenteral meningitis treatment on an outpatient basis.17,28 A management algorithm for adults with suspected bacterial meningitis, as recommended by the Infectious Diseases Society of America (IDSA), is summarized in Figure 70–2.
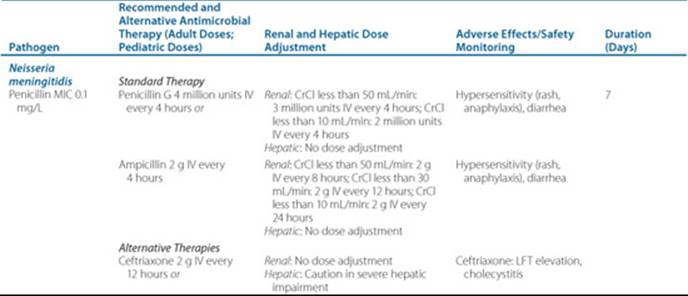
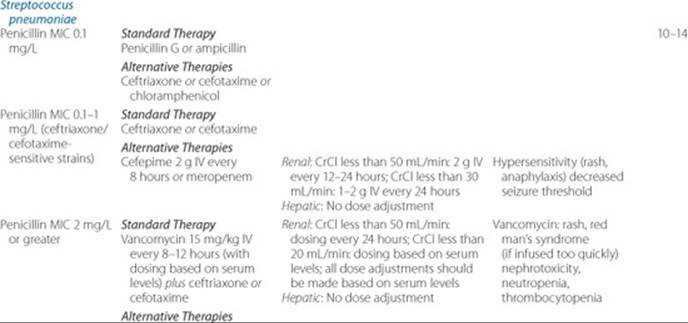
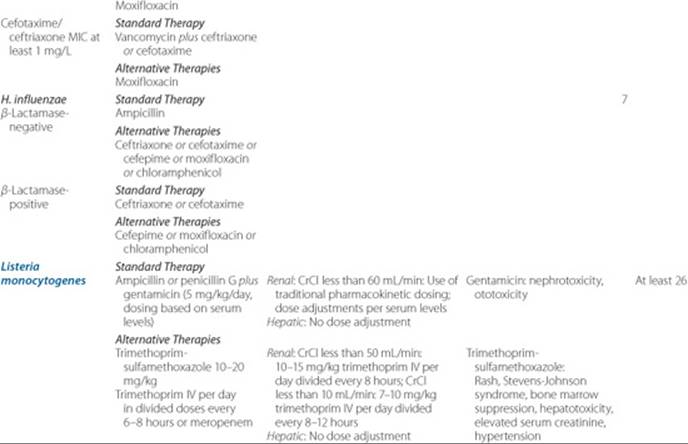
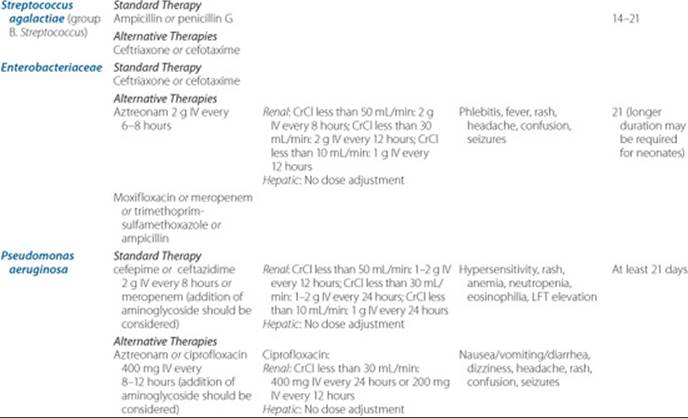
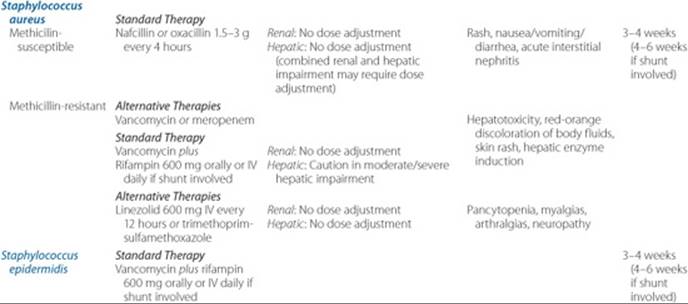
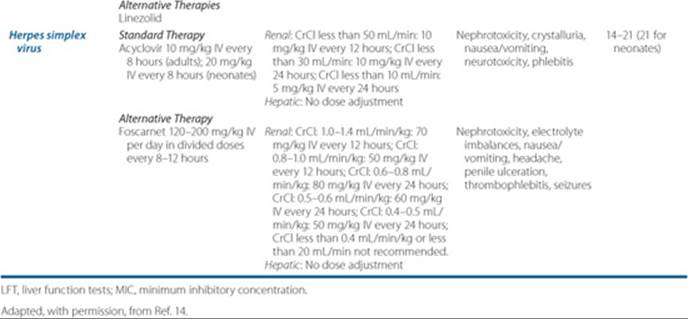
Table 70–3 Pathogen-Based Definitive Treatment for CNS Infections

Empirical Antimicrobial Therapy
After expeditious workup (i.e., evaluation of risk factors, clinical signs and symptoms, and laboratory data) and diagnosis, prompt and aggressive antimicrobial therapy is initiated. Appropriate empirical treatment is of the utmost importance in patients with suspected CNS infections. In most patients, a diagnostic LP will be performed before beginning antibiotics, but this never should delay initiation of antimicrobials. Antibiotic pretreatment may alter the CSF profile and complicate interpretation. ![]() Empirical therapy should be directed at the most likely pathogen(s) for a specific patient, taking into account age, risk factors for infection (including underlying disease and immune dysfunction, vaccine history, and recent exposures), CSF Gram stain results, CSF antibiotic penetration, and local antimicrobial resistance patterns. Results of the CSF Gram stain may be used to help narrow empirical therapy for bacterial meningitis. In the absence of a positive Gram stain, empirical therapy should be continued for at least 48 to 72 hours, when meningitis may, in most cases, be ruled out by CSF findings inconsistent with bacterial meningitis, negative CSF culture, and negative PCR evaluations. A repeat LP may be useful in the absence of other findings. Table 70–1 outlines recommendations for empirical antibiotic therapy for bacterial meningitis by most likely pathogen(s) and patient risk factors.
Empirical therapy should be directed at the most likely pathogen(s) for a specific patient, taking into account age, risk factors for infection (including underlying disease and immune dysfunction, vaccine history, and recent exposures), CSF Gram stain results, CSF antibiotic penetration, and local antimicrobial resistance patterns. Results of the CSF Gram stain may be used to help narrow empirical therapy for bacterial meningitis. In the absence of a positive Gram stain, empirical therapy should be continued for at least 48 to 72 hours, when meningitis may, in most cases, be ruled out by CSF findings inconsistent with bacterial meningitis, negative CSF culture, and negative PCR evaluations. A repeat LP may be useful in the absence of other findings. Table 70–1 outlines recommendations for empirical antibiotic therapy for bacterial meningitis by most likely pathogen(s) and patient risk factors.
Impact of Antimicrobial Resistance on Treatment Regimens for Meningitis
Development of resistance to β-lactam antibiotics, including penicillins and cephalosporins, has significantly impacted the management of bacterial meningitis. Approximately 17% of U.S. pneumococcal CSF isolates are resistant to penicillin, and 3.5% of CSF isolates are resistant to cephalosporins.29 The Clinical and Laboratory Standards Institute (CLSI) has set a lower ceftriaxone susceptibility breakpoint for pneumococcal CSF isolates (1 mg/L) than for isolates from non-CNS sites (2 mg/L). Increasing pneumococcal resistance to penicillin G has changed empirical treatment regimens to the combination of a third-generation cephalosporin plus vancomycin. Recognition of relative and high-level resistance to N. meningitidis in the laboratory, as well as in clinical treatment failures, has led to greater use of third-generation cephalosporins for empirical therapy of meningococcal meningitis.20 Traditionally, ampicillin was the cornerstone of treatment for H. influenzae meningitis. Now, treatment of suspected or proven β-lactamase-mediated Hib meningitis requires a third-generation cephalosporin. Increasing rates of methicillin-resistant S. aureus (about one-third of staphylococcal CSF isolates) and coagulase-negative staphylococci require the use of vancomycin for empirical therapy when these pathogens are suspected.29 As previously mentioned, hospitalized patients, especially those residing in an intensive care unit, are at risk for developing meningitis secondary to gram-negative pathogens. The emergence and continued rise of multidrug resistant strains of gram-negative organisms such as Pseudomonas aeruginosa,Acinetobacter species, AmpC and extended spectrum β-lactamase (ESBL)-producing strains of Enterobacteraciae have become a recognized threat nationally. Global and local resistance patterns should be taken into account and combined with optimized pharmacodynamic dosing strategies when designing empirical treatment regimens for bacterial meningitis.

FIGURE 70–2. Management algorithm for adults with suspected bacterial meningitis. a Management algorithm is similar for infants and children with suspected bacterial meningitis. b See Table 70–1 for empirical treatment recommendations. c See text for specific recommendations for use of adjunctive dexamethasone in adults with bacterial meningitis. d See Table 70–3 for pathogen-based definitive treatment recommendations. (Adapted, with permission, from Ref. 14.)
Pathogen-Directed Antimicrobial Therapy
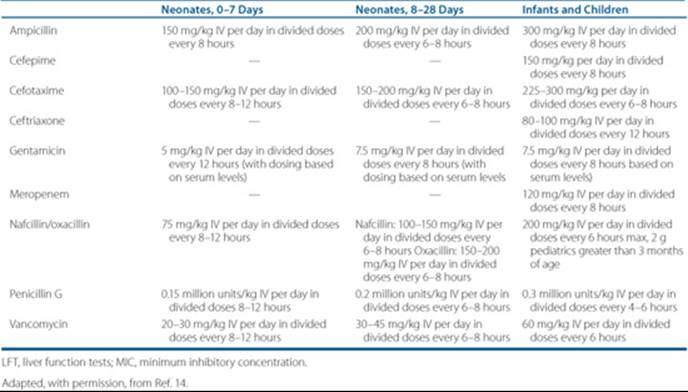
![]() Empirical antimicrobial therapy should be modified on the basis of laboratory data and clinical response. If cultures or other diagnostics, such as CSF Gram stain or bacterial antigen or antibody tests indicate a specific pathogen, therapy should be adjusted quickly as needed to ensure adequate coverage for the offending pathogen(s). Table 70–3 outlines recommended definitive pathogen-directed treatment regimens, recommended treatment duration, and key adverse effects that should be monitored during antibiotic therapy for meningitis. Treatment considerations for selected pathogens causing CNS infections are summarized below. Table 70–4 provides pediatric doses of selected agents used in bacterial meningitis treatment.
Empirical antimicrobial therapy should be modified on the basis of laboratory data and clinical response. If cultures or other diagnostics, such as CSF Gram stain or bacterial antigen or antibody tests indicate a specific pathogen, therapy should be adjusted quickly as needed to ensure adequate coverage for the offending pathogen(s). Table 70–3 outlines recommended definitive pathogen-directed treatment regimens, recommended treatment duration, and key adverse effects that should be monitored during antibiotic therapy for meningitis. Treatment considerations for selected pathogens causing CNS infections are summarized below. Table 70–4 provides pediatric doses of selected agents used in bacterial meningitis treatment.
Neisseria meningitidis Meningitis
N. meningiditis most commonly causes CNS infections in children and young adults. An estimated 1,400 to 2,800 cases of meningococcal meningitis occur annually in the United States, with a mortality of about 10%.30 From 11% to 19% of survivors of meningococcal meningitis experience long-term sequelae, including hearing loss, limb loss, and neurologic deficits.30 Nearly all meningococcal disease is caused by five serogroups: A, B, C, Y, and W-135. In the United States, serotypes B, C, and Y each are responsible for approximately 30% of cases.
Table 70–4 Pediatric Doses of Selected Agents Used in Bacterial Meningitis Treatment
Meningococcal meningitis is observed most commonly in individuals living in close quarters (such as college students and military personnel). Although infants younger than 1 year of age are at highest risk, nearly 60% of cases occur in patients over 11 years of age.30,31 N. meningitidis colonizes the nasopharynx and usually is transmitted via inhaled respiratory droplets from patients or asymptomatic carriers. A subclinical bacteremia typically ensues, seeding the meninges. Meningococcal disease is often (approximately 50%) associated with a diffuse petechial rash, and patients may experience behavioral changes. Patients may develop fulminant meningococcal sepsis, characterized by shock, DIC, and multiorgan failure.30,31 Meningococcal sepsis has a poor prognosis and carries a mortality rate of up to 80%.20 Patients with suspected meningococcal infection should be kept on respiratory isolation for the first 24 hours of treatment.4
Traditionally, high-dose penicillin G was the treatment standard for meningococcal disease. However, increasing penicillin resistance requires that third-generation cephalosporins now be used for empirical treatment until in vitro susceptibilities are known.27 Patients with a history of type I penicillin allergy or cephalosporin allergy may be treated with vancomycin. Treatment should be continued for seven days, after which no further treatment is necessary.
Prevention of meningococcal disease by vaccination is a key to reducing the incidence of meningococcal meningitis. College freshmen living in dormitories, military recruits, patients undergoing splenectomy, HIV-infected patients and patients with complement deficiency should receive the meningococcal vaccine.30 Both the older polysaccharide meningococcal vaccine and the quadrivalent conjugate meningococcal vaccine protect against four of the five serotypes causing invasive disease (A, C, Y, and W-135). Meningococcal vaccines do not protect against serotype B, which causes more than 50% of the cases of meningococcal meningitis in children younger than 2 years of age.32 Either of the two available meningococcal vaccines can be used in outbreak situations, with protective antibodies measurable within 7 to 10 days. A possible advantage of the new conjugate vaccine is that it is believed to provide a longer duration of immunity than the older polysaccharide vaccine, although clinical studies to validate the duration of protection are not yet completed. The Centers for Disease Control and Prevention (CDC) Advisory Committee on Immunization Practices and the American Academy of Pediatrics recommend that all adolescents 11 to 12 years of age receive a dose of the new quadrivalent conjugate vaccine (currently approved by the FDA for patients 11-55 years of age). Until broader indications for the conjugate vaccine are licensed, the polysaccharide vaccine is available for patients 2 to 10 years of age, as well as patients over 55 years of age.
![]() Close contacts of patients with meningococcal infections should be evaluated for antimicrobial prophylaxis. Close contacts include members of the same household, individuals who share sleeping quarters, day-care contacts, and individuals exposed to oral secretions of meningitis patients. After consultation with the local health department, close contacts should receive prophylactic antibiotics to eradicate nasopharyngeal carriage of the organism. Household contacts of patients with meningococcal meningitis have a 400- to 800-fold increased risk of developing meningitis.31 Prophylactic antibiotics should be started as soon as possible, preferably within 24 hours of exposure (and within 14 days, after which the benefit is significantly reduced). Recommended regimens, all of which are 90% to 95% effective, for adults include rifampin 600 mg orally every 12 hours for 2 days, ciprofloxacin 500 mg orally for one dose, or ceftriaxone 250 mg intramuscularly for one dose. Regimens for children include rifampin 5 mg/kg orally every 12 hours for 2 days (less than 1 month of age), rifampin 10 mg/kg orally every 12 hours for 2 days (greater than 1 month of age), or ceftriaxone 125 mg intramuscularly for one dose (less than 12 years of age).30,31 It is not known if close contacts who have been vaccinated will benefit from prophylaxis. Patients with meningococcal meningitis who are treated with antibiotics other than third-generation cephalosporins also should be considered for prophylaxis to eradicate the nasopharyngeal carrier state.32
Close contacts of patients with meningococcal infections should be evaluated for antimicrobial prophylaxis. Close contacts include members of the same household, individuals who share sleeping quarters, day-care contacts, and individuals exposed to oral secretions of meningitis patients. After consultation with the local health department, close contacts should receive prophylactic antibiotics to eradicate nasopharyngeal carriage of the organism. Household contacts of patients with meningococcal meningitis have a 400- to 800-fold increased risk of developing meningitis.31 Prophylactic antibiotics should be started as soon as possible, preferably within 24 hours of exposure (and within 14 days, after which the benefit is significantly reduced). Recommended regimens, all of which are 90% to 95% effective, for adults include rifampin 600 mg orally every 12 hours for 2 days, ciprofloxacin 500 mg orally for one dose, or ceftriaxone 250 mg intramuscularly for one dose. Regimens for children include rifampin 5 mg/kg orally every 12 hours for 2 days (less than 1 month of age), rifampin 10 mg/kg orally every 12 hours for 2 days (greater than 1 month of age), or ceftriaxone 125 mg intramuscularly for one dose (less than 12 years of age).30,31 It is not known if close contacts who have been vaccinated will benefit from prophylaxis. Patients with meningococcal meningitis who are treated with antibiotics other than third-generation cephalosporins also should be considered for prophylaxis to eradicate the nasopharyngeal carrier state.32
Streptococcus pneumoniae Meningitis
S. pneumoniae is the most common cause of meningitis in adults and in children younger than 2 years of age. Pneumococcus is associated with the highest mortality observed with bacterial meningitis in adults (20-30%), and coma and seizures are more common in pneumococcal meningitis.1-3
Patients at high risk for pneumococcal meningitis include the elderly, alcoholics, splenectomized patients, patients with sickle cell disease, and patients with cochlear implants. At least 50% of pneumococcal meningitis cases are due to a primary infection of the ears, sinuses, or lungs.
Patient Encounter 2, Part 1
BB is a 4-month-old infant who is brought to the ED with a 3-day history of excessive crying, irritability, and poor eating. His parents report a tympanic temperature of 38.2°C (100.8°F) measured at home. Vital signs and laboratory values include a rectal temperature of 39°C (102.2°F), respirations 44 per minute, and peripheral WBC of 13.8 × 103/mm3 (13.8 × 109/L), with 65% PMNs. Physical examination reveals only that BB is more irritable while being held than when allowed to lie still. The child has not initiated routine vaccine schedule since receiving HBV initial dose at birth.
What signs and symptoms consistent with meningitis are present in BB?
What clues to causative pathogen are present in BB?
What empiric antimicrobial regimen should be started?
High-dose penicillin G traditionally has been the drug of choice for the treatment of pneumococcal meningitis. However, due to increases in pneumococcal resistance, the preferred empirical treatment now includes a third-generation cephalosporin in combination with vancomycin.17 All CSF isolates should be tested for penicillin and cephalosporin resistance by methods endorsed by the CLSI. Once in vitro sensitivity results are known, therapy may be tailored (Table 70–3). Patients with a history of type I penicillin allergy or cephalosporin allergy may be treated with vancomycin. Treatment should be continued for 10 to 14 days, after which no further maintenance therapy is required. Antimicrobial prophylaxis is not indicated for close contacts.
Administration of vaccines to high-risk individuals is a key strategy to reduce the risk of invasive pneumococcal disease. The 23-valent pneumococcal vaccine targets sero-types that account for over 90% of invasive disease in high-risk patients. However, the 23-valent vaccine does not produce a reliable immunologic response in children younger than 2 years of age, nor does it reduce pneumococcal carriage. The 7-valent pneumococcal protein-polysaccharide conjugate vaccine introduced in 2,000 targets the seven most common serotypes in children and provides protection (94% reduction) against invasive pneumococcal disease (such as sepsis and meningitis) in children younger than 5 years of age.33 Widespread administration of the 7-valent conjugate vaccine to children has also contributed to a 28% reduction in invasive pneumococcal disease in adults.7 Unlike the 23-valent vaccine, the 7-valent vaccine reduces carriage and transmission. S. pneumoniae remains the most common cause of bacterial meningitis in children, with nearly 50% of strains due to nonvaccine serotypes.8
Haemophilus influenzae Meningitis
Prior to the introduction of the Hib conjugate vaccine, H. influenzae type b was the most common cause of bacterial meningitis in the United States.5 Routine inoculation of pediatric patients against Hib since 1991 has reduced the incidence of invasive Hib disease (i.e., meningitis and sepsis) in children younger than 5 years of age by 99%,6 with mortality from Hib meningitis now less than 5%.2 The Hib vaccine is also recommended for patients undergoing splenectomy. Hib meningeal disease is often associated with a parameningeal focus such as a sinus or middle ear infection. Increases in β-lactamase-mediated resistance have changed the empirical treatment of choice from ampicillin to third-generation cephalosporins (e.g., ceftriaxone and cefotaxime). Treatment should be continued for 7 days, after which no further maintenance therapy is required.
Patient Encounter 2, Part 2
BB underwent lumbar puncture. Initial results from CSF studies are WBC 1.76 × 103/mm3 (1.76 × 109/L) with 79% PMNs, protein 265 mg/dL (2,650 mg/L), glucose 30 mg/dL (1.67 mmol/L), with a concurrent serum glucose of 110 mg/dL (6.1 mmol/L). Gram stain shows gram-positive cocci and culture results confirm S. pneumoniae infection. The patient is admitted to an acute care unit and remains clinically stable.
What complications is he at risk for acutely? What potential long-term complications may result?
How can his antibiotic regimen be streamlined at this time?
How long should the antibiotics be continued?
![]() Close contacts of patients with H. influenzae type B meningitis should be evaluated for antimicrobial prophylaxis. The risk of Hib meningitis in close contacts may be up to 200- to 1,000-fold higher than in the general population.10 Invasive Hib disease, including meningitis, should be reported to the local health department and the CDC. Prophylaxis to eliminate nasal and oropharyngeal carriage of Hib in exposed individuals should be initiated after consultation with local health officials. Rifampin (600 mg/day for adults; 20 mg/kg/day for children, maximum of 600 mg/day) is administered for 4 days.16Rifampin prophylaxis is not necessary for individuals who have received the full Hib vaccine series. Exposed, unvaccinated children between 12 and 48 months of age should receive one dose of vaccine, and unvaccinated children 2 to 11 months of age should receive three doses of vaccine, as well as rifampin prophylaxis.16 Because of prior vaccine shortages, it cannot be assumed that all children have been vaccinated. Further, some children have not received all childhood vaccines because of parental fears regarding vaccine safety.
Close contacts of patients with H. influenzae type B meningitis should be evaluated for antimicrobial prophylaxis. The risk of Hib meningitis in close contacts may be up to 200- to 1,000-fold higher than in the general population.10 Invasive Hib disease, including meningitis, should be reported to the local health department and the CDC. Prophylaxis to eliminate nasal and oropharyngeal carriage of Hib in exposed individuals should be initiated after consultation with local health officials. Rifampin (600 mg/day for adults; 20 mg/kg/day for children, maximum of 600 mg/day) is administered for 4 days.16Rifampin prophylaxis is not necessary for individuals who have received the full Hib vaccine series. Exposed, unvaccinated children between 12 and 48 months of age should receive one dose of vaccine, and unvaccinated children 2 to 11 months of age should receive three doses of vaccine, as well as rifampin prophylaxis.16 Because of prior vaccine shortages, it cannot be assumed that all children have been vaccinated. Further, some children have not received all childhood vaccines because of parental fears regarding vaccine safety.
Listeria monocytogenes Meningitis
L. monocytogenes is an intracellular gram-positive bacillus that has been reported to contaminate certain foods, such as soft cheese, unpasteurized milk, raw meats and fish, processed meats, and raw vegetables. Bacteria from contaminated foods colonize the GI tract, pass into the bloodstream, and overcome natural cellular immune responses to cause infection. L. monocytogenes meningitis, usually observed in patients at extremes of age and in immunocompromised patients with depressed cellular immunity (including patients with leukemia, solid-organ transplants, and HIV/AIDS), has an overall mortality rate of up to 30%.34,35
Only a limited number of antibiotics show bactericidal activity against Listeria. The combination of high-dose ampicillin or penicillin G and an aminoglycoside is synergistic and bactericidal against Listeria.A total treatment course of at least 3 weeks is required. Because of concerns about the risk of nephrotoxicity with an extended treatment course of aminoglycosides, patients are treated with combination therapy for 10 days and may finish out the remainder of their treatment with ampicillin or penicillin alone.34 In penicillin-allergic patients, trimethoprim-sulfamethoxazole is the agent of choice due to documented in vitro bactericidal activity against Listeria, as well as good CNS penetration. Vancomycin and cephalosporins are not effective treatments for Listeria meningitis. Prophylaxis is not needed for close contacts, nor is suppressive therapy indicated. Patients with severe depression of cell-mediated immunity should be advised to avoid foods that may be contaminated with Listeria.
Group B Streptococcus Meningitis
Infection with group B Streptococcus (such as S. agalactiae) is the most common cause of neonatal sepsis and meningitis. One of every four to five pregnant women is a carrier of group B Streptococcus in the vagina or rectum. Group B streptococci can be acquired during childbirth after exposure to infected secretions from the mother’s birth canal or rectum. Neonates born to women who are carriers are at very high risk (1 of every 100-200 babies) of developing invasive group B streptococcal disease, including sepsis and meningitis.36 Neonatal meningitis is associated with significant morbidity and mortality. Synergistic treatment with penicillin or ampicillin, plus gentamicin, for 14 to 21 days is recommended for the treatment of group B streptococcal meningitis.17
To reduce the risk of clinical group B streptococcal disease in neonates, pregnant women should be screened at 35 to 37 weeks’ gestation to determine if they are carriers of group B streptococci.36 Intrapartum antibiotics (e.g., penicillin or ampicillin) are recommended for pregnant women with the following characteristics: group B streptococcal carrier state detected at screening, history of group B streptococcal bacteriuria at any time during pregnancy, and history of delivery of infant with invasive group B streptococcal disease.36
Gram-Negative Bacillary Meningitis
Meningitis caused by enteric gram-negative bacilli is an important cause of morbidity and mortality in populations at risk, including those with diabetes, malignancy, cirrhosis, immunosuppression, advanced age, parameningeal infection, and/or a defect allowing communication from skin to CNS (such as neurosurgery, congenital defects, or cranial trauma).10
The optimal treatment for gram-negative bacillary meningitis is not well defined. The introduction of extended-spectrum cephalosporins has improved patient outcomes significantly. While the third-generation cephalosporins ceftriaxone and cefotaxime provide good coverage for most enterobacteriaceae, these antibiotics are not active against P. aeruginosa. Ceftazidime, cefepime, and carbapenems are effective in pseudomonal meningitis.25,27 Addition of an aminoglycoside may improve treatment results; however, CNS penetration of aminoglycosides is extremely poor, even in the setting of inflamed meninges. Intrathecal or intraventricular administration of aminoglycosides may be useful, but intraventricular antibiotics have been associated with increased mortality in neonates.25,37 Intrathecal therapy is accomplished by administering the antibiotic into the CSF via LP, whereas intraventricular therapy is usually administered into a reservoir implanted in the ventricles of the brain.
Initial therapy of suspected or documented pseudomonal meningitis should include an extended-spectrum β-lactam (e.g., ceftazidime, cefepime, or meropenem) plus an aminoglycoside (preferably tobramycin or amikacin). Although the carbapenem imipenem-cilastatin has similar activity to these β-lactams, its use is not recommended in meningitis because of the risk of seizures. Aztreonam, high-dose ciprofloxacin, and colistin are alternative treatments for pseudomonal meningitis. Local therapy (i.e., intrathecal or intraventricular therapy) may be indicated in patients with gram-negative bacillary meningitis (especially infections caused by multidrug-resistant P. aeruginosa) or in patients who fail to improve on IV antibiotics alone. In cases of multidrug-resistant pathogens, alternative pharmacodynamic dosing strategies such as continuous or extended infusion of β-lactam antimicrobials may be considered to optimize target attainment (time greater than minimum inhibitory concentration). Given the differences in local hospital resistance patterns, administration of pathogen-directed treatment is very important after microbiology results become available. Therapy for gram-negative bacillary meningitis should be continued for at least 21 days.
Postoperative Infections in the Neurosurgical Patient and Shunt Infections
Patients who undergo neurosurgical procedures or have invasive or implanted foreign devices (such as CSF shunts, intraspinal pumps or catheters, or epidural catheters) are at risk for CNS infections. Key pathogens in postneuro-surgical infections include coagulase-negative staphylococci, S. aureus, streptococci, propionobacteria, and gram-negative bacilli, including P. aeruginosa. Clinical signs and symptoms may be similar to those of other CNS infections, and there also may be evidence of malfunction of implanted hardware or visible signs of a postoperative wound infection.
Empirical therapy for postoperative infections in neurosurgical patients (including patients with CSF shunts) should include vancomycin in combination with either cefepime, ceftazidime, or meropenem. Linezolid reaches adequate CSF concentrations and resolves cases of meningitis refractory to vancomycin.35,38 However, data with linezolid are limited. The addition of rifampin should be considered for treatment of shunt infections. When culture and sensitivity data are available, pathogen-directed antibiotic therapy should be administered. Removal of infected devices is desirable; aggressive antibiotic therapy (including high-dose IV antibiotic therapy plus intraventricular vancomycin and/or tobramycin) may be effective for patients in whom hardware removal is not possible.39 If methicillin-resistant S. aureus is identified as the causative organism, daptomycin may be considered an alternative therapy.40
The use of prophylactic antibiotics against meningitis postcraniotomy remains controversial. A meta-analysis suggests that prophylaxis reduces rates of postoperative meningitis by nearly one-half.42 Other studies have demonstrated no benefit and there is limited data on organism-specific reductions in infection rate.43,44 Additionally, breakthrough meningitis that does occur may be a result of drug-resistant pathogens.43
Brain abscesses are localized collections of pus within the cranium. These infections are difficult to treat due to the presence of walled-off infections in the brain tissue that are hard for some antibiotics to reach. In addition to appropriate antimicrobial therapy (a discussion of which is beyond the scope of this chapter), surgical debridement is of ten required as an adjunctive measure. Surgical debridement may also be required in the management of neurosurgical postoperative infections.
Viral Encephalitis and Meningitis
Viral encephalitis and meningitis may mimic bacterial meningitis on clinical presentation but often can be differentiated by CSF findings (Table 70–2). The most common viral pathogens are enteroviruses, which cause approximately 85% of cases of viral CNS infections.10 Other viruses that may cause CNS infections include arboviruses, HSV, cytomegalovirus, varicella-zoster virus, rotavirus, coronavirus, influenza viruses A and B, West Nile virus, and Epstein-Barr virus. Viral CNS infections are acquired through hematogenous or neuronal spread.10 Most cases of enteroviral meningitis or encephalitis are self-limiting with supportive treatment.41 However, arbovirus, West Nile virus, and Eastern equine virus infections are associated with a less favorable prognosis.
In contrast to other viral encephalitides, HSV type 1 and 2 encephalitis are treatable. Although rare (1 case per 250,000 population per year in the United States), HSV encephalitis is a serious, life-threatening infection.45 Over 90% of HSV encephalitis in adults is due to HSV type 1, whereas HSV type 2 predominates in neonatal HSV encephalitis (greater than 70%).46 HSV encephalitis is the result of reactivation of a latent infection (two-thirds of cases) or a severe case of primary infection (one-third). Without effective treatment, the mortality rate may be as high as 85% and survivors often have significant residual neurologic deficits. In accordance with 2008 IDSA guidelines, high-dose IV acyclovir is the drug of choice, given for 2 to 3 weeks at a dose of 10 mg/kg intravenously every 8 hours in adults, based on ideal body weight, and for 3 weeks at a dose of 20 mg/kg intravenously every 8 hours in neonates.47,48 Patients receiving acyclovir should maintain adequate hydration (consider continuous IV hydration in those receiving high-dose acyclovir) to help prevent acute kidney injury secondary to crystal nephropathy.47,48Foscarnet 120 to 200 mg/kg/day divided every 8 to 12 hours for 2 to 3 weeks is the treatment of choice for acyclovir-resistant HSV isolates.47,48
Adjunctive Dexamethasone Therapy
The adjunctive agent dexamethasone improves outcomes in selected patient populations with meningitis. Dexamethasone inhibits the release of proinflammatory cytokines and limits the CNS inflammatory response stimulated by infection and antibiotic therapy.
Clinical benefit in reducing neurologic deficits (primarily by reducing hearing loss) has been observed in infants and children with H. influenzae meningitis, as well as other pathogens causing meningitis, if dexamethasone is initiated prior to antibiotic therapy.1,13 The American Academy of Pediatrics recommends dexamethasone (0.15 mg/kg IV every 6 hours for 2–4 days) for infants and children at least 6 weeks of age with Hib meningitis and consideration of dexamethasone in pneumococcal meningitis.17,49 In contrast to this recommendation, a large multicenter cohort study failed to show any mortality benefit of adjunctive dexamethasone therapy regardless of age or responsible pathogen (S. pneumoniae or N. meningitidis).50 Dexamethasone should be initiated 10 to 20 minutes before or no later than the time of initiation of antibiotic therapy; it is not recommended for infants and children who have already received antibiotic therapy because it is unlikely to improve treatment outcome in these patients. There are insufficient data to make a recommendation regarding the use of adjunctive dexamethasone therapy in neonatal meningitis.
In adults, a significant benefit was observed with dexa-methasone over placebo in reducing meningitis complications, including death, particularly in patients with pneumococcal meningitis.51 The IDSA recommends dexamethasone 0.15 mg/kg intravenously every 6 hours for 2 to 4 days (with the first dose administered 10 to 20 minutes before or with the first dose of antibiotics) in adults with suspected or proven pneumococcal meningitis.17Dexamethasone is not recommended for adults who have already received antibiotic therapy. Some clinicians would administer dexamethasone to all adults with meningitis pending results of laboratory tests. Benefit of dexamethasone in bacterial meningitis in a HIVpositive population has not been clearly established.52
There is some controversy regarding the administration of dexamethasone to patients with pneumococcal meningitis caused by penicillin- or cephalosporin-resistant strains, for which vancomycin would be required. Animal models indicate that concurrent steroid use reduces vancomycin penetration into the CSF by 42% to 77% and delays CSF sterilization due to reduction in the inflammatory response.27 A prospective evaluation in patients with pneumococcal meningitis receiving vancomycin and adjunctive dexa-methasone demonstrated that adequate concentrations of vancomycin, nearly 30% of serum concentrations, were achievable in the CSF, provided appropriate vancomycin dosage was utilized.53 Treatment failures have been reported in adults with resistant pneumococcal meningitis who were treated with dexamethasone, but the risk-benefit of using dexamethasone in these patients cannot be defined at this time. Animal models indicate a benefit of adding rifampin in patients with resistant pneumococcal meningitis whenever dexamethasone is used.25,27
OUTCOME EVALUATION
Monitor patients with CNS infections continuously throughout their treatment course to evaluate their progress toward achieving treatment goals, including relief of symptoms, eradication of infection, and reduction of inflammation to prevent death and the development of neurologic deficits. These treatment goals are best achieved by appropriate parenteral antimicrobial therapy, including empirical therapy to cover the most likely pathogens, followed by directed therapy after culture and sensitivity results are known. ![]() Components of a monitoring plan to assess efficacy and safety of antimicrobial therapy of CNS infections include clinical signs and symptoms and laboratory data (such as CSF findings, culture, and sensitivity data).
Components of a monitoring plan to assess efficacy and safety of antimicrobial therapy of CNS infections include clinical signs and symptoms and laboratory data (such as CSF findings, culture, and sensitivity data).
Patient Encounter 2, Part 3
Further results reveal BB had confirmed bacterial meningitis secondary to S. pneumoniae, serotype 6B. It was noted that BB had not received any vaccinations since birth. The parents are concerned and inquire about the need for antibiotic prophylaxis for the family and vaccination for BB.
Who should receive antimicrobial prophylaxis for S. pneumoniae?
Who should receive vaccination against pneumococcal disease?
How is vaccination important in the prevention of invasive pneumococcal disease, specifically noting BB?
During the patient’s treatment course, monitor clinical signs and symptoms at least three times daily. Trends are more important than one-time assessments. Expect fever, headache, nausea and vomiting, and malaise to begin to improve within 24 to 48 hours of initiation of antimicrobial therapy and supportive care. Evaluate the patient for resolution of neurologic signs and symptoms, such as altered mental status and nuchal rigidity, as the infection is eradicated and inflammation is reduced within the CNS. Expect improvement and subsequent resolution of signs and symptoms as the treatment course continues. At the time of hospital discharge, arrange outpatient follow-up for several weeks to months depending on the causative pathogen, clinical treatment course, and patient’s underlying comorbidities. Specifically evaluate patients for the presence of residual neurologic deficits.
Monitoring of laboratory tests is important in patients receiving treatment for CNS infections. Monitor CSF and blood cultures so that antimicrobial therapy can be tailored to the etiologic organisms. Follow-up cultures may be obtained to prove eradication of the organism(s) or treatment failure. Although repeat LP generally is not performed, consider repeat LP for patients who do not respond clinically after 48 hours of appropriate antimicrobial therapy, especially those with resistant pneumococcus who receive dexamethasone.13 Other candidates for repeat LP include the following: those with infection with gram-negative bacilli, prolonged fever, and recurrent meningitis. Repeat the LP in neonates to determine the duration of therapy. Repeat LP also may be performed to relieve elevated intracranial pressure. Expect repeat blood cultures to become negative quickly during therapy and the serum WBC count to improve and normalize with appropriate antimicrobial therapy.
Patient Care and Monitoring
1. Assess the patient’s signs, symptoms, and risk factors for meningitis. Do these offer any clues to the offending pathogen?
2. Determine if the patient can undergo an immediate LP or if the LP should be delayed until a CNS mass lesion can be ruled out. If the LP is delayed, blood cultures should be drawn and appropriate empirical antimicrobial therapy initiated immediately.
3. Based on patient-specific data, local resistance patterns, and other relevant data, design an appropriate empirical antimicrobial regimen directed at the most likely pathogens; empirical regimens should consist of high-dose IV cidal therapy.
4. Determine if adjunctive dexamethasone therapy is indicated; if so, start steroid therapy 15-20 minutes before the first dose of antimicrobial therapy.
5. Provide supportive care for patients with CNS infections, including hydration, electrolyte replacement, antipyretics, analgesics, and antiepileptic drugs.
6. Monitor culture and sensitivity data from the microbiology laboratory to determine whether any refinements are needed in the patient’s treatment regimen. Design a therapeutic plan to finish out the patient’s course of therapy for acute meningitis.
7. Monitor the patient’s response to therapy (i.e., clinical signs/symptoms and laboratory data), as well as the development of complications, including seizures and hearing loss. Dexamethasone therapy may reduce antibiotic penetration, so antimicrobial drug dosing may have to be increased (especially vancomycin) to achieve dequate CSF levels. Serum levels of vancomycin should be measured and doses titrated to ensure adequate CNS concentrations. Evaluate whether intraventricular or intrathecal antibiotics are indicated.
8. Perform ongoing surveillance for adverse drug reactions, drug allergies, and drug interactions.
9. Determine whether prophylaxis is indicated for close contacts of patients with CNS infections. Close contacts should be located for patients with suspected meningococcal or Hib meningitis. After consultation with the local health department, antibiotic prophylaxis should be provided promptly to these individuals to avoid secondary disease.
10. Evaluate whether the patient is a candidate for finishing out his or her course of parenteral treatment on an outpatient basis. If so, the importance of close medical follow-up and medication compliance should be stressed to the patient and his or her family.
11. Consider how to minimize the patient’s risk of contracting the current (and other) CNS infections in the future; administer appropriate vaccines after recovery from the acute infection.
12. Arrange for patient follow-up after discharge from the hospital. Continue to monitor for neurologic sequelae for several months after completion of treatment, and educate the patient and family in this regard. Serious complications that may occur include, among others, hearing loss, hemiparesis, quadriparesis, muscular hypertonia, ataxia, seizure disorders, mental retardation, learning disabilities, and obstructive hydrocephalus.
Evaluate antimicrobial dosing regimens to ensure efficacy of the treatment regimen. Trough vancomycin concentrations of 15 to 20 mg/L are recommended for the treatment of CNS infections.17 Monitor patients for drug adverse effects, drug allergies, and drug interactions. The specific safety monitoring plan will depend on the antibiotic(s) used (Table 70–3). Pay close attention to concomitant medications in patients on rifampin for treatment or prophylaxis. Rifampin is a potent inducer of hepatic metabolism and may reduce the efficacy of other drugs metabolized by the cytochrome P-450 3A enzyme pathway.
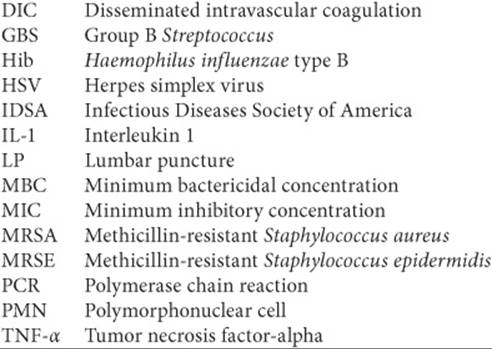
Abbreviations Introduced in This Chapter
![]()
 Self-assessment questions and answers are available at http://www.mhpharmacotherapy.com/pp.html.
Self-assessment questions and answers are available at http://www.mhpharmacotherapy.com/pp.html.
REFERENCES
1. van de Beek D, de Gans J, McIntyre P, Prasad K. Corticosteroids for acute bacterial meningitis. Cochrane Database Syst Rev 2003;3:CD004405.
2. van de Beek D, de Gans J, Spanjaard L, et al. Clinical features and prognostic factors in adults with bacterial meningitis. N Engl J Med 2004;351(18):1849–1859.
3. Aronin SI, Peduzzi P, Quagliarello VJ. Common-acquired bacterial meningitis: Risk stratification for adverse clinical outcome and effect of antibiotic timing. Ann Intern Med 1998;129(11):862–869.
4. van de Beek D, de Gans J, Tunkel AR, Wijdicks EFM. Community-acquired bacterial meningitis in adults. N Engl J Med 2006;354:44–53.
5. Schuchat A, Robinson K, Wenger JD, et al. Bacterial meningitis in the United States in 1995. N Engl J Med 1997;337(14):970–976.
6. Centers for Disease Control and Prevention. Progress toward elimination of Haemophilus influenzae type b invasive disease among infants and children—United States, 1998–2000. MMWR Recomm Rep 2002; 51(RR11):234–237.
7. Lexau CA, Lynfield R, Danila R, et al. Changing epidemiology of invasive pneumococcal disease among older adults in the era of pediatric pneumococcal conjugate vaccine. JAMA 2005;294(16):2043–2051.
8. Nigrovic LE, Kuppermann N, Malley R, et al. Children with bacterial meningitis presenting to the emergency department during the pneumococcal conjugate vaccine era. Acad Emerg Med 2008;15:522–528.
9. Sejvar JJ. The evolving epidemiology of viral encephalitis. Curr Opin Neurol 2006;19:350–357.
10. Mitropoulous IF, Hermsen ED, Schafer JA, Rotschafer JC. Central nervous system infections. In: DiPiro JT, Talbert RL, Yee GC, et al., eds. Pharmacotherapy: A Pathophysiologic Approach, 7th ed. New York City: McGraw-Hill; 2008:1743–1760.
11. Khetsuriani N, Holman RC, Anderson LJ. Burden of encephalitis-associated hospitalizations in the United States, 1988–1997. Clin Infect Dis 2002;35:175–182.
12. Chamberlain MC. Neoplastic meningitis. J Clin Oncol 2005;23(15): 3605–3613.
13. Moris G, Garcia-Monco JC. The challenge of drug-induced aseptic meningitis. Arch Intern Med 1999;159(11):1185–1194.
14. Scheld WM, Koedel U, Nathan B, Pfister HW. Pathophysiology of bacterial meningitis: mechanism(s) of neuronal injury. J Infect Dis 2002;186(Suppl 2):S225–S233.
15. Kim KS. Pathogenesis of bacterial meningitis: From bacteraemia to neuronal injury. Nat Rev Neurosci 2003;4:376–385.
16. Bashir HE, Laundy M, Booy R. Diagnosis and treatment of bacterial meningitis. Arch Dis Child 2003;88:615–620.
17. Tunkel AR, Hartman BJ, Kaplan SL, et al. Practice guidelines for the management of bacterial meningitis. Clin Infect Dis 2004;39:1267–1284.
18. Choi C. Bacterial meningitis in aging adults. Clin Infect Dis 2001;33:1380–1385.
19. Swartz MN. Bacterial meningitis—A view of the past 90 years. N Engl J Med 2004;351(18):1826–1828.
20. van Deuren M, Brandtzaeg P, van der Meer JWM. Update on meningococcal disease with emphasis on pathogenesis and clinical management. Clin Microbiol Rev 2000;13(1):144–166.
21. Lu CH, Huang CR, Chang, WN, et al. Community-acquired bacterial meningitis in adults: The epidemiology, timing of appropriate antimicrobial therapy, and prognostic factors. Clin Neurol Neurosurg 2002;104:352–358.
22. Miner JR, Heegaard W, Mapes A, Biros M. Presentation, time to antibiotics, and mortality of patients with bacterial meningitis at an urban county medical center. J Emerg Med 2001;21:387–392.
23. Radetsky M. Duration of symptoms and outcome in bacterial meningitis: An analysis of causation and the implications of a delay in diagnosis. Pediatr Infect Dis J 1992;11:694–698.
24. Schaad UB, Suter S, Gianella-Borradori A, et al. A comparison of ceftriaxone and cefuroxime for the treatment of bacterial meningitis in children. N Engl J Med 1990;322(3):141–147.
25. Quagliarello VJ, Scheld WM. Treatment of bacterial meningitis. N Engl J Med 1997;336(10):708–716.
26. Pankey GA, Sabath LR. Clinical relevance of bacterio-static versus bactericidal mechanisms of action in the treatment of gram-positive bacterial infections. Clin Infect Dis 2004;38:864–870.
27. Sinner SW, Tunkel AR. Antimicrobial agents in the treatment of bacterial meningitis. Infect Dis Clin N Am 2004;18:581–602.
28. Tice AD, Strait K, Ramey R, et al. Outpatient parenteral antimicrobial therapy for central nervous system infections. Clin Infect Dis 1999;29:1394–1399.
29. Jones ME, Draghi DC, Karlowsky JA, Sahm DF, Bradley JS. Prevalence of antimicrobial resistance in bacteria isolated from central nervous system specimens as reported by U.S. hospital laboratories from 2000 to 2002 (Online. Updated March 25, 2004). Ann Clin Microb 2004;3:3 (online journal published March 25, 2004).
30. Centers for Disease Control and Prevention. Prevention and control of meningococcal disease. MMWR Recomm Rep 2005;54(RR07): 1–21.
31. Rosenstein NE, Perkins BA, Stephens DS, Popovic T, Hughes JM. Meningococcal disease. N Engl J Med 2001;344(18):1378–1388.
32. Campos-Outcalt D. Meningococcal vaccine: New product, new recommendations. J Fam Pract 2005;54(4):324–326.
33. Centers for Disease Control and Prevention. Direct and indirect effects of routine vaccination of children with 7-valent pneumococcal conjugate vaccine on incidence of invasive pneumococcal disease—United States, 1998–2003. Morb Mortal Wkly Rep 2005;54(36):893–897.
34. Mylonakis D, Hohmann EL, Calderwood SB. Central nervous system infection with Listeria monocytogenes: 33 years’ experience at a general hospital and review of 776 episodes from the literature. Medicine 1998;77(5):313–336.
35. Hof H. An update on the medical management of Listeriosis. Expert Opin Pharmacother 2004;5(8):1727–1735.
36. Centers for Disease Control and Prevention. Prevention of perinatal Group B streptococcal disease. MMWR Recomm Rep 2002;51(RR11): 1–22.
37. Shah S, Ohlsson A, Shah V. Intraventricular antibiotics for bacterial meningitis in neonates. Cochrane Database Syst Rev 2004;4:CD004496.
38. Villani P, Regazzi MB, Marubbi F, et al. Cerebrospinal fluid linezolid concentrations in postneurosurgical central nervous system infections. Antimicrob Agents Chemother 2002;46(3):936–937.
39. Anderson EJ, Yogev R. A rational approach to the management of ventricular shunt infections. Pediatr Infect Dis J 2005;24:557–558.
40. Lee DH, Palermo B, Chowdhury M. Successful treatment of methicillin-resistant Staphylococcus aureus meningitis with daptomycin. Clin Infect Dis 2008;47:588–589.
41. Sawyer MH. Enterovirus infections: Diagnosis and treatment. Pediatr Infect Dis J 1999;18(12):1033–1040.
42. Barker FG. Efficacy of prophylactic antibiotics against meningitis after craniotomy: A meta-analysis. Neurosurgery 2007;60:887–894.
43. Korinek AM, Golmard JL, Elcheick A, et al. Risk factors for neurosurgical site infections after craniotomy: A critical reappraisal of antibiotic prophylaxis on 4,578 patients. Br J Neurosurg 2005;19: 155–162.
44. Reichert MC, Medeiros EA, Ferraz FA. Hospital-acquired meningitis in patients undergoing craniotomy: Incidence, evolution, and risk factors. Am J Infect Control 2002;30:158–164.
45. Tyler KL. Herpes simplex virus infections of the central nervous system: Encephalitis and meningitis, including Mollaret’s. Herpes 2004;11(Suppl 2):57A–64A.
46. Kimberlin D. Herpes simplex virus, meningitis and encephalitis in neonates. Herpes 2004;11(Suppl 2):65A–76A.
47. Tunkel AR, Glaser CA, Bloch KC, et al. The management of encephalitis: Clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis 2008;47:303–327.
48. Roos KL. Encephalitis. Neurol Clin 1999;17:813–833.
49. American Academy of Pediatrics. Pneumococcal infections. In: Pickering, LK, ed. Red Book: 2003 Report of the Committee on Infectious Diseases, 26th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2003:490–500.
50. Mongelluzzo J, Mohamad Z, Ten Have TR, Shah SS. Corticosteroids and mortality in children with bacterial meningitis. JAMA2008;299(17):2048–2055.
51. de Gans J, van de Beek D, for the European Dexamethasone in Adulthood Bacterial Meningitis Study Investigators. N Engl J Med 2002;347(20):1549–1556.
52. Scarborough M, Gordon SB, Whitty CJM, et al. Corticosteroids for bacterial meningitis in adults in Sub-Saharan Africa. N Engl J Med 2007;357:2441–2450.
53. Ricard JD, Wolff M, Lacherade JC, et al. Levels of vancomycin in cerebrospinal fluid of adult patients receiving adjunctive corticosteroids to treat pneumococcal meningitis: A prospective multicenter observational study. Clin Infect Dis 2007;44:250–255.