Water is a complex and incompletely understood chemical compound. The purest form of water is freshly formed rain as it leaves the cloud. It is also a very high-energy form of water. In the journey from rain cloud to final delivery tap, much of this energy is expended in acquiring various impurities as solute or suspension.
Improved dialysis technology has made high-purity water critical for dialysis fluid preparation. Fortunately the science of water purification has made parallel advances. Enhanced membranes for reverse osmosis, ultrafiltration (UF) devices to screen out endotoxins as well as bacteria, and improved monitoring systems are being applied in the renal community.
What impurities may be present in tap water?
Three categories of contaminating substances can cause patient injury or equipment malfunction: (1) chemical solutes, (2) bacteria or bacterial products, and (3) particulate matter. Of these, the chemical and bacterial contaminants may be directly harmful to patients receiving dialysis.
How do impurities get into water?
Falling rainwater passing through the air contacts carbon dioxide and sulfur dioxide, forming carbonic and sulfuric acid in weak solution. Upon hitting the ground, this water encounters limestone and other minerals to form calcium bicarbonate and sulfate, magnesium carbonate, and other salts. Calcium carbonate is the most prevalent impurity in tap water and accounts for most of its hardness.
What other inorganic chemicals may be present in tap water?
Sodium, chloride, iron, aluminum, nitrates, manganese, copper, zinc, iodide, and fluoride are common ionic constituents. The types of mineral present in the geographic area and the time the water is in contact with them determine the content.
Trace elements that may be present include arsenic, silver, strontium, selenium, chromium, lead, cadmium, cyanide, barium, tin, and others.
Are these chemicals harmful?
Nitrates and chloramines may cause methemoglobinemia, in which red cell hemoglobin cannot transport oxygen. Copper in excess may cause hemolysis. Manganese can be toxic, and iron may possibly be toxic. Fluoride is believed to aggravate uremic bone disease; it does accumulate in bone, and it is toxic to enzyme systems. Tin has been found in significantly higher quantity in tissues of dialyzed uremic patients than in nonuremic individuals. Aluminum accumulates and is related to dialysis dementia syndrome, as well as to a form of anemia and osteodystrophy. Zinc causes gastrointestinal upset and may produce anemia. In areas of radioactivity, the presence of strontium-90 (90Sr) may pose a danger.
Are there other materials in tap water?
Nonionic organic compounds, particularly nitrogenous matter such as proteins and polypeptides, phenols, indoles, and aldehydes, may be present. Solid particles of iron, sand, and silica are frequent. Suspended material, including mud, algae, plankton, bacteria, viruses, pyrogenic matter, and dissolved gases (ammonia, carbon dioxide, chlorine), are often present. The most common soluble organic compounds are chloramines from urban water treatment systems. The content of these materials as well as ionic impurities vary with the water source, season, and distribution system.
Some water supplies have identifiable amounts of pesticides or herbicides, such as chlordane, DDT, aldrin, lindane, 2,4,4’-Trichlorobiphenyl, and others.
Most water supplies contain various kinds of bacteria. Many are not detected by routine testing for coliform organisms. Such organisms include Flavobacterium, Achromobacter, Serratia, Pseudomonas, and several atypical mycobacteria.
If a water supply meets the requirements of the safe drinking water act and environmental protection agency standards, is it safe for dialysis?
No. Contaminants in the water used to make dialysis fluid may enter the patient’s bloodstream through the dialysis membrane. In addition, most dialysis procedures use bicarbonate as the buffer. Some delivery systems, in bicarbonate mode, will not function properly if the pH is outside the range of 6.5 to 7.8. The pH of untreated tap water may be extremely acidic or extremely alkaline. It is a requirement that water, dialysate, and equipment used for the hemodialysis treatment meet the quality standards found in the Association for the Advancement of Medical Instrumentation (AAMI) publication Dialysate for Hemodialysis (ANSI/AAMI RD52:2004).
Why is special water treatment necessary to make dialyzing fluid?
During hemodialysis the amount of water that contacts the patient’s blood is more than 25 times the amount taken in by drinking. A substance present in water to only one quarter of its upper limit of safety for drinking purposes may enter the body during hemodialysis in amounts 10 to 25 times that much. Ingested water is processed by the gastrointestinal tract before reaching the bloodstream. This selective membrane can alter the rate at which foreign substances are absorbed from ingested water. In a dialyzer system the dialyzer membrane cannot select ions to be absorbed or rejected, and they pass by diffusion. Substances that are harmless in drinking water may be toxic in dialysis water.
What methods are used to treat water for use in hemodialysis?
• Filtration
• Activated carbon filters (adsorption)
• Water softeners
• Reverse osmosis (RO)
• Deionization (DI)
• Ultraviolet light exposure
What is accomplished by filtration?
Suspended particles (mud, sand, rust, algae) are removed by mechanical filtration through a wound filament or membrane cartridge or by tanks containing granular material that can be backflushed. These effectively filter particles down to about 5 mm in size. Submicron filters are available that screen out particles as small as 0.2 mm. The smaller the number of the filter, the more efficient it is at filtering substances. The number of the filter represents the size of the particle that it is capable of filtering.
What types of filters are used?
The use of multimedia depth filters (i.e., sand filters) is a very economical and efficient way to remove suspended particles by filtering the water through sand. Cartridge filters remove particulate matter by filtering the water through a very stiff or rigid device. An ultrafilter is a very thin and delicate filter that removes much smaller solutes, such as endotoxins. Ultrafilters are highly effective for the removal of fine particles, bacteria, endotoxins, and other pyrogenic matter, as well as high molecular weight organic molecules.
What is the silt density index?
The silt density index (SDI) is an indicator of the colloid and suspended particulate matter present in tap water. The measuring device indicates the pressure drop over time as the tap water crosses a 0.45-mm membrane filter. The more suspended material present, the slower the water passes. An SDI of less than 5 is required of feed water for most RO systems.
What is the action of the carbon tank?
The carbon tank contains granular activated carbon, which removes chlorine and chloramines from the water by adsorption. Chlorine and chloramines are toxic to the blood and patient exposure to these organics can be extremely harmful. Carbon filters or tanks also remove organic matter and odor-producing materials by the same method. Adsorption is a physical process that does not require a chemical reaction and is simply the process in which liquids, gases, or suspended materials cling to a surface, such as the activated carbon. The carbon tank will not remove electrolytes, such as calcium or sodium.
Two carbon tanks are required and they should be side by side, with water passing directly from the first tank into the second tank. A sample port should be present after each of them to test for chlorine and chloramines. The water immediately leaving the first tank should be sampled for chlorine and chloramines with an approved testing device. If the sample shows that the water coming out of the first tank contains chlorine, a second sample should be obtained from the water leaving the second tank. If the sample from the second testing port is within limits, operations can continue for 72 hours until a replacement bed is installed. Testing of the water should continue to ensure there is not further chlorine breakthrough. Dialysis treatments should be suspended if the sample from the second tank contains chlorine. Prior to testing, the water system should be operating for a minimum of 15 minutes in the normal operating mode so that you have a sample that represents the current status of your water. You would not want to test a sample that has been exposed to the carbon bed for a prolonged period of time. The maximum allowable level for total chlorines is 0.5 mg/L (ppm) and the maximum allowable level for chloramine is 0.1 mg/L (ppm). Chlorine and chloramine testing should be done at the beginning of each treatment day, prior to the beginning of each patient shift, or every four hours, whichever is shorter. Proper documentation of results is critical. Empty bed contact time (EBCT) is the amount of time it takes for water to flow through the carbon tanks. The AAMI standard (RD62:2006) and End-Stage Renal Disease Conditions for Coverage require an EBCT equal to or exceeding 10 minutes (minimum of 5 minutes of exposure in each tank).
The first tank removes virtually all of the chlorine, and the second tank acts as a standby or backup in the event that the first tank did not effectively remove all of the chlorine and chloramines. These tanks are sometimes referred to as the working tank and the polishing tank. The tanks must be backwashed nightly to redistribute the carbon for more effective adsorption. The polishing tank has a low flow through it and little chlorine present, making it a good location for bacterial growth. Rotating the polishing tank and the working tank will help minimize the growth of organisms and extend the life of the tanks.
Commonly, there are two types of carbon tanks: (1) portable exchange and (2) “permanent” portable exchange. Portable exchange tanks are “changed out” on a cycle that is developed by the facility. The vendor then replaces them with “new charcoal”–filled tanks. Permanent tanks are equipped with a control unit that allows them to be backwashed at the facility’s discretion. At intervals the carbon is replaced by the vendor or the facility. If the carbon tanks are rebedded at the facility, care must be taken to follow the local waste management guidelines as well as the manufacturer’s recommendations for personal protective equipment. Backwashing does not regenerate the carbon beds. It actually “fluffs” the carbon particles so that channels are removed and the total bed is once again available to contact water passing through it.
What is the action of the water softener?
A water softener is a device located after the carbon tanks that exchanges ions in the water. Water hardness is caused primarily by calcium and magnesium ions. A water softener exchanges calcium and magnesium ions for sodium ions on a milliequivalent-for-milliequivalent basis. Other positively charged ions, such as aluminum, are also removed by the water softener. For each calcium ion removed, two sodium ions are added. The sodium is later removed by the RO system. Permanent softeners have a concentrated brine tank that holds the sodium chloride and controls for on-site regeneration of the softener.
If the feed water is very hard, a softener will remove most of the calcium and magnesium before further treatment. If a deionizer is used downstream, the softener will reduce the divalent ion load presented to the deionizer resin bed and prolong its life. If the subsequent treatment is RO, the removal of calcium and magnesium by the softener may result in higher-quality product water and longer RO membrane life. If a softener was not part of the water treatment system, calcium could potentially build up on the RO membranes and decrease their effectiveness.
What problems occur with the use of water softeners?
If the raw water is very hard, considerable sodium is substituted in the exchange for calcium and magnesium. Municipal water supplies often vary seasonably or even during a single day if multiple sources are used.
There are two types of softeners: portable exchange and permanent. Portable exchange units are provided ready for use by the vendor. Regeneration of the media resin is performed by the vendor at a central facility.
There are no online monitors that will indicate “hard” or “soft” water, but commercial test kits for total hardness are available and are quite reliable. The degree of hardness of both source water and product water should be determined each day. Total hardness is measured post softener and in grains per gallon (gpg) or parts per million (ppm). This will indicate the need for the regeneration cycle, as well as any softener malfunction.
What is reverse osmosis?
RO represents the ultimate in ultrafiltration and is the most effective method of treating water used in dialysis. The RO process removes most contaminants left in the water by the pre-RO treatment systems, including bacterial endotoxins and other contaminants. The RO process involves the movement of water under high pressure across a semipermeable membrane. The dissolved solutes or contaminants will form on the feed side of the membrane and the pure water will form on the product side of the membrane. The product water will be virtually free of dissolved solutes and microorganisms. It is expected that the water going through the membrane will have a rejection rate of at least 80%. The product or purified water will then be sent to a holding tank, where it will be stored before use.
How are organic compounds processed by the membrane?
Organic compounds have no net charge and are not electrically repelled but are physically screened by the membrane. Almost all particles of molecular weight greater than 200 Da are rejected. This includes bacteria, viruses, and pyrogens.
What types of membranes are used for reverse osmosis?
Membranes for RO use must be (1) freely permeable to water, (2) highly impermeable to solutes, and (3) able to tolerate very high operating pressures. Desirable characteristics include tolerance to a wide range of pH and temperature and resistance to attack by bacteria and by chemicals, such as chlorine.
Membranes in general use include (1) cellulose, (2) aromatic polyamide, (3) thin-film composites, and (4) high-flux, chlorine-resistant polysulfone.
• Cellulose acetate membranes have high water permeability but poor rejection of low molecular weight contaminants. Range of pH tolerance is limited; the membranes degrade at temperatures greater than 35°C (95°F) and are vulnerable to bacteria. They are relatively inexpensive.
• Polyamide membranes have wide pH tolerance and are more resistant to bacterial action and to hydrolysis than are cellulosic membranes. They are very susceptible to degradation by free chlorine.
• Thin-film composites are expensive. The supporting layer is usually a porous polysulfone. Fixed to this is a thin, dense, solute-rejecting surface film such as polyfurane cyanurate or a polyamide. Composite membranes have better water flux and better solute rejection than cellulose acetate. They are less subject to compaction and bacterial action.
• Chlorine-resistant polysulfone membranes have a very long service life. They tolerate a wide span of pH and temperatures. Water flux is high. They differ from other membranes in that if divalent ions are present in the feed water, rejection of monovalent ions is sharply reduced. Therefore it is essential that the feed water be softened or deionized before entering the RO unit.
What configuration of reverse osmosis modules is used?
Module design must include such features as a large membrane surface area, a tolerance for very high pressure (up to 500 psi), good flow characteristics, and a low pressure drop. Configurations in use for hemodialysis water are (1) the spiral-wound or spiral-wrap (Fig. 8-1) and (2) hollow-fiber modules.

Figure 8-1 Spiral-wrap reverse osmosis module.
Spiral-wound units consist of two layers of membrane with a fabric material fastened between them, sandwich fashion. The fabric material is the product carrier. The membrane-sandwich sheet, along with a plastic mesh separator, is wrapped in a spiral around a central perforated tube in a manner somewhat similar to that of an old-style coil dialyzer. Feed water under high pressure enters one end of the unit and flows along the channels provided by the plastic mesh; some water is forced by the hydraulic pressure through the membrane. The central fabric conducts this filtered water to the central tube, from which it emerges as product water.
In hollow-fiber units the membrane is formed as capillary fibers of 80 to 250 mm inside diameter. Several thousand of these fibers are bundled inside a high-pressure cylinder. Pressurized feed water surrounds and permeates the hollow fibers, forming the product water inside the capillary lumina. The small internal diameter of the hollow fibers can contribute to plugging and reduced permeate flow.
What are special advantages of reverse osmosis over other types of water treatment?
RO has several advantages, including the following:
• Bacteria, viruses, and pyrogen materials are rejected by the intact membrane. In this respect RO water approaches distilled water in quality.
• Available units are relatively compact and require little space. They are well suited to home dialysis.
• In average use, the membrane has a life of a little more than one to two years before replacement is necessary.
• Periodic complete sterilization of the RO system with formalin or other sterilant is practical.
What are disadvantages of reverse osmosis systems?
Disadvantages of RO systems include the following:
• The membranes have a limited service life. For instance:
¡ Cellulose acetate membranes have limited pH tolerance. They degrade at temperatures greater than 35°C (95°F). They are vulnerable to bacteria. They eventually hydrolyze.
¡ Polyamide membranes are intolerant of temperature greater than 35°C (95°F). They have poor tolerance for free chlorine.
¡ Thin-film composites are intolerant of chlorine.
¡ High-flux polysulfones require softening or deionization of feed water to function properly.
• As with hemodialysis membranes, leaks are possible. Continual monitoring of product water flow rate and conductivity is necessary.
• Product water is 25% to 50% of feed water. The remaining 50% to 75% goes to waste, a matter of economic and environmental concern.
• The membrane must be kept continually wet throughout its entire life. The flow cannot simply be stopped and the unit filled with water; bacterial growth, hydrolysis of the membrane, and pyrogen production are likely to result. When not in operation, the unit should be held in a sterilant-filled state.
• Chloramines (oxidant compounds formed from the reaction between chlorine and ammonia used as bactericidal agents in some city water supplies) are nonionic and freely cross the RO membrane. Anemia resulting from chloramines has occurred in some dialysis patients. A carbon filter should always be used ahead of an RO system to remove any chloramines.
• To meet peak flow needs in large hemodialysis facilities, a reservoir or holding tanks for processed water from the RO unit may be necessary. The water is recirculated in a continuous loop from RO unit to tanks and back to prevent stagnation. The tanks and plumbing are sites for potential microbial growth and endotoxin formation. Tank design is important in minimizing contamination. A steeply rounded or conical tank bottom with the drain port at the extreme low point ensures complete emptying. The reentry port should be near the top and use a special nozzle to spray the underside of the cover. This prevents water droplets from forming on the cover, and the cascade of water down the sides prevents the collection of stagnant water. The top should have a microbial filter in the air vent. This design also provides excellent sterilant contact during chemical disinfection and complete flushing away of sterilant at “rinse-out.” Chlorine or iodine may also be metered into the system between the RO unit and the tanks to control the growth of organisms (Fig. 8-2).
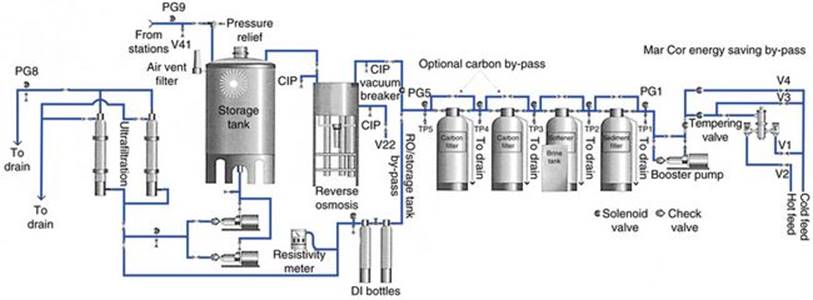
Figure 8-2 Recirculating loop water treatment system with holding tank.
(Courtesy Mar Cor Services, Harleysville, Pa.)
What is deionization?
DI refers to the removal of ionized minerals and salts from a solution, in this case, the feed water. Positively charged ions are exchanged by the resin beads for hydrogen ions, and negatively charged ions are exchanged to form hydroxide ions (Fig. 8-3). The hydrogen and hydroxide ions formed as a result combine to create water molecules. Deionizers produce water of high ionic purity, but they do not remove bacteria or pyrogens. Indeed, deionizers often make the quality of water worse in terms of bacteria and endotoxin content; the resin bed provides an environment conducive to bacterial proliferation. It is prudent to follow deionization equipment with submicron filtration or a UF unit (Fig. 8-4).

Figure 8-3 Schematic diagram of two-bed deionizing system.

Figure 8-4 Direct feed water treatment system to produce ultrapure water.
(Courtesy Mar Cor Services, Harleysville, Pa.)
How is water quality monitored with the use of a deionizer?
It is imperative that some type of monitor be installed to ensure the chemical quality of the product water. Deionizer water quality values are expressed in resistivity units. The AAMI guidelines state that product water should not be allowed to go below 1 MΩ resistance; at that point the tanks should be exchanged.
What problems occur with deionizers?
The following are several problems with deionizers to watch for:
• An initial problem is obtaining the maximum flow rate needed. As with softeners, proper size of the DI set is critical. Peak and normal operating flow rates and operating line pressures should be determined. The user then should look at the operating specifications for a variety of tank sizes and select the size that best meets the facility’s needs, taking account of the pressure drop across the DI set. Pressure indicators before and after this subsystem are advisable so that the difference in pressure can be easily determined.
• Total ion content of the feed water is a problem; only a finite quantity of ions can be removed by a resin bed of given size. Service life of the deionizer depends on water composition and volume. If a DI unit is positioned ahead of an RO unit, its service life will be short. It will be processing water of high ionic content while the RO unit will serve primarily as a bacterial and endotoxin screen. If the DI unit is located downstream from the RO device, the DI then becomes a “polisher.” It also increases chances of microbiologic contamination. It is recommended that a submicron filter or an ultrafilter be placed downstream.
• Resin beds tend to exhaust suddenly. A parallel bypass installation is necessary so that switchover can be made while the exhausted tanks are replaced. The water in tanks that are standing idle will be stagnant. Provision for flushing a reasonable volume to the drain should be part of the system. The volumetric capacity of deionizers (gallons of water passing through the tanks) is rated in gpg of total dissolved solids (TDS), expressed as calcium carbonate. (Note: 1 gpg approximates 17.1 mg/L CaCO3.) Rated capacity of the deionizer divided by the TDS of the feed water will give an approximation of the volume of water that may be treated before the unit exhausts. Online, continuous readout resistivity meters should be positioned to monitor the effluent water. When the resistance degrades to 1 MΩ/cm, the tanks should be exchanged (an AAMI standard).
• Usually the anion and cation resins exhaust at different times. If the tanks are used to exhaustion, ions previously removed may be released, possibly in a concentration greater than that of the feed water. The water may become extremely acidic or extremely alkaline, depending on which resin exhausted first. This situation may be hazardous to patients or equipment.
How is ultraviolet light used in treating water?
Ultraviolet (UV) light is a form of radiation that penetrates the cell walls of microorganisms and destroys them by altering their deoxyribonucleic acid (DNA). In the dialysis water treatment system, the UV light source is housed in a clear protective quartz sleeve. It is placed so that water can pass through a flow chamber, where it is exposed to intense UV radiation. It is important that the water flow not be too turbulent and that the water be free of suspended particles. UV light passes more easily through clear translucent fluids. Cloudy liquids make the UV light more difficult to penetrate and could potentially allow microbes to hide behind the suspended particles and not be eliminated. The UV light does not destroy endotoxins.
What degree of water purity is required for hemodialysis?
The AAMI developed a set of water quality guidelines that is recognized as the U.S. national standard. The standard now applies not only to chemical or inorganic contaminants but to microbiologic contaminants as well. These requirements are shown in Table 8-1 along with the adverse effects of exposure. The AAMI list of contaminants has been expanded to include antimony, beryllium, and thallium due to changes in the Safe Water Drinking Act.
Table 8-1 AAMI Water Quality Guidelines*
|
Water contaminant |
AAMI suggested maximum level (mg/L) |
Adverse effects from exposure† |
|
Aluminum |
0.01 |
Anemia, bone disease, neurologic changes |
|
Antimony |
0.006 |
Nausea/vomiting |
|
Arsenic, lead, silver |
0.005 each |
|
|
Bacteria |
<200 CFU/mL |
Hypotension, nausea/vomiting |
|
Beryllium |
0.004 |
Bone damage |
|
Cadmium |
0.001 |
Nausea/vomiting, diarrhea, salivation, sensory disturbances, kidney/liver/bone damage |
|
Calcium |
2 (0.1 mEq/L) |
Nausea/vomiting, headache, muscle weakness, tachycardia, hypertension, abnormal bone mineralization, soft tissue calcifications, pancreatitis |
|
Chloramines |
0.1 |
Hemolysis, chest pain, arrhythmias, nausea/vomiting |
|
Chlorine |
0.5 |
|
|
Chromium |
0.014 |
Liver damage |
|
Copper, barium, zinc |
0.1 each |
Chills, flushing, headaches, projectile vomiting, hypotension, anemia, liver damage, pancreatitis |
|
Endotoxin |
<2 EU/mL |
Hypotension, nausea/vomiting |
|
Fluoride |
0.2 |
Chest pain, nausea/vomiting, hypotension, headache, bone disease |
|
Magnesium |
4 (0.3 mEq/L) |
Nausea/vomiting |
|
Mercury |
0.0002 |
Kidney damage |
|
Nitrate (N) |
2 |
Hemolysis, hypotension, nausea/vomiting, weakness, confusion |
|
Potassium |
8 (0.2 mEq/L) |
|
|
Selenium |
0.09 |
Fatigue, irritability, hair/nail loss, kidney/liver damage |
|
Sodium |
70 (3 mEq/L) |
Increased thirst, nausea, headache, hypertension, pulmonary edema, seizures, coma |
|
Sulfate |
100 |
Metabolic acidosis, nausea/vomiting |
|
Thallium |
0.002 mg/L |
Liver/kidney damage |
* The physician has ultimate responsibility for determining the quality of water used for dialysis.
† Acute symptoms in italics.
From Vlchek DL, Burrows-Hudson S: Quality assurance guidelines for hemodialysis devices, Washington, DC, February 1991, U.S. Department of Health & Human Services, U.S. Food and Drug Administration; U.S. Environmental Protection Agency: Drinking water contaminants, from http://www.epa.gov/safewater/mcl.html; Association for the Advancement of Medical Instrumentation, Arlington, Va, 2001.
What problems are there in handling very pure water?
As water is treated increasingly near its pure state, its energy level also increases. Such pure water very quickly reacts chemically with materials it contacts. Only pipe or tubing of medical-grade stainless steel, polyvinyl chloride (PVC), or one of the new inert materials may be used to carry the product water. Tanks must be of such material. If exposed to air, ultrapure water will quickly absorb and react with carbon dioxide.
What problems are there with bacteria and pyrogens in water treatment?
The maximum level of bacteria in the water used to prepare dialysate and reprocess dialyzers must be less than 200 colony-forming units (CFU). The AAMI action level is 50 CFU for bacteria in water to prepare dialysate. New membranes are much more porous to water, solutes, and suspended matter. Transmembrane movement is bidirectional, relative to pressure and solute concentration gradients. Proper prefilters with an RO unit or DI with submicron postfiltration will in most instances meet the standard. Bacteria proliferate on filter surfaces, carbon tanks, softener and DI resin beds, and the feed water surface of the RO membrane. A regular schedule of backflushing with an approved sterilant must be used to minimize bacterial growth in all components of the water treatment system. The sterilant must, of course, be thoroughly rinsed from the system before water is used for patients. Chemical sterilization kills bacteria but does not destroy them, and actually fixes some of the protein and polysaccharide components and endotoxins. Copious backflushing is needed to wash this debris away from the collecting surfaces.
A majority of facilities use bicarbonate-containing concentrate in their fluid-proportioning systems. Many facilities use dialyzers with high-flux membranes, along with controlled UF devices.
Bicarbonate concentrate, when stored, supports proliferation of endotoxin-forming microorganisms. Whether these originate from the water used to prepare the concentrate or from the bicarbonate powder, it is likely that more strict microbial and endotoxin limits will be necessary. For high-flux dialysis where backfiltration poses a problem, delivery of sterile, pyrogen-free fluid from the proportioning system to the dialyzer may become necessary.
How may microbiologic contaminants be further reduced?
The following three means are most commonly used to reduce microbiologic contaminants:
• Chlorine may be metered into RO product water. This is sometimes used in facilities that recirculate RO water through a holding tank system. However, the chlorine also produces problems.
• Submicron (0.05 mm) filters will stop passage of bacteria and viruses. Such filters must be replaced frequently and are expensive. They do not exclude all pyrogenic matter.
• UF will reject bacteria and endotoxins effectively. Initial installation is relatively expensive, but operation is economical. Sanitization is simple, and service life is good.
How is ultrafiltration used to remove bacteria and endotoxins?
UF membranes have an effective pore size of more than 0.001 mm. Pores of this size do not retard the movement of osmotically active solutes; hence less hydraulic pressure is needed for the transmembrane movement of water than is needed with RO membranes.
UF membranes are often called molecular filters; they filter suspended particles of molecular size rather than dissolved substances. The larger particles do not have the osmotic effect of dissolved solutes. There is little osmotic backpressure, compared with RO membranes, hence less need for high hydraulic pressure. However, these molecular filters reject bacteria, endotoxins, and endotoxin fragments that are thousands of daltons in size. Ultrafilters are available that exclude particles of 50,000 to 100,000 Da; in fact, an even tighter membrane of 1000 to 10,000 Da is available.
UF devices may be placed ahead of RO units to prevent bacterial growth or accumulation of particulate material on the feed water surface of the RO membrane. When used as the final step before delivery of product water to the proportioning system, UF will ensure its microbiologic quality.
What tests are done to maintain the water treatment systems?
Bacteria culturing. Bacteria culturing is performed to detect the presence of bacteria in the water. A colony count is typically read in 24 and 48 hours. Bacterial cultures are also performed on the dialysate. The maximum level of endotoxin in water used to prepare dialysate and reprocess dialyzers must not exceed the AAMI standard of 2 endotoxin units per milliliter (EU/mL). Testing is performed monthly. If a problem with bacteria is identified by positive cultures, testing should be conducted weekly until the problem is resolved.
Conductivity. Conductivity is verified on the feed and product water to make certain it contains the proper amount of ions. It can be measured with a pHoenix meter (which also measures pH and temperature). Conductivity may also be measured with a handheld meter, such as the Myron-L.
Resistivity. Resistivity determines the efficiency of removal of ions from water processed in a deionizer. Water with a high resistivity will have a low conductivity due to the low amount of ions in the solution.
Hardness test. This test detects the presence of calcium and magnesium in the water.
Total dissolved solids. TDS determines the total dissolved solids in water. TDS is the sum of all ions in a solution and verifies the effectiveness of the RO membranes. This can be checked with a handheld meter. The results are expressed in ppm.
What microbiologic standards apply to dialyzer reuse?
The microbiologic standards that apply to dialyzer reuse are defined in the AAMI Recommended Practice for Reuse of Dialyzers (RD47). The water used in reprocessing should have a bacterial count of less than 200 CFU/mL or an endotoxin level of less than 2 EU/mL. This also may be made stricter because of the problems with bicarbonate and with high-flux dialyzers. The action level for the total microbial count in the water is required to be 50 CFU/mL, with an action level for endotoxins of 1 EU/mL.
What kind of water processing is best for the individual dialysis unit?
The kind of water processing depends on the quality of available tap water and its solute content. Feed water should be analyzed on a regular basis for chemical and bacteriologic content and should meet the Environmental Protection Agency (EPA) drinking water standard. Product water—the final purified water used to prepare dialysis fluid—should meet AAMI and other applicable standards. Components of a system to meet these requirements may include the following:
• Initial sediment filter(s)
• Resin-type softener (water hardness checked twice daily)
• Activated carbon filter (two in series)
• RO unit (with continuous conductivity/resistivity monitoring of inflow and outflow water)
• DI unit (continuous conductivity monitoring of outflow, plus monthly bacteriologic, limulus test, and chemical analysis)
A complete system of this type will provide maximum purity water, approaching 18 MΩ/cm resistance. Thorough investigation is necessary to reach the desired purity of water in the most economic manner. Ongoing monitoring is essential to ensure its maintenance.
Where may information about available tap water quality be obtained?
State departments of health conduct regular and detailed analyses of public water supplies, except in Indiana and Wyoming, where the EPA has responsibility. The reports are available upon request and often, upon request, any periodic reports will be sent to the facility. The department of health may do an analysis of a specific water supply on request. Manufacturers of water treatment equipment and supplies seek to tailor their equipment to each individual dialysis facility’s needs. They may provide a detailed water analysis as part of their service.
Information on chemical content is usually given in ppm. This is equal to milligrams per liter. To convert to mEq/L, multiply milligrams per liter times valence and divide by molecular weight. For example, for calcium:
![]()
![]()
![]()
What cost factors are involved in establishing an adequate water treatment system?
Before setting a dollar figure on how much to spend, the facility should consult with a knowledgeable designer of dialysis facility water treatment systems and a reliable supplier/ installer. Facility needs, current and future, should be determined. Consideration should be given to each of the following factors:
• Peak volume needs
• Desired quality of product water (minimum should exceed AAMI standards)
• Expertise of the technical staff
• Cost of feed water
• Compliance with standards
• Type(s) of therapy to be delivered
• Ease of operation
• Maintenance requirements
Components listed above should be included only to achieve a particular goal, with the final objective of meeting or exceeding AAMI standards. If the source water is of very low mineral content, it may be possible to achieve 1 MΩ/cm product water by RO alone, or by DI alone, after appropriate filtration. Only the minimum number of components necessary should be used to meet or exceed AAMI standards.
Preparation of bicarbonate dialysate and high-flux dialysis may necessitate more stringent microbial control than is required by current AAMI standards and the 1991 Quality Assurance Guidelines.
What are the food and drug administration’s guidelines for water treatment equipment?
According to the Food and Drug Administration (FDA) guidelines, each premarket notification for a water purification component or system should include the information listed in Box 8-1. This helps the FDA determine whether the application has “substantial equivalence” to a water purification system already on the market. A copy of the guidelines can be obtained from the Center for Devices and Radiological Health’s Division of Small Manufacturers, International and Consumer Assistance.
![]()
Box 8-1 Factors Included in Premarket Notification for Water Purification Products
• Device name, including both the trade or propriety name and the classification name
• Establishment registration number, if applicable, of the owner or operator submitting the premarket notification
• The generic class (class 2) in which the device has been placed under the Federal Food, Drug, and Cosmetic Act and the appropriate panel
• A statement of the action taken by the registered manufacturer for special controls
• The Safe Medical Devices Act of 1990 (SMDA) requires all persons preparing a premarket notification submission to include (a) a summary of the safety and effectiveness information in the premarket information notification submission upon which an equivalence determination could be based, or (b) a statement that safety and effectiveness information will be made available to interested persons upon request
• Proposed labels, labeling, and advertisements sufficient to describe the water purification component or system, its intended use, and the directions for use (including maintenance, operation, cleaning, and troubleshooting), accompanied by a specific intended use statement and any warnings, contraindications, or limitations clearly displayed
• Statement comparing the water purification component or system to a legally marketed predicate device (one that was in commercial distribution prior to May 28, 1976, or one that has been cleared for marketing in the United States under Section 510[k] of the act)
• For a device or device labeling that has undergone a change or modification that could significantly affect the safety or effectiveness of the device, the 510(k) must include any additional supporting data to show that the manufacturer has considered the effects that the change or modification might have on the safety and effectiveness of the device
• Requirements are listed for these water purification components:
• Reverse osmosis (RO)
• Water softeners
• Carbon absorption beds
• Deionization (DI)
• Sediment and cartridge filters
• Ultraviolet (UV) disinfection unit
• Ultrafilters
• Auxiliary components
• Water storage tanks
• Additional requirements for water purification systems applications:
• Provide a description of the decision-making process used to meet the needs of the user.
• Describe the consequences of failure for each component and the required corrective action.
• Provide user manuals for each component of the system, as well as guidance for the installation, start-up, and maintenance of the system.
• Label each component in the system with the name and address of the supplier.
• Provide the results of leach testing and identify the chemical composition of any material that leaches from the system.
• Certify that the water produced by each purification system will meet or exceed current standards and regulations.
Modified from U.S. Department of Health & Human Services, U.S. Food and Drug Administration: FDA guidelines, May 30, 1997.